0366
Radiofrequency-Induced Heating of Broken, Damaged, and Abandoned Leads1IT'IS Foundation, Zurich, Switzerland, 2Department of Physics, Aristotle University of Thessaloniki, Thessaloniki, Greece, 3ITET, ETH Zurich, Zurich, Switzerland, 4FDA, Silver Spring, MD, United States
Synopsis
To demonstrate the potential enhanced heating of abandoned (capped), damaged, or broken leads, we estimated in-vitro the deposited lead-tip power for a generic active implantable medical device (AIMD), intact and with wire breaks at regular intervals. We studied break size, a cut and capped lead, and a second wire parallel to the broken wire. The deposited lead-tip power enhancement was up to 30-fold over the intact lead. The presence of a nearby intact, or even broken, wire reduced this enhancement factor to ~3-fold. This shows the risk of extending MR-conditional labeling to broken, damaged, abandoned, or cut AIMD leads.
Abstract
To demonstrate the potential enhanced heating of abandoned (capped), damaged, or broken leads, we numerically estimated the deposited lead-tip power for a generic AIMD with a flexible lead, intact and with wire breaks at 10 cm intervals, under isoelectric conditions at 64 MHz in tissue simulating medium. We studied the effect of the break size (wire gap width), the behavior of a cut and capped lead, as well as the presence of an intact wire parallel to the broken wire. We experimentally validated the results of the configurations with maximum deposited lead-tip power. The enhancement of the deposited lead-tip power for the broken leads were up to 30-fold higher than the intact lead. The presence of a nearby intact, or even broken, wire reduced this enhancement factor to ~3-fold over the intact lead. The results demonstrate that care must be taken when extending MR-conditional labeling to broken, damaged, abandoned or cut leaded devices.Background
Patients with long conductive implants undergoing magnetic resonance (MR) examinations bear the additional risk of interaction of the implant with the radiofrequency (RF) fields induced in the body by the MR system. The risk is assessed for potential variation in the implant configuration, lead design, lead trajectories, tissue environment, and incident field (RF coil, imaging landmark, etc.), including consideration of the measurement and simulation uncertainties. However, individual wires of a lead may already be broken before, or break during implantation, as some unresponsive channels may be tolerated by the implantation protocol. Wire breakage may also occur spontaneously over time, and broken, retained, or abandoned leads may result from subsequent surgeries, where leads may be re-positioned, cut, or simply unplugged rather than removed. The proximal end of the abandoned lead may be capped (isolated from the tissue) or left in contact with the tissue. The presence of broken, damaged, abandoned, or cut AIMD leads leaves patients ineligible for MR examinations at some sites, while at others it is allowed by the expert if mitigating steps are taken (e.g., reduced scan intensity or time). To our knowledge, there is no clinical study to date of the MR safety effects of AIMD leads with broken wires.Method
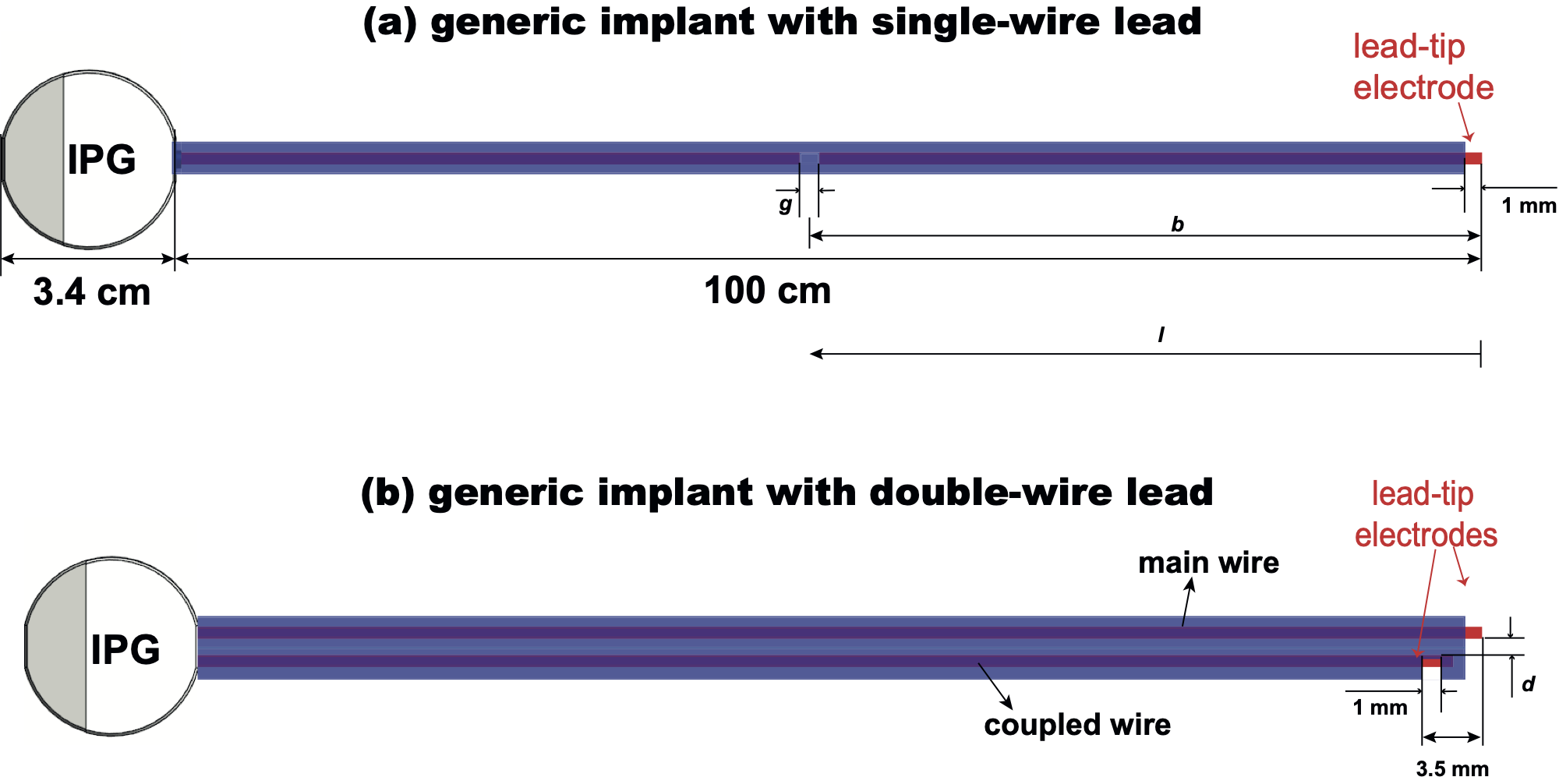
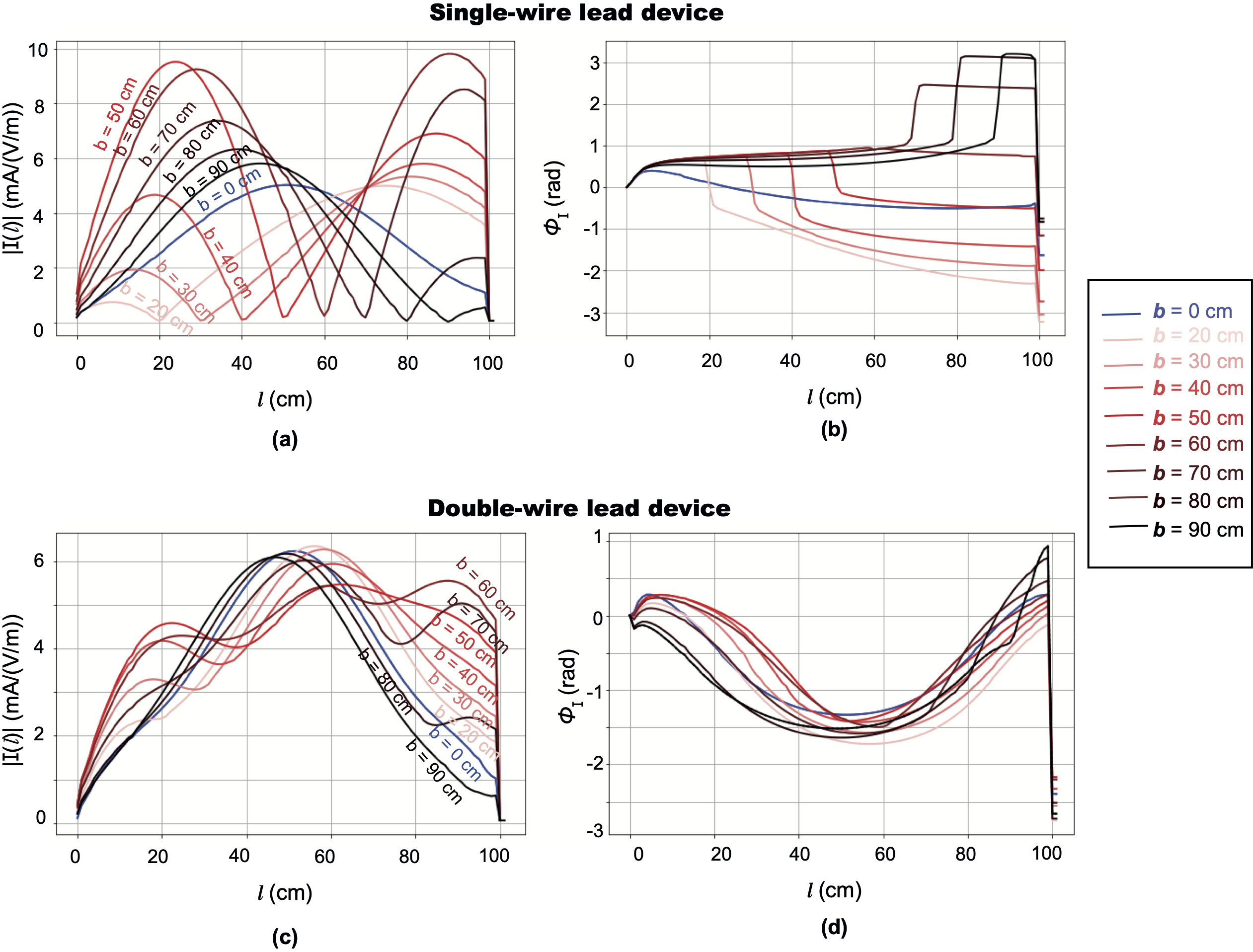
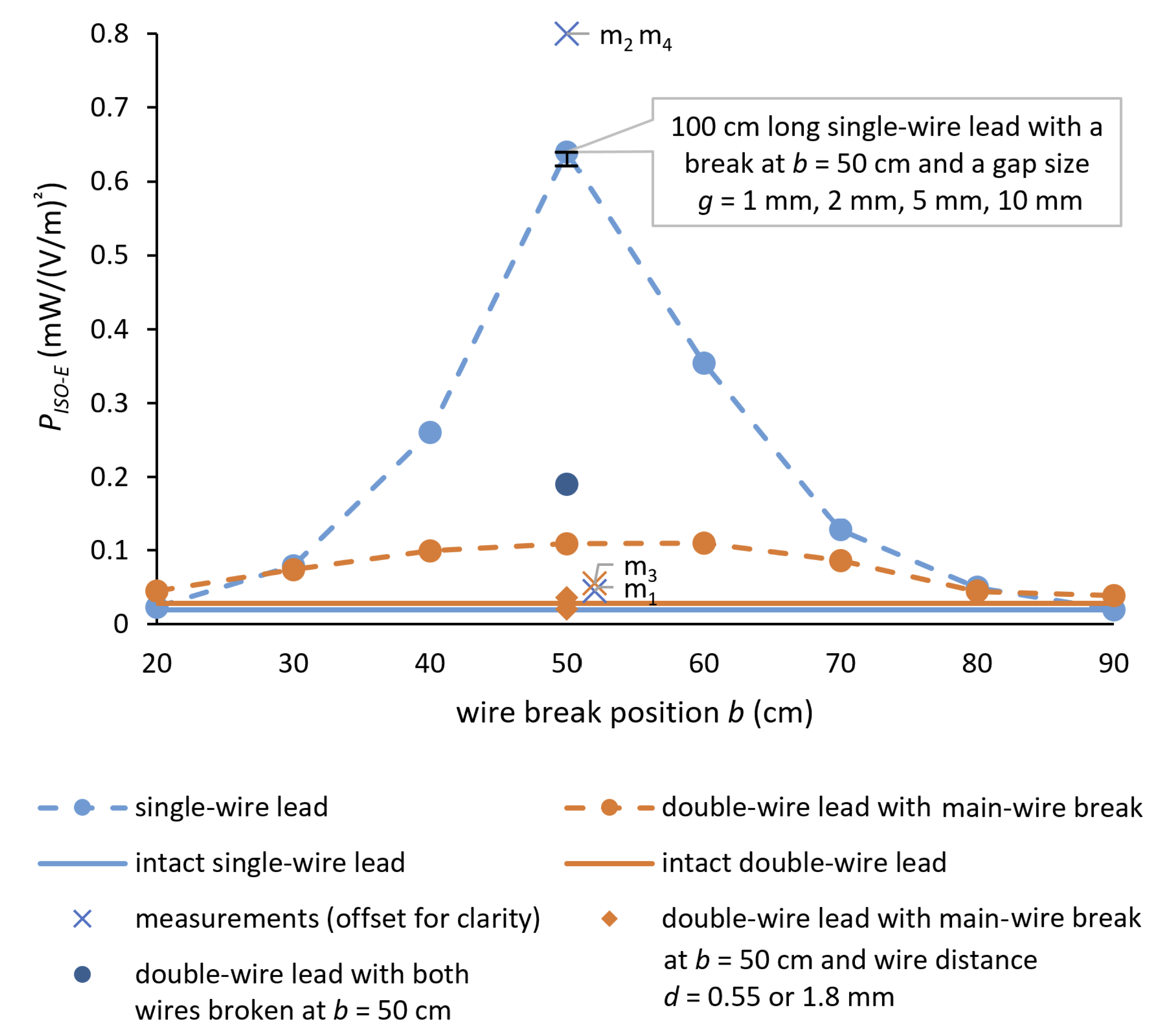
We defined a generic AIMD with a metallic IPG and a 100 cm single-wire lead, and performed finite-difference time domain (FDTD) simulations at 64 MHz in homogeneous tissue simulating medium to derive the RF-induced SAR distribution near the lead-tip, the current distribution along the lead, and the transfer function. We added a 1 mm break at 10 cm intervals along the wire. For the single-wire lead with a wire break at 50 cm, which represented the highest deposited lead-tip power, we varied the gap sizes up to 10 mm. To study the influence of a nearby (coupled) wire, we created a double-wire lead with a wire spacing of 0.55–1.8 mm. We also checked the effect of breaks in both wires at the worst-case length. For experimental validation, we manufactured leads corresponding to the single-wire intact lead, single-wire broken lead at worst-case break location, double-wire lead with one wire broken, and double-wire leadwith both wires broken, and characterized their deposited lead-tip power via radiated tests.Results
The deposited lead-tip power under iso-electric conditions was ~30 times higher than for the intact single-wire lead when the wire break was positioned at the half-wavelength distance (i.e., lead with a wire break at 50 cm from the tip). By adding an extra intact wire, or surprisingly even an extra broken wire, the RF-induced deposited lead-tip power enhancement decreased for the single-wire lead from >30-fold to less than 3-fold. This enhancement decreased to less than 4 times when we placed an intact wire parallel to the broken wire. By changing the spacing between the broken and unbroken wire, the enhancement factor varied by a factor of ~3. When the coupled wire was also broken at 50 cm, the deposited power increased by ~2 compared to the case when only the main-wire was broken at 50 cm, but was still ~3 times lower than for the broken single wire. Surprisingly, a parallel lead reduced the enhancement to less than 7 times that of the intact case even when the wire was broken. All numerical results were successfully experimentally validated within the combined uncertainty.Conclusions
This work demonstrates the potential for dangerously large RF-induced heating of abandoned (capped), damaged, or broken leads when compared to intact leads. The maximum enhancement of the in-vitro deposited lead-tip power of a generic AIMD due to a wire break reached 30-fold compared to the intact lead. Due to electromagnetic coupling, the presence of a nearby intact, or even broken, wire was seen to reduce the potential enhancement significantly. Our experimental results confirm that a capped abandoned lead behaves the same as a broken lead with the same length from the lead-tip to the break point. The numerically extracted results were successfully validated by experiments within the combined uncertainty. These potential heating enhancements should becarefully considered, together with the probability of tissue damage and/or the use of a pre-scan diagnostic, such as an impedance check, when performing risk assessment for MR examinations or device labeling.Acknowledgements
This work was supported by the EMPIR grant 17IND01 MIMAS, which is co-funded by the European Union's Horizon 2020 research and innovation program and the EMPIR participating states. The authors would like to thank Dr. Arya Fallahi from IT'IS Foundation and Dr. Sabine Regel from SR Scientific GmbH for their insightful comments and careful reading, and Dr. Maurice Cox from NPL for his review of the confidence interval estimation.
Disclaimer: The mention of commercial products, their sources or their use in connection with material reported herein is not to be construed as either an actual or implied endorsement of such products by the Department of Health and Human Services.
References
- Bansal S, NCT04478773: Evaluating MRI Scanning in Patients With Fractured or Abandoned Endocardial Leads. US Clinical Trial; 2020-2022.
- Acikel V, Magrath P, Parker SE, Hu P, Wu HH, Finn JP, et al. RF-induced heating of pacemaker/ICD lead-tips during MRI Scans at 1.5T and 3T: Evaluation in Cadavers. Journal of Cardiovascular Magnetic Resonance 2016;18:O121.
- Higgins JV, Gard JJ, Sheldon SH, Espinosa RE, Wood CP, Felmlee JP, et al. Safety and Outcomes of Magnetic Resonance Imaging in Patients with Abandoned Pacemaker and Defibrillator Leads. Pacing and Clinical Electrophysiology 2014;37(10):1284–1290. https://onlinelibrary.wiley.com/doi/abs/10.1111/pace.12419.
- Kim J, Hwang J, Choi JH, Choi HI, Kim MS, Jung SH, et al. Frequency and clinical impact of retained implantable cardioverter defibrillator lead materials in heart transplant recipients. PLOS ONE 2017 05;12(5):1–9. https://doi.org/10. 1371/journal.pone.0176925.
- Morris MF, Verma DR, Sheikh H, Su W, Pershad A. Outcomes after magnetic resonance imaging in patients with pacemakers and defibrillators and abandoned leads. Cardiovascular Revascularization Medicine 2018;19(6):685 – 688. http://www.sciencedirect.com/science/article/pii/S1553838918300095.
- Padmanabhan D, Kella DK, Mehta R, Kapa S, Deshmukh A, Mulpuru S, et al. Safety of magnetic resonance imaging in patients with legacy pacemakers and defibrillators and abandoned leads. Heart Rhythm Society 2017;15:228–233.
- Russo RJ, Costa HS, Silva PD, Anderson JL, Arshad A, Biederman RWW, et al. Assessing the Risks Associated with MRI in Patients with a Pacemaker or Defibrillator. New England Journal of Medicine 2017;376(8):755–764. https: //doi.org/10.1056/NEJMoa1603265, pMID: 28225684.
- Jensen TS, Chin J, Ashby L, Rollins J, Caños DA, Hutter J, et al., Decision memo for magnetic resonance imaging (MRI) (CAG-00399R4). US Centers for Medicare and Medicaid Services; 2018.
- Verma A, Ha ACT, Dennie C, Essebag V, Exner DV, Khan N, et al., Canadian Heart Rhythm Society and Canadian Association of Radiologists Consensus Statement on Magnetic Resonance Imaging with Cardiac Implantable Electronic Devices. Canadian Association of Radiologists Journal 2014;65(4):290–300. https://doi.org/10.1016/j.carj.2014.08.001, pMID: 25440499.
- Liorni I, Neufeld E, Kühn S, Murbach M, Zastrow E, Kainz W, et al. Novel Mechanistic Model and Computational Ap- proximation for Electromagnetic Safety Evaluations of Electrically Short Implants. Physics in Medicine and Biology 2018 11;63(22):225015. https://doi.org/10.1088/1361-6560/aae94c.
- Park SM, Kamondetdacha R, Nyenhuis JA. Calculation of MRI-induced heating of an implanted medical lead wire with an electric field transfer function. J Magn Reson Imaging 2007;26(5):1278–1285.
- Langman DA, Finn JP, Ennis DB. Abandoned Pacemaker Leads Are a Potential Risk for Patients Undergoing MRI. Pacing and Clinical Electrophysiology 2011;34(9):1051–1053. https://onlinelibrary.wiley.com/doi/abs/10.1111/j.1540- 8159.2011.03176.x.
- Mattei E, Gentili G, Censi F, Triventi M, Calcagnini G. Impact of capped and uncapped abandoned leads on the heating of an MR-conditional pacemaker implant. Magnetic Resonance in Medicine 2015;73(1):390–400. https://onlinelibrary.wiley.com/doi/abs/10.1002/mrm.25106.
- Balmer C, Gass M, Dave H, Duru F, Luechinger R. Magnetic Resonance Imaging of Patients with Epicardial Leads: In-vitro Evaluation of Temperature Changes at the Lead Tip. Journal of Interventional Cardiac Electrophysiology 2019;56:321–326
Figures