0412
SAR Management in pTx Sequence Design: The Impact of Electromagnetic-Field-Derived Virtual Observation Points1Imaging Centre of Excellence, University of Glasgow, Glasgow, United Kingdom, 2Department of Neuroradiology, University Hospital Erlangen, Erlangen, Germany, 3Siemens Healthineers, Erlangen, Germany, 4MR CoilTech Limited, Glasgow, United Kingdom, 5Institute of Radiology, University Hospital Erlangen, Erlangen, Germany
Synopsis
We compare two methods for estimating local SAR with virtual observation points (VOPs) in a commercial and a self-built 8Tx/32Rx head coil, respectively. The commercial coil relies on a constant safety factor that reduces the hardware power limits in each transmit channel, where the self-built coil derives the VOPs from coil electromagnetic field (EMF) simulations. We show the use of both coils in vivo with MPRAGE using Universal and subject-specific pTx pulses. The EMF-based VOPs, used with the self-built coil, resulted in a lower local SAR estimate for a similar image quality, providing more flexibility in pulse sequence design.
Introduction
Virtual observation points (VOPs) [1] provide a common method for evaluating local specific absorption rate (SAR) in parallel transmit (pTx) MRI. The Eigenvalue clustering method defines an overestimation with respect to the “worst case”shim configuration (in the local SAR sense) of pTx channels. It has been suggested to include as many electromagnetic field (EMF) body model simulations at as many positions as computationally feasible in the VOPs to account for potential local SAR hotpots [2]. Nevertheless, commercial pTx coils for 7T are typically supplied without the EMF-based VOPs and instead apply a constant safety factor for local SAR supervision, which can be overly conservative. In this abstract we compare the use of EMF-based VOPs in a self-built 8Tx/32Rx head coil to constant safety factor VOPs in a commercial 8Tx/32Rx coil. We investigate the local SAR values for both coils using Universal Pulses (UPs) [3] and subject-specific FOCUS pulses [4] in healthy volunteers.Methods
In Vivo pTx ExperimentsB0 and B1+ maps were acquired from 10 healthy subjects on two 7T scanners (MAGNETOM Terra Siemens, Erlangen, Germany). One scanner was equipped with a commercial 8Tx/32Rx coil (Nova Medical, Wilmington,MA,USA); the other scanner with a self-built dual-mode 8Tx/32Rx coil [5],[6]. For each coil, volunteer maps were used to generate non-selective UPs [3] for 5° excitation (using a SPINS trajectory [7]) and for inversion (using kT-points [8]). Furthermore, subject-specific FOCUS excitation and inversion pulses were designed [4]. These pulses were used in an MPRAGE sequence (TE=2.28ms/TR=3000ms/TI=1100ms/matrix=250x224x160/1mm3isotropic) in one subject at each 7T site. Single-transmit comparisons were made using a standard adiabatic hyperbolic secant inversion and circularly polarized (CP) 5° excitation pulses.
VOP Shim Configurations Comparison
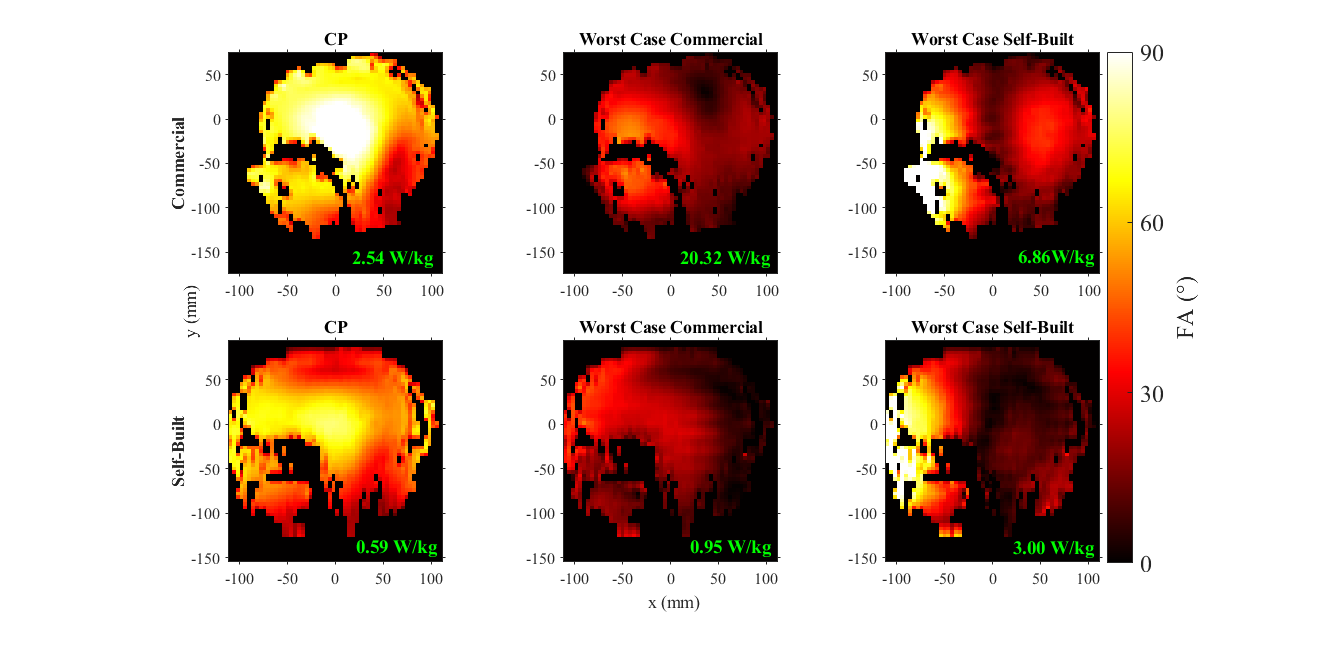
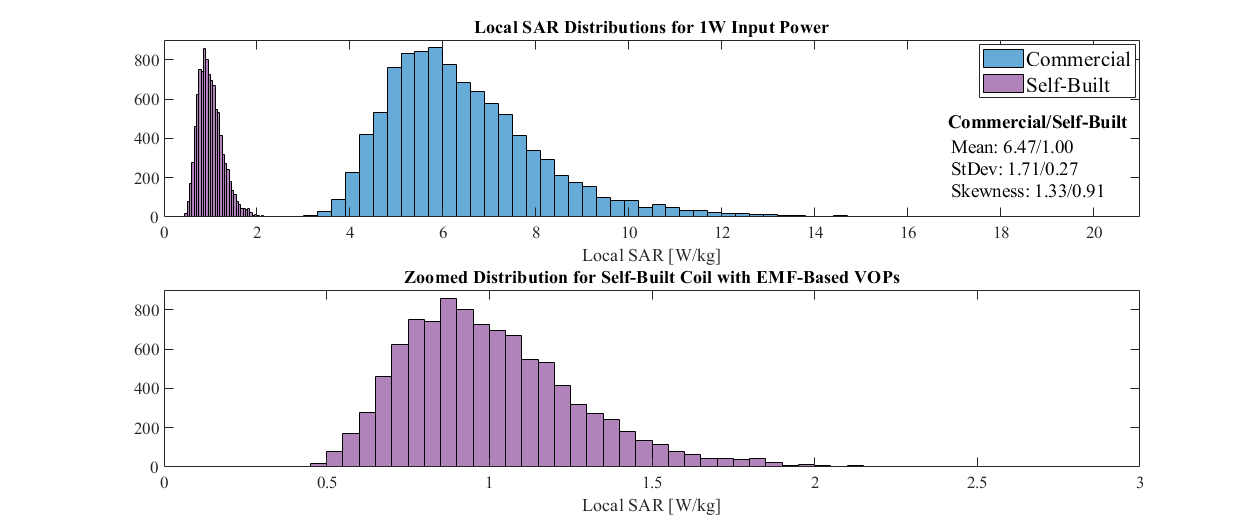
For all MPRAGE scans, we exported B0/B1+ maps, system calibration measurements, SAR measurements, and FOCUS pulses. For each coil’s set of VOPs, the “worst case” shim configuration (in the local SAR sense) was used to calculate the maximum local SAR given 1W input power. We used the same calculation for CP mode and the opposite coil’s “worst case” configuration. Flip-angle maps for these shim configurations were simulated for each coil. Ten thousand random shim configurations were also generated and 1W local SAR was calculated in both coils.
Overestimation Factor in EMF VOP Model
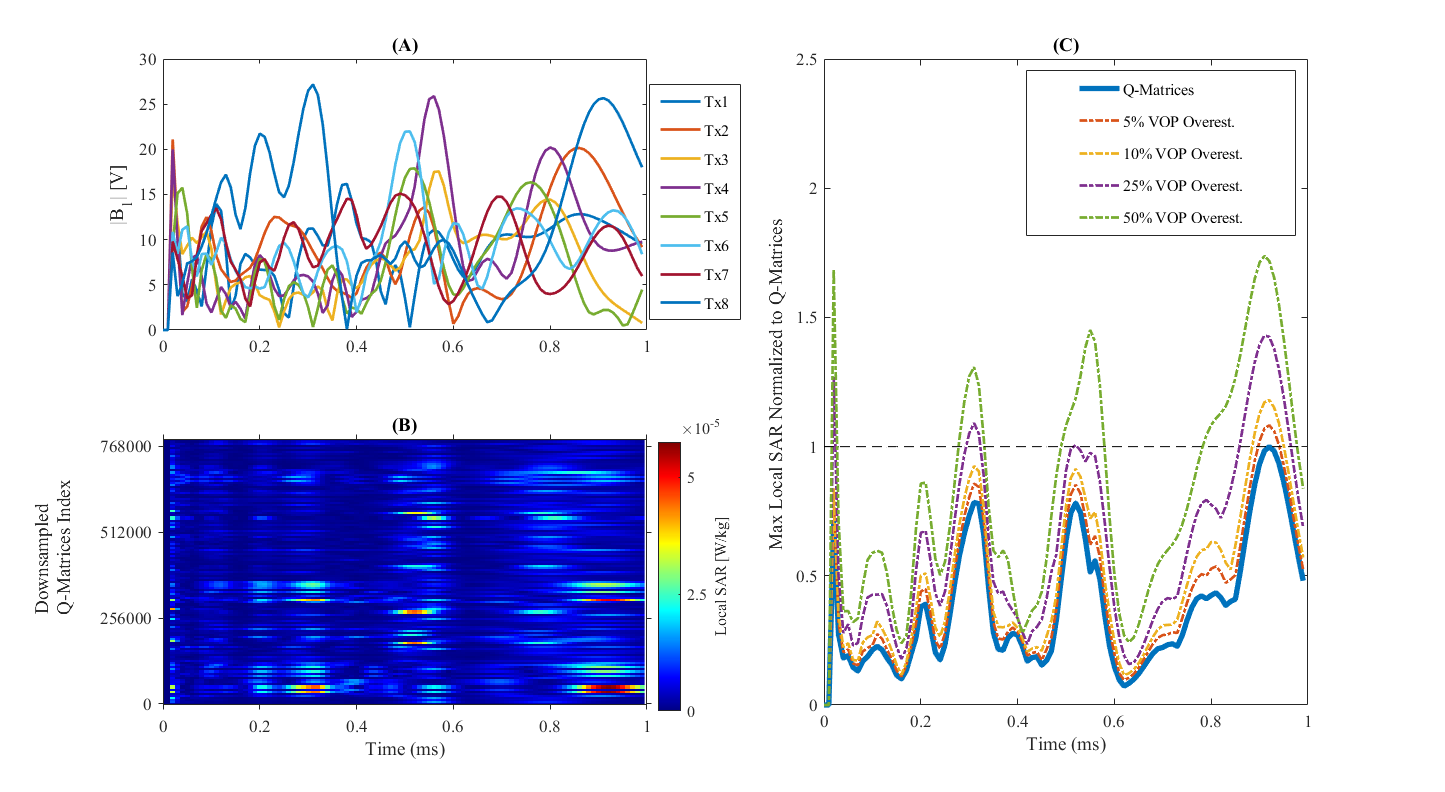
The constant safety factor for commercial coil VOPs is the channel power limit, multiplied by ~2.5. In the self-built coil, the safety factor varies [1] in relation to the “worst case” configuration. To understand varying degrees of overestimation with the EMF-based VOPs, time varying instantaneous maximum local SAR was computed for self-built coil's UP excitation pulse. This was done for uncompressed coil model Q-matrices [9], consisting of 9 concatenated human body models [6]. The UP local SAR was also calculated for 5%/10%/25%/50% “worst case” overestimation VOP compressions. The self-built coil has been approved by local ethics and safety committees for operation in IEC normal operating mode using 10% overestimation in VOP compression.
Comparison of Calculations and Scanner SAR Measurements
Finally, we compared UPs and FOCUS pulses for both coils’ VOP models with MPRAGE experimental data. We calculated local SAR contributions of each pulse (excitation or inversion) across VOP models and all experimental combinations used in MPRAGE. Since the same sets of MPRAGE scans were performed with both coils, SAR estimates can be compared to scanner predictions and real-time measurements for both VOP models.
Results
Figure 1 shows simulated flip-angle maps for both coils with three shim configurations along with the corresponding 1W input SAR. The flip-angle distributions suggest a similar EMF for both coils, which would generate similar local SAR hotspots.Figure 2 displays 1W maximum local SAR for both coil VOPs for CP, "worst-case", and 10,000 random shims.
Figure 3 shows instantaneous local SAR for the EMF-based VOPs using the self-built coil’s UP excitation (3A). Figure 3B plots time-resolved SAR for MPRAGE using a subset of the uncompressed EMF Q-matrices; different VOPs dominate local SAR contribution for various pulse time points. Figure 3C plots time varying local VOP SAR relative to the Q-matrices’ SAR. The VOP SAR is never underestimated compared to the full EMF model.
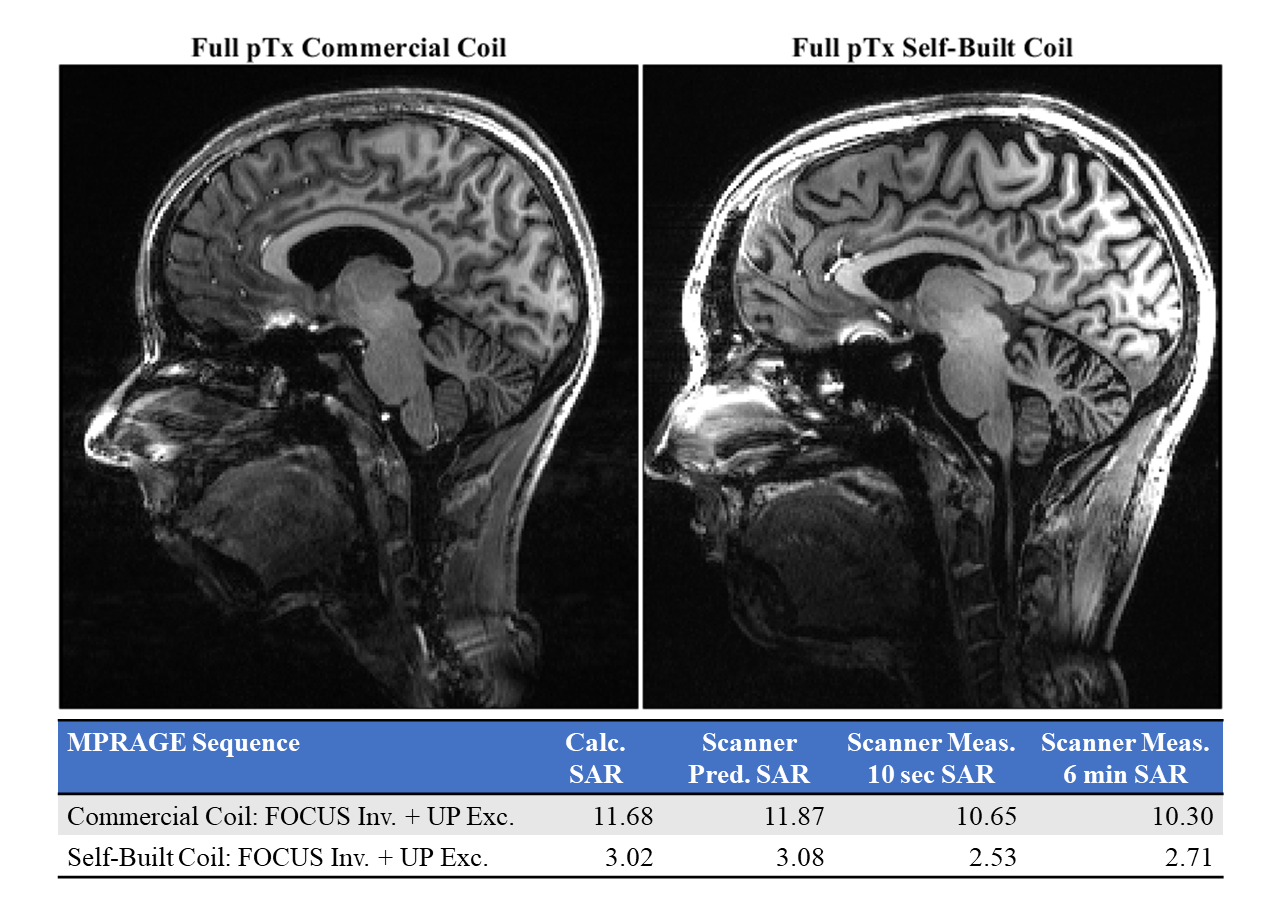
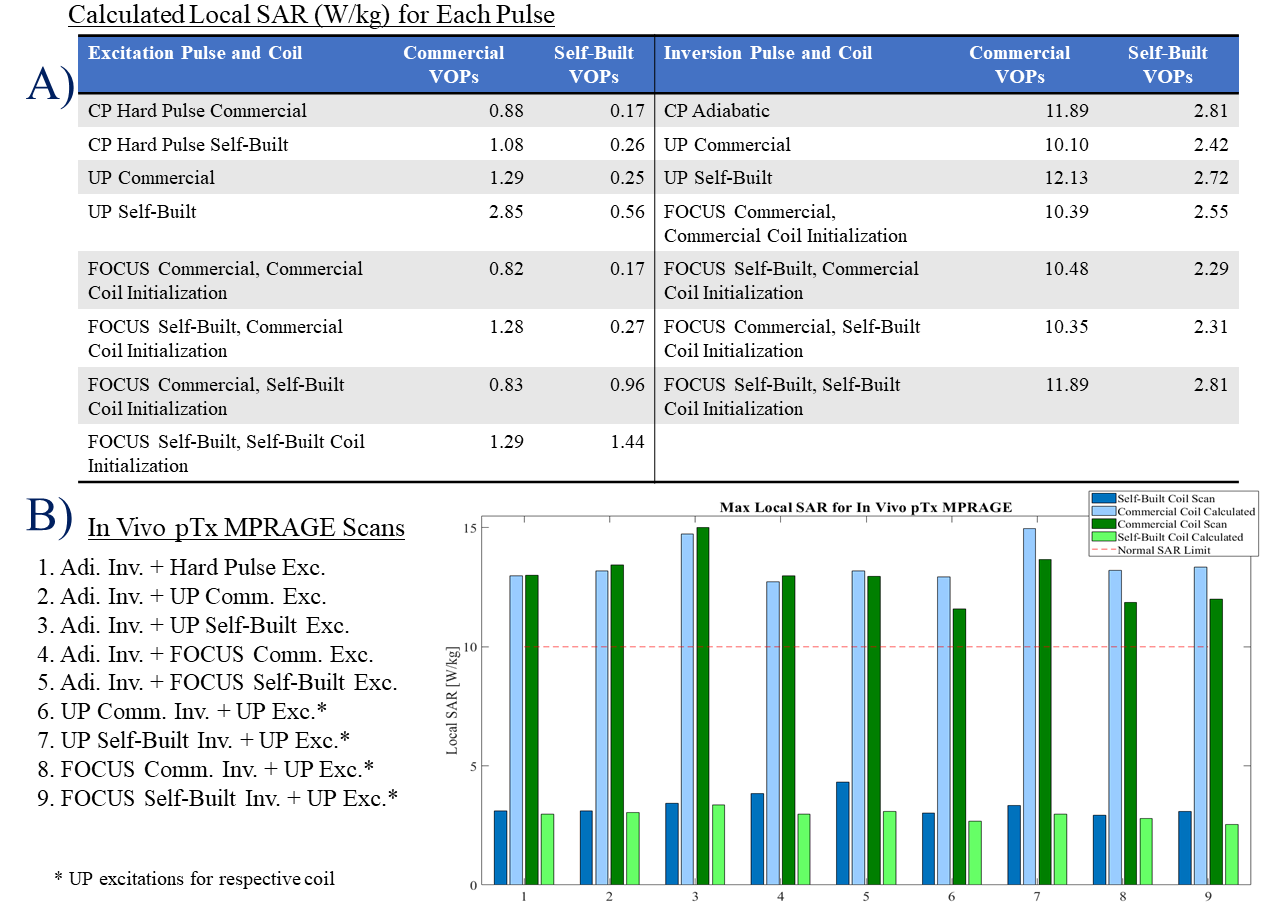
Figure 4 shows both subjects' pTx MPRAGE images and lists the calculated and scanner provided SAR.
Figure 5 lists local SAR calculations and scanner measurements for the pTx pulses used in vivo. For the same scans, the commercial coil required operation in IEC first level mode while the self-built coil, normal mode.
Discussion & Conclusion
Comparing the VOPs’ simulated and experimental performance in both coils, the commercial coil VOPs provide SAR estimates that are highly conservative compared to estimates from VOPs based on anatomical models. The self-built coil's EMF-based VOPs are closer to the modeled SAR deposition from the uncompressed Q-matrices, thus allowing lower IEC level scanning. Nevertheless, even with EMF-based VOPs, safety margins are required to allow variation in the subjects' anatomy and position in the head coil. For the current study, this safety margin was provided by the VOP compression setting and the restriction to the IEC normal mode limit of 10W/kg for local SAR in the head. Larger scale EMF simulations are required to explore the effect of subject anatomy and to optimize the use of VOPs for wider application.Acknowledgements
The authors would like to extend their thanks for Dr. Rene Gumbrecht (Siemens Healthcare, Erlangen, Germany) for helpful discussions on the SAR monitoring system of the 7T MAGNETOM Terra. They also wish to thank Rosemary Woodward, Tracey Hopkins, and Dr. Sarah Allwood-Spiers (NHS Greater Glasgow & Clyde,UK) for assistance with collection of the volunteer B0 and B1+ maps used in UP design. Finally we thank Dr. Andrew Tyler Morgan (NIMH, NIH, Bethesda,MD,USA) for last-minute help revising this abstract.References
[1] G. Eichfelder et al., MRM 2011. [2] E. Kopanaglu et al., MRM 2020.[3] V. Gras et al., MRM 2017.[4] J. Herrler et al., MRM 2020 .[5] G. Shajan et al., ISMRM 2019.[6] S.N.Williams et al., ISMRM 2020.[7] S. Malik et al., MRM 2011.[8] M. Cloos et al., MRM 2012. [9] I. Graesslin et al., MRM 2012.
Figures