0316
Motion-Resolved Four-Dimensional Abdominal Diffusion-Weighted Imaging using Propeller Echo-Planar Imaging (4D-DW-Propeller-EPI)1Department of Diagnostic Radiology, The University of Hong Kong, HongKong, China, 2Department of Health Technology and Informatics, The Hong Kong Polytechnic University, HongKong, China
Synopsis
Motion-resolved four dimensional diffusion-weighted echo-planar imaging (4D-DW-EPI) may better characterize the respiratory-induced motion of tumor than 4D-MRI with conventional T1 and T2 image contrasts. However, the existing 4D-DW-EPI technique can only provide limited geometric accuracy and low sampling rate over respiratory cycles. Thus, we proposed an advanced 4D-DW-Propeller-EPI technique with golden angle acquisition for improving the geometric accuracy and data sampling rate. Simulation study and in-vivo study were conducted to evaluate the performance of 4D-DW-Propeller-EPI. Our results demonstrate that 4D-DW-Propeller-EPI showed superior image quality to 4D-DW-EPI and had a potential for the application of MRI-guided abdominal radiotherapy.
Introduction
In past two decades, various motion-resolved four dimensional MRI (4D-MRI) techniques with conventional image contrasts (i.e., T1 and T2 weightings) have been proposed to characterize the respiratory-induced motion of the tumor for MRI-guided abdominal radiotherapy (RT)1. Although diffusion-weighted imaging (DWI) may better delineate the tumor and provide the assessment of treatment response2, implementing abdominal 4D-DWI is technically challenging. Yilin Liu et al. first demonstrated the feasibility of 4D single-shot diffusion-weighted echo-planar imaging (4D-DW-EPI) with 1) repeated data acquisition over multiple respiratory cycles and 2) retrospective data sorting method3. This pioneer study also preliminarily showed improvements in delineation of target volume for the planning of MRI-guided RT. However, 4D-DW-EPI can only provide limited geometric accuracy4 and low data sampling rate over multiple respiratory cycles (4~5s for whole liver coverage). Parallel imaging can alterative above issues, but it only shows limited improvement in the abdomen5. Previously, 2D-DW-Propeller-EPI has been shown able to achieve high-quality free-breathing liver DWI with excellent geometric accuracy6–8. In this study, we aim to develop an advanced 4D-DWI by using 2D-DW-Propeller-EPI with golden angle acquisition (4D-DW-Propeller-EPI)9,10 for improving the geometric accuracy and data sampling rate.Materials and methods
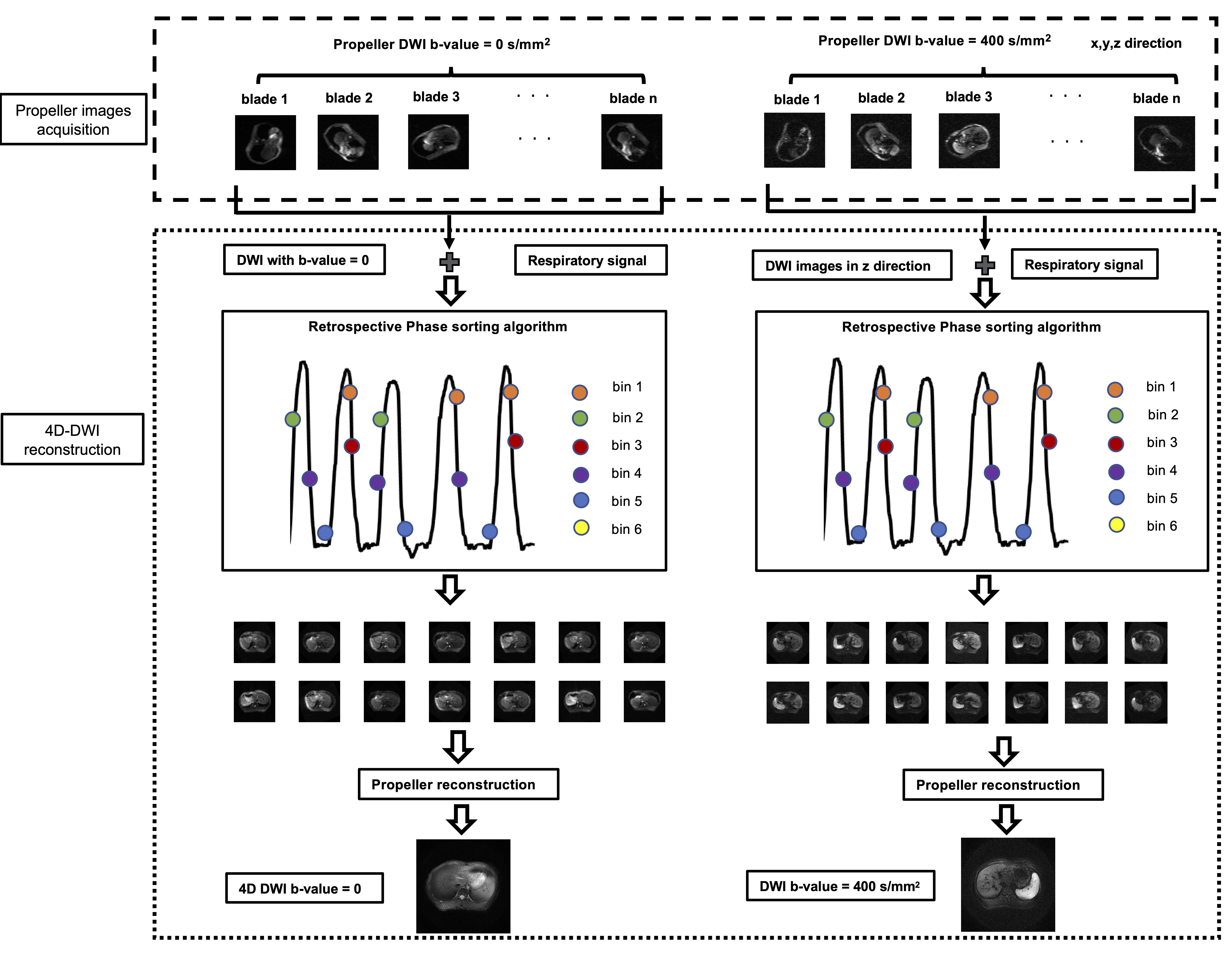
4D-DW-Propeller-EPIFig.1 shows the framework of proposed 4D-DW-Propeller-EPI technique, with golden angle (111.25o) for improving the k-space coverage in repeated data sampling. Compared to 4D-DW-EPI, the shortened ETL in each blade acquisition (e.g., ETL=32) can reduce the TR per volume coverage, thereby improving the data sampling rate.
Simulation Study
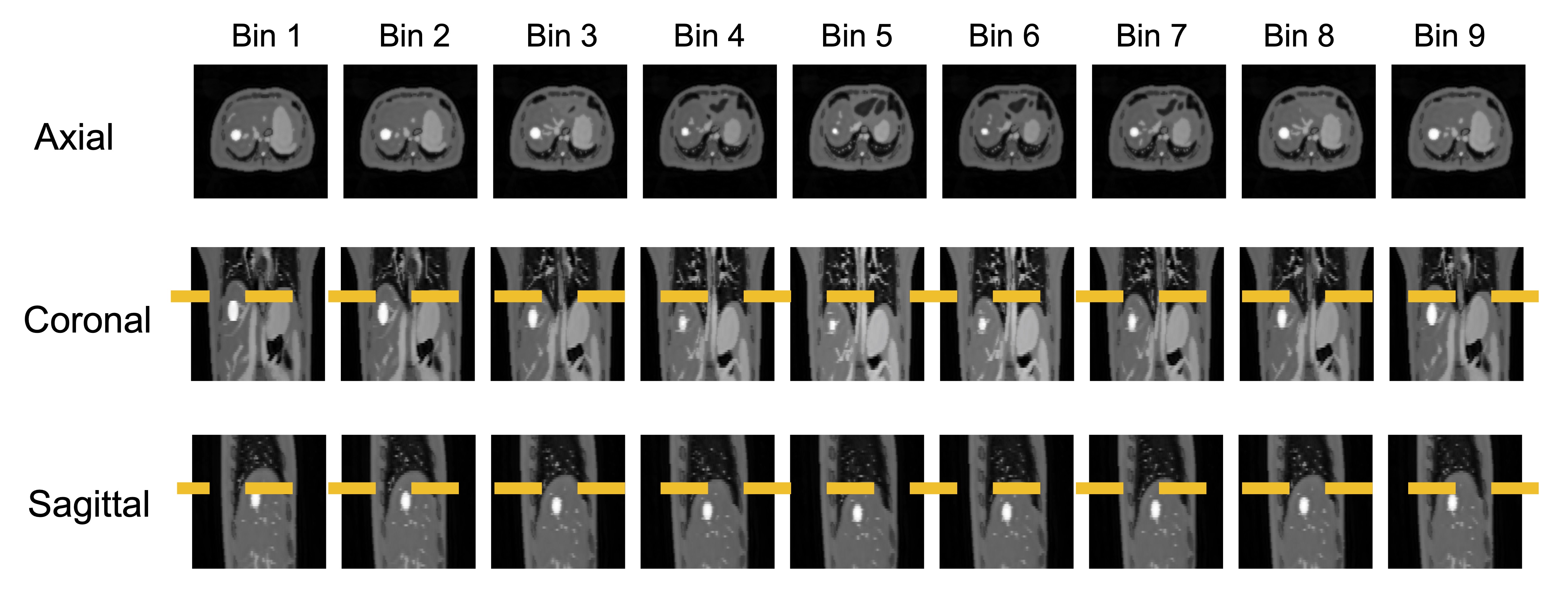
4D Digital Extended Cardiac-Torso (XCAT) phantom was used to evaluate the improvement of k-space coverage with 4D-DW-Propeller-EPI. Dynamic abdominal images (256x256; 1.6mm slice thickness) were generated with the respiratory period of 4s, and diaphragm motion of +/-20 mm. The 4D-DW-Propeller-EPI acquisition was simulated by sampling each blade data (128x32) with golden angle at corresponding respiratory phase with a 1.25s TR. The simulated data then underwent phase binning3 and Propeller-EPI reconstruction for producing 4D-DWI data.
In-vivo Study
Image acquisition: 4D-DW-Propeller-EPI data were acquired from a healthy volunteer under free-breathing at a 1.5T MRI (Explore, GE Healthcare) using a 12-channel body coil. 2D abdominal images with 8mm slice thickness were acquired in an interleaved slice order with two diffusion contrasts (b=0 and b=400 along z direction), and total 180 blades (matrix size=128x32) with rotating angle at 111.25o (golden angle) were acquired for each diffusion contrast. Two different data sampling rates were tested with (1) TR of 1250ms (maximum slice coverage=8; total scantime=450s), and (2) TR = 2000 ms (maximum slice coverage=14; total scantime=720s). In addition, 4D-DW-Propeller-EPI data with 15o rotating angle (TR=4000ms, slice coverage=20, slice thickness=8mm, number of blades=90), and 4D-DW-EPI data (TR=4000ms, slice coverage=26, slice thickness=8mm) were also acquired from another healthy volunteer for comparison.
Respiratory signal recording: A bellow was used to monitor the respiration, and the recorded waveform (sampling rate=25Hz) served as an external respiratory surrogate signal.
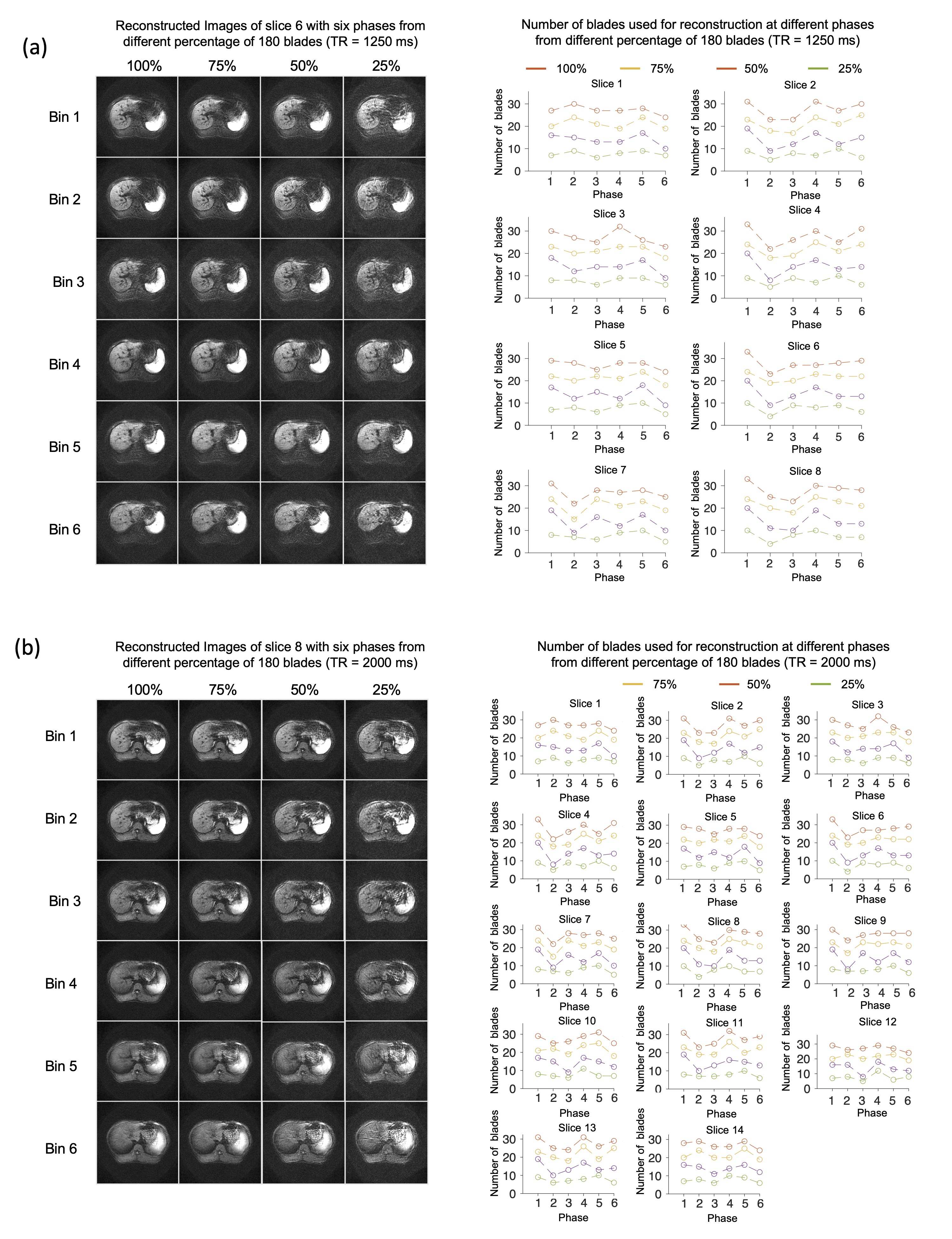
Data reconstruction: For 4D-DW-EPI, phase binning was performed to generate the dataset with six respiratory phases according to the recorded respiratory surrogate signal3. For 4D-DW-Propeller-EPI, at each scan locations, the phase binning was firstly performed on all blade data to separate the blade data into six-phase bins, and then the blade data falling into same phase bin were combined by using Propeller-EPI reconstruction6-8. In addition, to evaluate the effect of reducing sampling duration, we used 100%, 75%, 50%, and 25% of blade data (total 180 blades) to reconstruct the 4D-DWI data with the same target number of respiratory phases.
Results
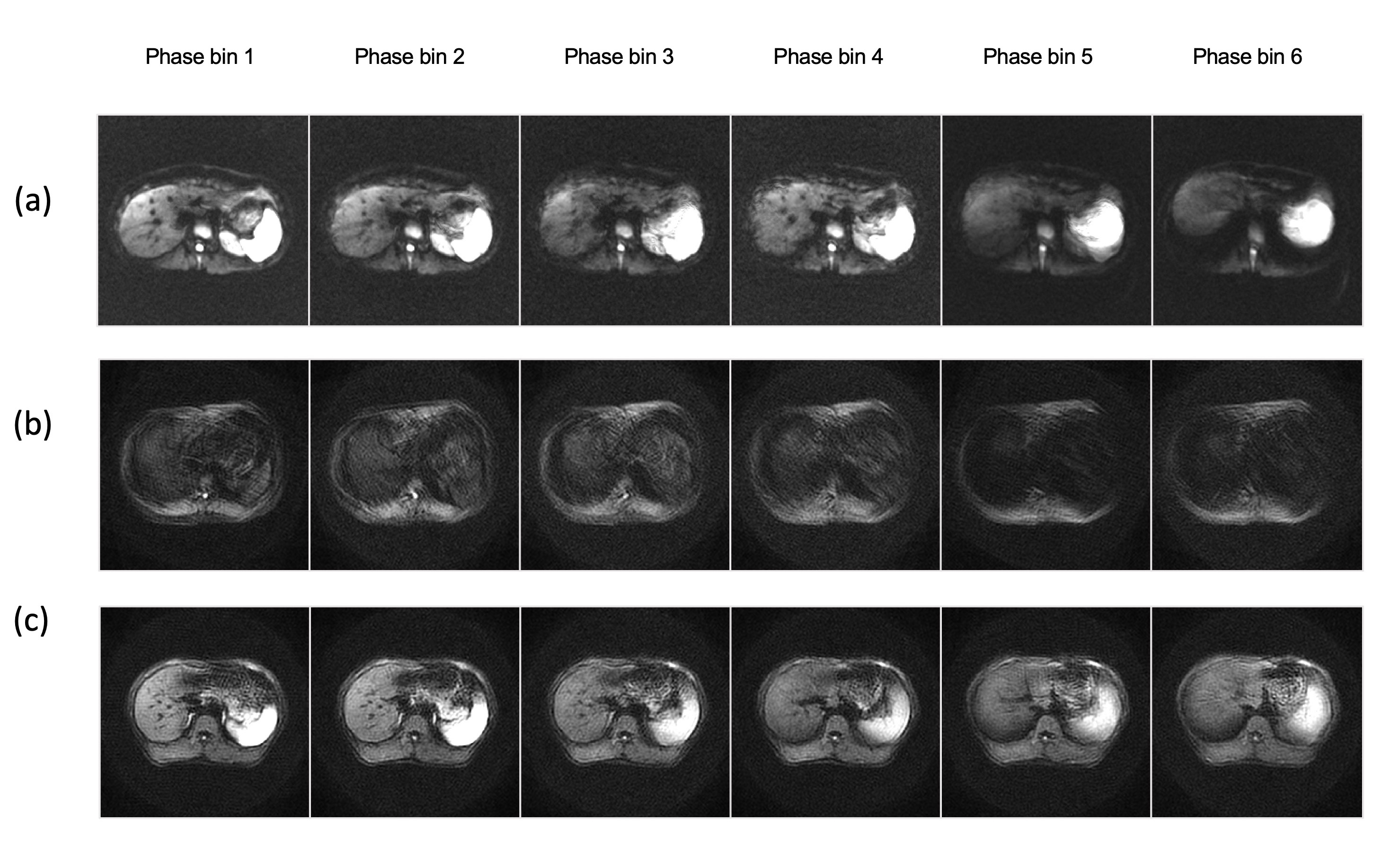
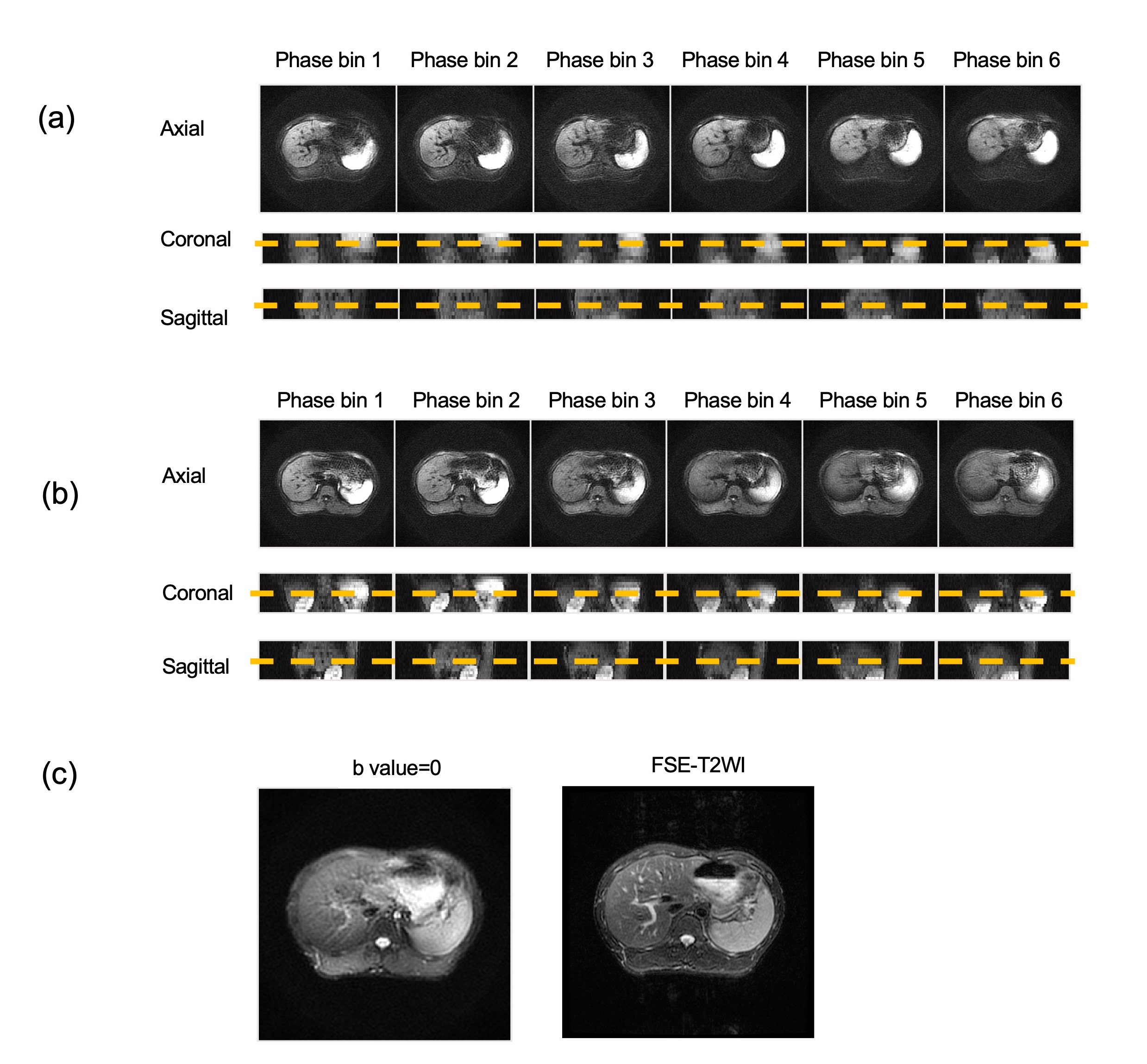
Fig.2 shows the simulated result of 4D-DW-Propeller-EPI abdominal images with nine respiratory phases. Fig.3 compares the in-vivo 4D-DWI images with six respiratory phases reconstructed from the data acquired with 4D-DW-EPI, 4D-DW-Propeller-EPI without golden angle (15°), and 4D-DW-Propeller-EPI with golden angle (111.25°). Fig.4 shows in-vivo 4D-DW-Propeller-EPI images reconstructed from 100%, 75%, 50%, and 25% of blade data acquired with two different TRs. Fig.5 shows the reformatted 4D-DW-Propeller-EPI images reconstructed from 100% of blade data, and the comparison with routine FSE-T2 images.Discussion
Compare with 4D-DW-EPI, the proposed 4D-DW-Propeller-EPI can improve the geometric accuracy (Fig.5c) and data sampling rate, thereby enabling high-quality 4D-DWI. The use of golden angle can provide better coverage in the k-space(Fig.3), because it can reduce the redundancy of blade data after phase binning. However, like most 4D-MRI techniques, 4D-DW-Propeller-EPI relies on oversampling of data with multiple respiratory cycles, leading to prolonged scantime. Shortening the sampling duration can significantly reduce the number of blades available in each phase bin for subsequent Propeller-EPI reconstruction, resulting in degraded image quality (Fig.4). In this preliminary evaluation, the quality of reconstructed data remains comparable when using 75% of acquired blade data (i.e., 25% reduction of scantime). Less usage of acquired blade data (e.g., >50% reduction of scantime) can cause insufficient blade data for the image reconstruction of each respiratory phase. Moreover, even though higher data sampling rate is preferable (i.e., TR=1.25s in Fig.4), the slice coverage of proposed 4D-DW-Propeller-EPI is insufficient. To further improve acquisition efficiency of proposed 4D-DW-Propeller-EPI, an advanced Propeller-EPI reconstruction method with both in-plane and through-plane accelerations (e.g., multi-band imaging) is needed11. In conclusion, the superior image quality and improved geometric accuracy of 4D-DW-Propeller-EPI may benefit the application of MRI-guided abdominal RT.Acknowledgements
Updated acknowledgement: The work was in part supported by grants from Hong Kong Research Grant Council (GRFs HKU17138616, HKU17121517, HKU17106820, and GRF 151021/18M), Hong Kong Innovation and Technology Commission (ITS/403/18), and Health and Medical Research Fund (HMRF 06173276).References
(1) Stemkens, B.; Paulson, E. S.; Tijssen, R. H. Nuts and Bolts of 4D-MRI for Radiotherapy. Physics in Medicine & Biology 2018, 63 (21), 21TR01.
(2) Giles, S. L.; Messiou, C.; Collins, D. J.; Morgan, V. A.; Simpkin, C. J.; West, S.; Davies, F. E.; Morgan, G. J.; deSouza, N. M. Whole-Body Diffusion-Weighted MR Imaging for Assessment of Treatment Response in Myeloma. Radiology 2014, 271 (3), 785–794.
(3) Liu, Y.; Zhong, X.; Czito, B. G.; Palta, M.; Bashir, M. R.; Dale, B. M.; Yin, F.-F.; Cai, J. Four-Dimensional Diffusion-Weighted MR Imaging (4D-DWI): A Feasibility Study. Medical physics 2017, 44 (2), 397–406.
(4) Taouli, B.; Koh, D.-M. Diffusion-Weighted MR Imaging of the Liver. Radiology 2010, 254 (1), 47–66.
(5) Lewis, S.; Dyvorne, H.; Cui, Y.; Taouli, B. Diffusion-Weighted Imaging of the Liver: Techniques and Applications. Magnetic Resonance Imaging Clinics 2014, 22 (3), 373–395.
(6) Chang, H.-C.; Chen, N.-K.; Juan, C.-J.; Chuang, T.-C.; Ko, C.-W.; Chung, H.-W. Free Breathing Liver DWI Using PROPELLER-DW-EPI with Inherent Reductions of Geometric Distortion and Motion Artifacts at 1.5 T.
(7) Chuang, T.-C.; Huang, T.-Y.; Lin, F.-H.; Wang, F.-N.; Juan, C.-J.; Chung, H.-W.; Chen, C.-Y.; Kwong, K. K. PROPELLER-EPI with Parallel Imaging Using a Circularly Symmetric Phased-Array RF Coil at 3.0 T: Application to High-Resolution Diffusion Tensor Imaging. Magnetic Resonance in Medicine: An Official Journal of the International Society for Magnetic Resonance in Medicine 2006, 56 (6), 1352–1358.
(8) Wang, F.-N.; Huang, T.-Y.; Lin, F.-H.; Chuang, T.-C.; Chen, N.-K.; Chung, H.-W.; Chen, C.-Y.; Kwong, K. K. PROPELLER EPI: An MRI Technique Suitable for Diffusion Tensor Imaging at High Field Strength with Reduced Geometric Distortions. Magnetic Resonance in Medicine: An Official Journal of the International Society for Magnetic Resonance in Medicine 2005, 54 (5), 1232–1240.
(9) Nehrke, K.; Börnert, P.; van Yperen, G. H.; Eggers, H. Golden Angle PROPELLER MRI.
(10) Wen, Q.; Feng, L.; Zhou, K.; Wu, Y.-C. Rapid Golden-Angle Diffusion-Weighted Propeller MRI for Simultaneous Assessment of ADC and IVIM. NeuroImage 2020, 223, 117327.
(11) Liu X, Cui D, Dai E, Hui ES, Chan Q, and Chang HC, “Self-calibrated and Collaborative Propeller-EPI Reconstruction (SCOPER) for High-Quality Diffusion-Tensor Imaging”, International Society for Magnetic Resonance in Medicine, 27th Annual Meeting, Montreal, Canada, May 2019.
Figures