0320
Intraindividual comparison of stack-of-stars acquisition for arterial phase imaging with and without breath-holding on dynamic MRI of the liver
Shintaro Ichikawa1, Utaroh Motosugi2, Tetsuya Wakayama3, Satoshi Funayama1, Daiki Tamada1, Sagar Mandava4, Ty A Cashen5, and Hiroshi Onishi1
1Department of Radiology, University of Yamanashi, Chuo, Japan, 2Kofu Kyoritsu Hospital, Kofu, Japan, 3GE Healthcare, Hino, Japan, 4GE Healthcare, Atlanta, GA, United States, 5GE Healthcare, Madison, WI, United States
1Department of Radiology, University of Yamanashi, Chuo, Japan, 2Kofu Kyoritsu Hospital, Kofu, Japan, 3GE Healthcare, Hino, Japan, 4GE Healthcare, Atlanta, GA, United States, 5GE Healthcare, Madison, WI, United States
Synopsis
We performed intra-individual comparison of arterial phase (AP) images between differential subsampling with Cartesian ordering (DISCO) and stack-of-stars acquisition without breath-holding (DISCO-Star) on dynamic magnetic resonance imaging of the liver. Patients showing inadequate scan timing of AP in DISCO and DISCO-Star (12 s/phase) dataset were 4.9% and 21.2%, respectively. One advantage of DISCO-Star was that the adequate scan timing of AP can be obtained by using additional high frame rate reconstruction (3 s/phase) in the patient with inadequate scan timing in routine reconstruction. DISCO-Star was useful to obtain adequate AP imaging in all patients.
Introduction
Dynamic contrast-enhanced magnetic resonance imaging (DCE-MRI) of the liver is typically performed using a breath-holding 3D gradient echo sequence. However, breath-holding for >10 s is sometimes difficult for some patients. In such patients, image quality may be impaired with respiratory motion artifacts during breath-hold acquisition, leading to diagnostic inaccuracy. Multiple arterial phase acquisition can be a solution for respiratory artifacts. Differential subsampling with Cartesian ordering (DISCO) is a high spatiotemporal-resolution dynamic contrast-enhanced MRI technique that combines a dual-echo SPGR sequence with pseudo-random variable-density k-space segmentation and view-sharing reconstruction1. It could provide at least one image set with reduced or no artifacts. Another strategy for reducing the respiratory artifact is breath-hold-free acquisition. Respiratory gating with navigator echoes is available to obtain 3D gradient echo sequences without breath-holding. However, respiratory gating prolongs the acquisition time, leading to limited time resolution. DISCO-Star is a stack-of-stars technique that is robust for respiratory motion compared with Cartesian sampling2 and is useful for obtaining free-breathing DCE-MRI. To date, there has been no direct comparison of the image quality of arterial phase (AP) imaging between DISCO and DISCO-Star. Thus, this study aimed to investigate the utility of AP imaging using DISCO-Star compared to DISCO.Methods
This retrospective study was approved by the institutional review board, and the requirement for informed patient consent was waived. Forty-one patients who underwent gadoxetate disodium-enhanced MRI using DISCO and DISCO-Star at different time points with a 3-T MRI system were enrolled. Gadoxetate disodium (0.025 mmol/kg body weight) was administered at a rate of 1 mL/s, followed by a 20-mL saline flush using a power injector. Imaging parameters of DISCO and DISCO-Star are shown in Fig.1. In the DISCO-Star sequence, a total of 1500 radial spokes were acquired in 4 min continuously, and for routine frame rate reconstruction, 20 phases with 150 spokes per phase were reconstructed using 75 spokes offset between phases, which was equivalent to 12 s/phase. In each phase reconstruction, an auto-calibrating reconstruction for the Cartesian sampling (ARC) algorithm was used before Fourier transformation in the kz direction and conjugate gradient-sensitivity encoding (CG-SENSE) algorithm was used for in-plane reconstruction3. Soft-gating, a retrospective gating technique, was used to suppress image blur due to respiratory motion4. Visual assessment of the scan timing of AP (adequate or inadequate) was performed for each group, and in case of inadequate scan timing in the DISCO-Star group, retrospective reconstruction with a high frame rate (80 phases, 3 s/phase) was added. Adequate scan timing of AP was defined as that time when the antegrade flow enhanced the hepatic artery and portal vein but not the hepatic vein (Fig. 2). Artifact (5-point visual score: 5, no; 4, mild; 3, moderate; 2, extreme; 1, unreadable), overall image quality (5-point visual score: 5, excellent; 4, good; 3, acceptable; 2, poor; 1, non-acceptable), and the diagnosable image quality (≥3) were also assessed for each group and compared using the chi-square test. The non-inferiority of the AP image quality of DISCO-Star was compared to that of DISCO using the two one-sided McNemar tests with 5% non-inferiority margins.Results
Inadequate scan timing of AP was observed in two patients (4.9%, 2/41) in the DISCO dataset and nine patients (22.0%, 9/41) in the DISCO-Star dataset, respectively. Adequate scan timing of AP was observed in the 3rd phase (21.2%, 7/32), 4th phase (66.7%, 22/32), or 5th phase (9.5%, 3/32) in the DISCO-Star dataset. (Fig. 3). In all patients with inadequate timing of AP in DISCO-Star dataset, retrospective additional reconstruction with a high frame rate offered images of adequate scan timing of AP (Fig. 4). DISCO-Star showed lower scores for streak artifacts and overall image quality (P < 0.0001). However, non-inferiority in the proportion of diagnosable images in the DISCO-Star dataset in comparison with the DISCO dataset (P = 0.036). (Fig. 5).Discussion
Our results revealed that DISCO-Star showed a high performance in obtaining AP images with adequate scan timing. Although routine frame rate reconstruction (12 s/phase) was not perfect, retrospective high frame rate reconstruction (3 s/phase) salvaged the AP images in cases with inadequate scan timing of AP by routine frame rate. AP is the most important phase in DCE-MRI of the liver. There are some drawbacks to obtaining optimal AP images on gadoxetate disodium-enhanced MRI. Previous reports revealed that a high incidence (7%–14%) of patients self-reported transient dyspnea after the administration of gadoxetate disodium5,6. Its injection volume is half that of extracellular contrast agents, which causes a short duration of adequate scan timing and truncation artifacts due to k-space inhomogeneity7,8. DISCO-Star without breath-holding is a good solution to obtain optimal AP images because there is no worry of missing scan timing of AP and it is not affected by respiratory motion artifacts. Our results revealed that there was no significant difference in diagnosable image quality between the DISCO-Star and DISCO datasets. However, the degradation of image quality due to streak artifacts is a problem to be solved.Conclusion
The use of DISCO-Star is the good solution to obtain the optimal AP images.Acknowledgements
No acknowledgement found.References
1. Saranathan M, Rettmann DW, Hargreaves BA, et al. DIfferential Subsampling with Cartesian Ordering (DISCO): a high spatio-temporal resolution Dixon imaging sequence for multiphasic contrast enhanced abdominal imaging. J Magn Reson Imaging. 2012;35:1484–1492. 2. Peters DC, Korosec FR, Grist TM, et al. Undersampled projection reconstruction applied to MR angiography Magn Reson Med. 2000;43:91-101. 3. Pruessmann KP, Weiger M, Bornert P, et al. Advances in sensitivity encoding with arbitrary k-space trajectories Magn Reson Med. 2001;46:638-651. 4. Johnson KM, Block WF, Reeder SB et al. Improved least squares MR image reconstruction using estimates of k-Space data consistency. Magn Reson Med. 2012;67:1600-1608. 5. Motosugi U, Bannas P, Bookwalter CA, et al. An investigation of transient severe motion related to gadoxetic acid-enhanced MR imaging. Radiology. 2016;279(1):93-102. 6. McClellan TR, Motosugi U, Middleton MS, et al. Intravenous gadoxetate disodium administration reduces breath-holding capacity in the hepatic arterial phase: A multi-center randomized placebo-controlled trial. Radiology. 2017;282(2):361-368. 7. Haradome H, Grazioli L, Tsunoo M, et al. Can MR fluoroscopic triggering technique and slow rate injection provide appropriate arterial phase images with reducing artifacts on gadoxetic acid-DTPA (Gd-EOB-DTPA)-enhanced hepatic MR imaging? J Magn Reson Imaging. 2010;32(2):334-340. 8. Motosugi U, Ichikawa T, Sou H, et al. Dilution method of gadolinium ethoxybenzyl diethylenetriaminepentaacetic acid (Gd-EOB-DTPA)-enhanced magnetic resonance imaging (MRI). J Magn Reson Imaging. 2009;30(4):849-854.Figures
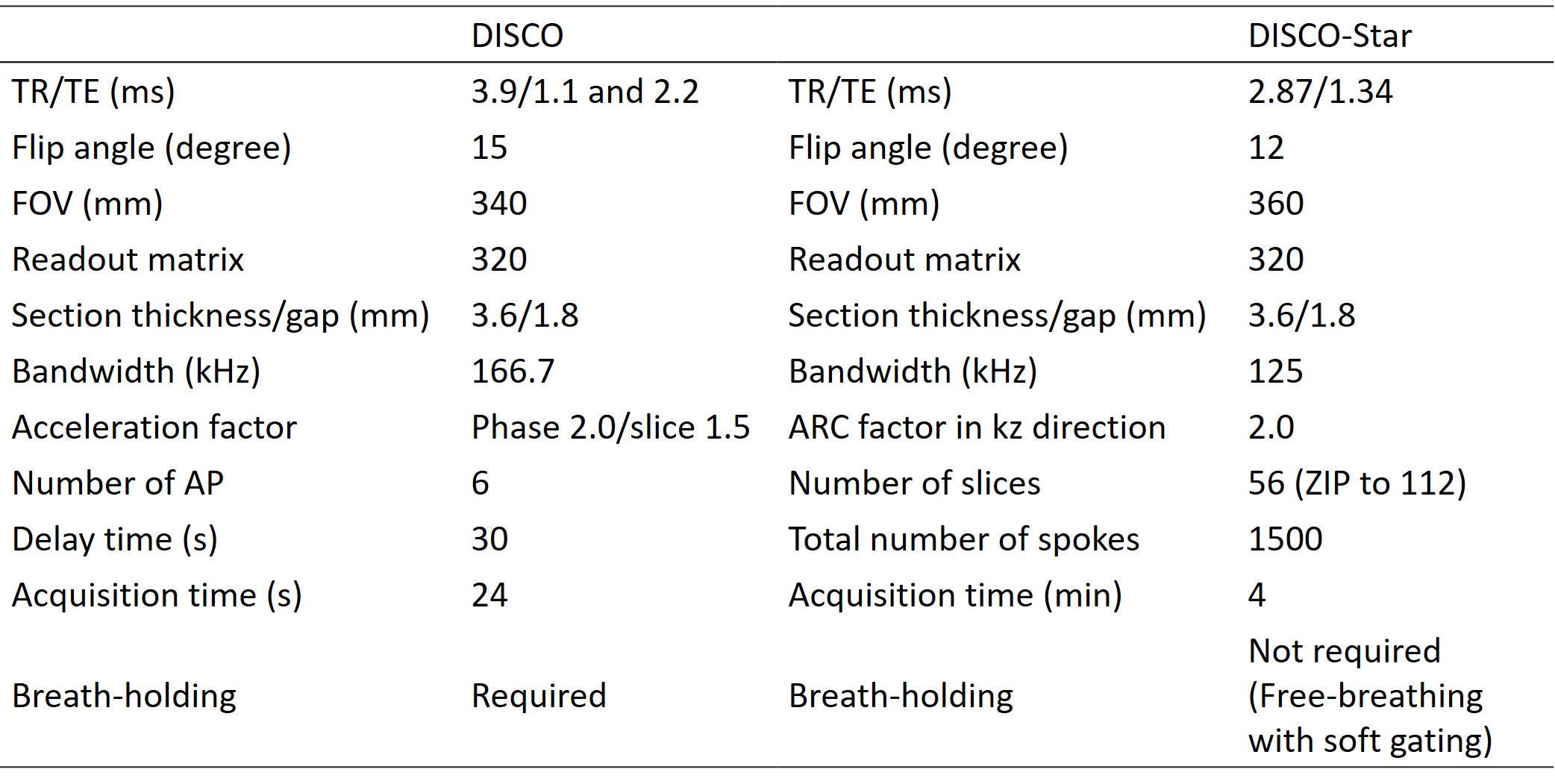
Fig. 1. Imaging parameters of DISCO and DISCO-Star.
DISCO was started
30 s after the start of contrast administration. Six phases arterial
phase (AP) images, within a single
breath-hold with oxygen inhalation were obtained (temporal resolution, ~4 s).
In DISCO-Star
sequence, total of 1500 radial spokes were acquired in 4 min continuously and
20 phases were reconstructed (12 s/phase) for routine frame rate
reconstruction. The retrospective
gating technique was used to suppress the image blur.
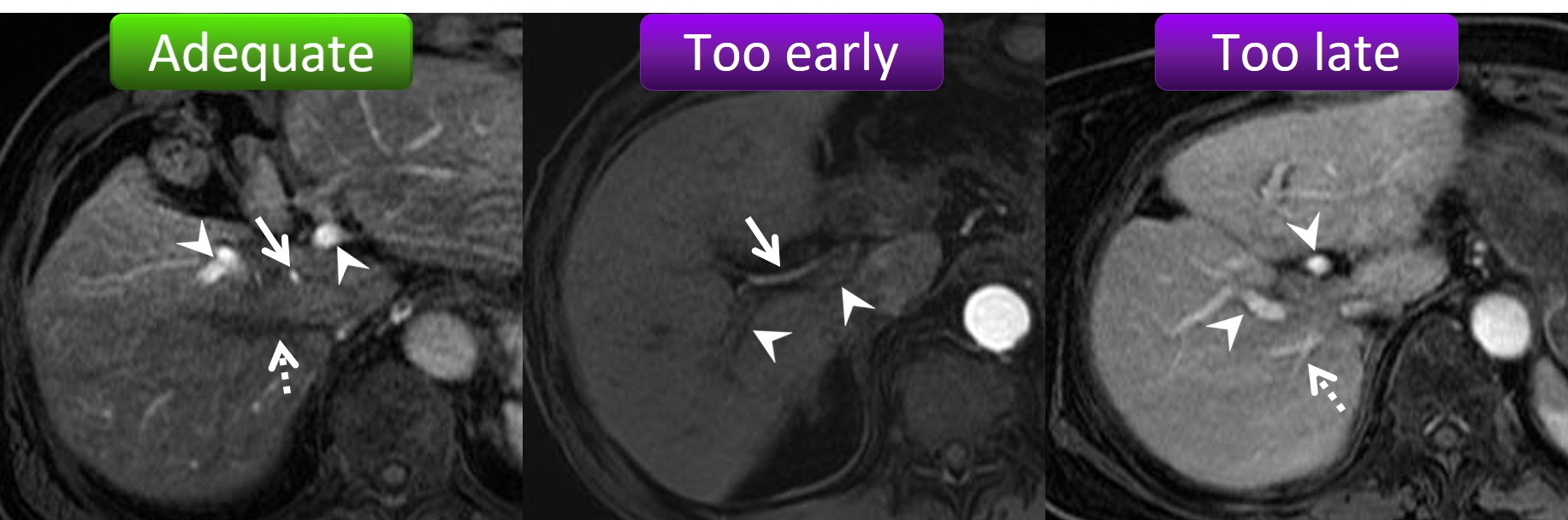
Fig. 2. Scan timing of the arterial phase
(AP).
The adequate scan timing of the AP is when
the hepatic artery (arrow) and portal vein (arrowhead) are enhanced but the
hepatic vein is not yet enhanced (dotted arrow) (left image). If only the
hepatic artery is enhanced (arrow), the scan timing is too early (middle image).
If the hepatic vein is already enhanced (dotted arrow), the scan timing is too
late (right image). Inadequate AP was defined as too early and too late scan
timings.
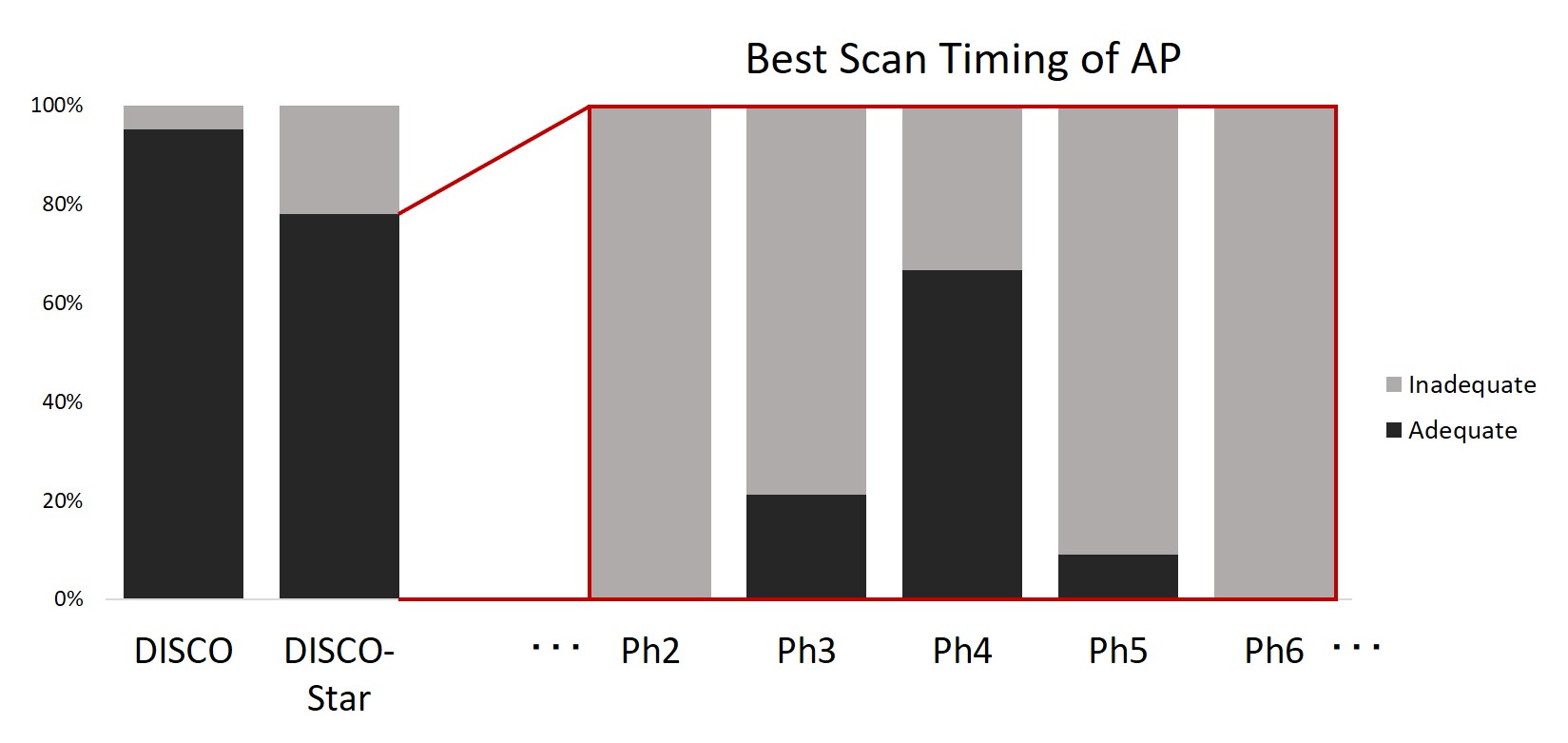
Fig. 3. The ratio of adequate scan timing
of arterial phase (AP) on each sequence and phase.
Inadequate scan timing of AP was observed two
patients (4.9%, 2/41) in DISCO dataset
and nine patients (22.0%, 9/41) in DISCO-Star dataset, respectively. The
adequate scan timing of AP was observed
in the 3rd phase (21.2%, 7/32), 4th phase (66.7%, 22/32), or 5th phase (9.5%,
3/32) in DISCO-Star dataset.
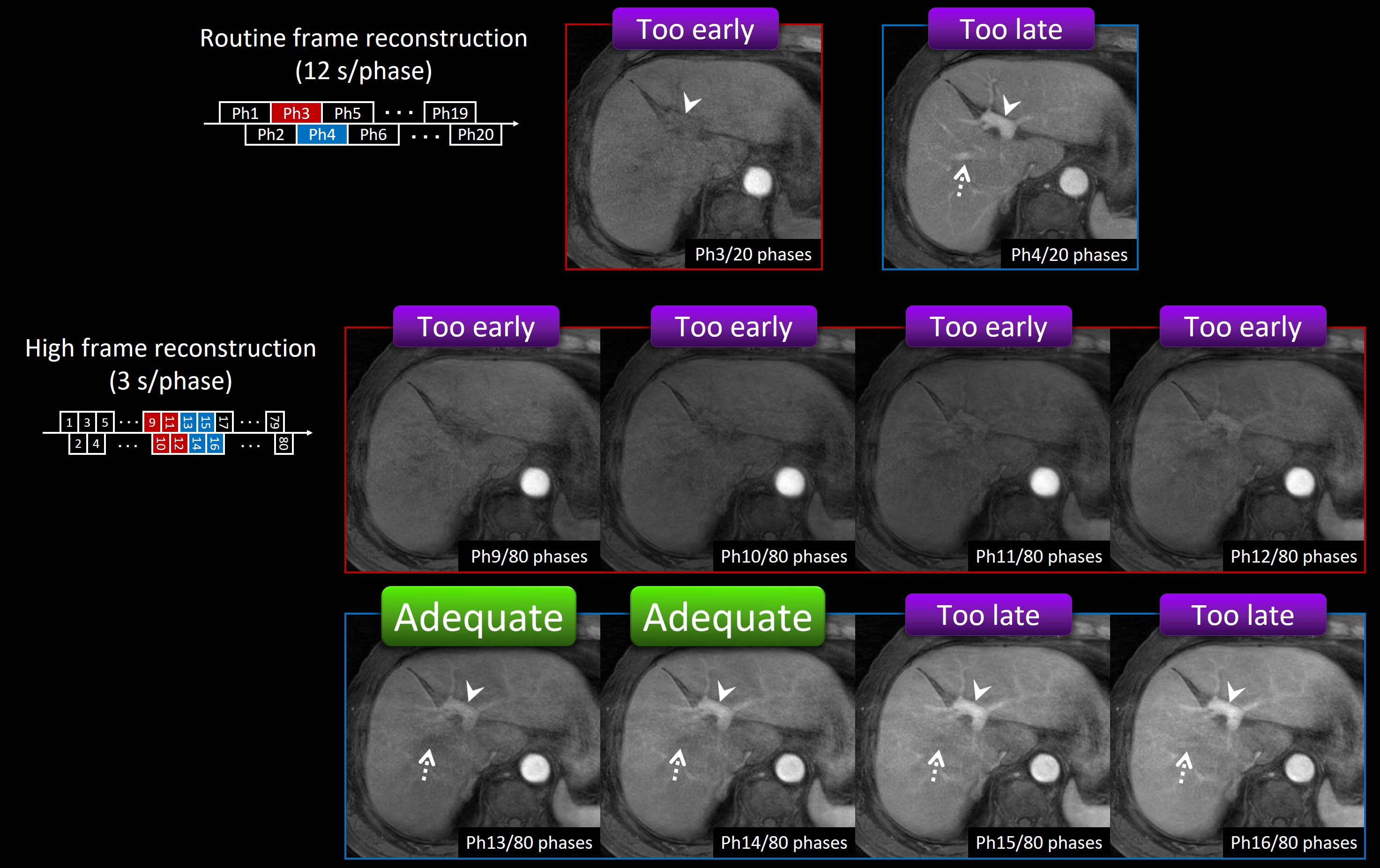
Fig. 4. Example of the utility of high frame rate reconstruction.
Adequate scan timing of arterial phase (AP)
was not observed on routine frame
reconstruction (12 s/phase). Portal vein (arrowhead) was not enough
enhanced in the 3rd phase and hepatic vein (dotted arrow) was already enhanced
in the 4th phase. Optimal AP was obtained with high frame rate reconstruction (3 s/phase). Portal vein
(arrowhead) was enhanced but the hepatic vein (dotted arrow) was not yet
enhanced in the 13th and 14th phase.
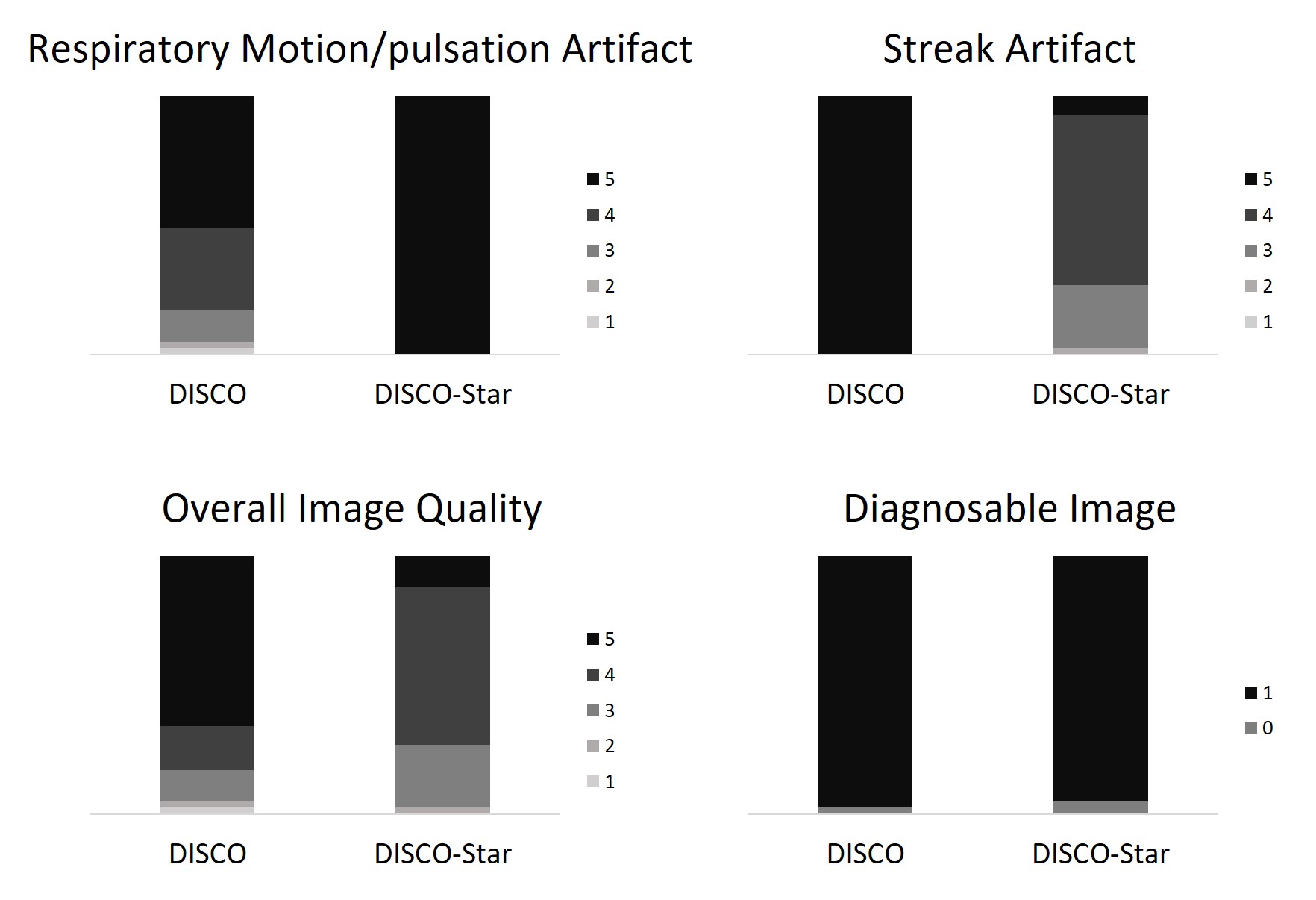
Fig. 5. Stacked bar graph representing
results of the visual assessment.
No respiratory motion/pulsation artifact was
observed in DISCO-Star dataset (P
< 0.0001). DISCO-Star showed lower score of streak artifact and overall
image quality (P < 0.0001).
However, there was non-inferiority in the proportion of diagnosable image in DISCO-Star
dataset in comparison with DISCO dataset.