0310
Abnormal aortic hemodynamics at predilection sites for dissection in Marfan patients: a 4D flow study
Pim van Ooij1, Mitzi van Andel2, Lukas M. Gottwald1, Aart J Nederveen1, and Maarten Groenink1
1Radiology & Nuclear Medicine, Amsterdam University Medical Centers, location AMC, Amsterdam, Netherlands, 2Cardiology, Amsterdam University Medical Centers, location AMC, Amsterdam, Netherlands
1Radiology & Nuclear Medicine, Amsterdam University Medical Centers, location AMC, Amsterdam, Netherlands, 2Cardiology, Amsterdam University Medical Centers, location AMC, Amsterdam, Netherlands
Synopsis
In this study we use 4D flow MRI techniques to investigate abnormal magnitude and direction of blood flow velocity and wall shear stress in patients with Marfan syndrome, a congenital disease that may cause aortic dissection. We found that patients that underwent aortic root repair have significantly more abnormal hemodynamics and that abnormally elevated hemodynamics were associated with blood pressure chracteristics. Abnormally directed hemodynamics were not associated with any patient characteristics, but showed a distinct regional increase at the inner proximal descending aorta, awell-know predilection site for aortic dissection in Marfan patients.
Introduction
Marfan syndrome is an inherited connective tissue disease mainly affecting the aorta.This condition may lead to aortic aneurysm formation, aortic dissection and subsequent sudden death at a relatively young age when untreated surgically. Altered aortic geometry end elastic function are probably both the result and the cause of the degenerative changes in the aortic wall. Interactions between aortic geometry and mechanic aortic wall properties probably result in altered aortic flow patterns as shown in previous 4D flow MRI studies (1,2). Hemodynamic evaluation of the aorta may indicate locations that are prone for aortic dissection and guide medicinal therapy to relieve stresses on the aortic wall in individual Marfan patients, in an attempt to postpone prophylactic aortic surgery. Here we present an aortic 4D flow MRI analysis, providing a comprehensive quantification and visualization of abnormal aortic velocity and WSS magnitude and direction with recently developed techniques 1,2. We hypothesize that abnormal hemodynamics are found in regions associated with dissection and are associated with patient characteristics (e.g. age, gender and aortic diameter).Methods
Fifty-six Marfan patients were prospectively included to participate in the study and provided informed consent. Twenty-five healthy subjects (age: 37 ± 13 (24 – 65), gender: 15 M, 10 W) were prospectively included as part of an earlier study3. Aortic 4D flow MRI was performed on a 3T Philips Ingenia system (Best, Netherlands). Subject demographics, abbreviations and scan specifics are given in table 1, of which the aortic diameters were measured on a Dixon scan (figure 1 shows an example for the sinus of Valsalva). The aorta was manually segmented on time-averaged phase contrast MR angiogram images (phase contrast images multiplied absolute velocity) by threshold, watershed and manual voxel in-/exclusion in Mimics (Materialise, Leuven, Belgium). The segmentations were used to mask the velocities, calculate WSS and co-registration for quantification of abnormal hemodynamics4. Abnormally elevated velocity and WSS were defined as higher than the three-dimensional 95% confidence interval. Abnormally directed velocity and WSS were defined as vector angle differences higher than 120°. The aorta was subdivided in 6 regions of interest (ROIs) for total multiple linear regression with the scan specifics listed in table 1. A Wilcoxon rank sum test was used to test for differences between untreated patients and patients treated with aortic root replacement surgery. Independent predictors were defined as characteristics that were significant in the total model. Significance was defined as P<0.05 with Bonferonni correction of a factor six (6 ROIs). The 3D maps with abnormal hemodynamics were co-registered and added to yield 3D maps that show the incidence of abnormal hemodynamics2,3.Results
Figure 2 shows examples of maps with abnormal velocity and WSS magnitude and direction respectively. In table 2 the mean abnormal hemodynamics and its independent predictors are given for the 6 ROIs. Ascending elevated velocity was associated with aortic root repair, whereas elevated WSS was associated with aortic root repair and blood pressure characteristics. No independent predictors were found for abnormally directed hemodynamics. Post-surgery patients had significantly more elevated velocity and WSS than untreated patients in the inner and outer ascending aorta and arch and significantly more abnormally directed WSS in the inner curvature of the ascending aorta and outer curvature of the arch. In figure 3 the incidence maps are shown for abnormally elevated velocity and abnormally directed WSS. The maximum incidence for elevated velocity and WSS was 32% and 20%, respectively, and found in the ascending aorta. The maxima for abnormally directed velocity and WSS were 18% and 39%, respectively, and found in the inner proximal descending aorta.Discussion
Altered aortic geometry and wall properties in Marfan patients had detectable hemodynamic effects in 30% of our Marfan cohort at known predilection sites for aortic dissection. Indeed, Marfan syndrome is characterized by great variety in phenotypical penetrance. Interestingly, the finding of abnormally directed hemodynamics5,6 in the proximal descending aorta was confirmed by the comparison methodology used here. This finding did not correlate with any aortic diameter or blood pressure characteristics, so this parameter may be an new independent indicator for localized aortic disease. Potentially, the abnormal hemodynamics in the proximal descending aorta are a consequence of abnormal aortic pulse wave velocity, shape or motion, which remains to be investigated.Conclusion
In this study we investigated abnormal hemodynamics in a cohort of Marfan patients by comparison with healthy subjects. We found that the incidence of abnormal elevated and directed hemodynamics was 30% of the cohort. Abnormalities in velocity and WSS magnitude mostly related to aortic diameters and blood pressure, whereas no relations with these characteristics were found for abnormally directed velocity and WSS. Altered hemodynamics were localized at predilection sites for aortic dissection in Marfan patients.Acknowledgements
No acknowledgement found.References
1. van Ooij, P. et al. Characterization of Abnormal Wall Shear Stress Using 4D Flow MRI in Human Bicuspid Aortopathy. Ann. Biomed. Eng. 43, 1385–1397 (2015). 2. van Ooij, P. et al. Fully quantitative mapping of abnormal aortic velocity and wall shear stress direction in patients with bicuspid aortic valves and repaired coarctation using 4D flow CMR. J Cardiovasc Magn Reson Accepted December 15th (2020). 3. Farag, E. S. et al. Aortic valve stenosis and aortic diameters determine the extent of increased wall shear stress in bicuspid aortic valve disease. J. Magn. Reson. Imaging 48, 522–530 (2018). 4. van Ooij, P. et al. A methodology to detect abnormal relative wall shear stress on the full surface of the thoracic aorta using four-dimensional flow MRI. Magn. Reson. Med. 73, 1216–1227 (2015). 5. van der Palen, R. L. F. et al. Altered aortic 3D hemodynamics and geometry in pediatric Marfan syndrome patients. J. Cardiovasc. Magn. Reson. 19, 30 (2017). 6. Geiger, J. et al. Longitudinal Evaluation of Aortic Hemodynamics in Marfan Syndrome: New Insights from a 4D Flow Cardiovascular Magnetic Resonance Multi-Year Follow-Up Study. J. Cardiovasc. Magn. Reson. 19, 33 (2017).Figures
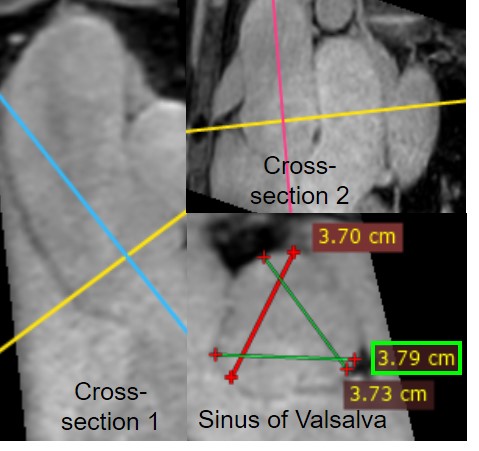
Figure 1. Aortic diameter measurements on 3D
Dixon images. An example for the sinus of Valsalva is displayed.
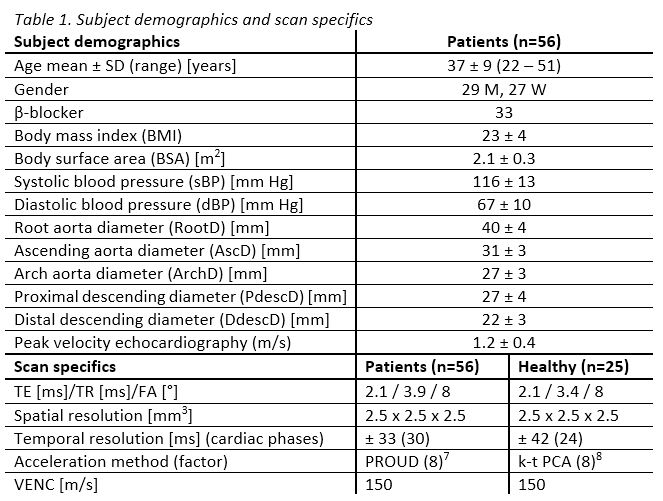
Table 1. Subject demographics and scan specifics
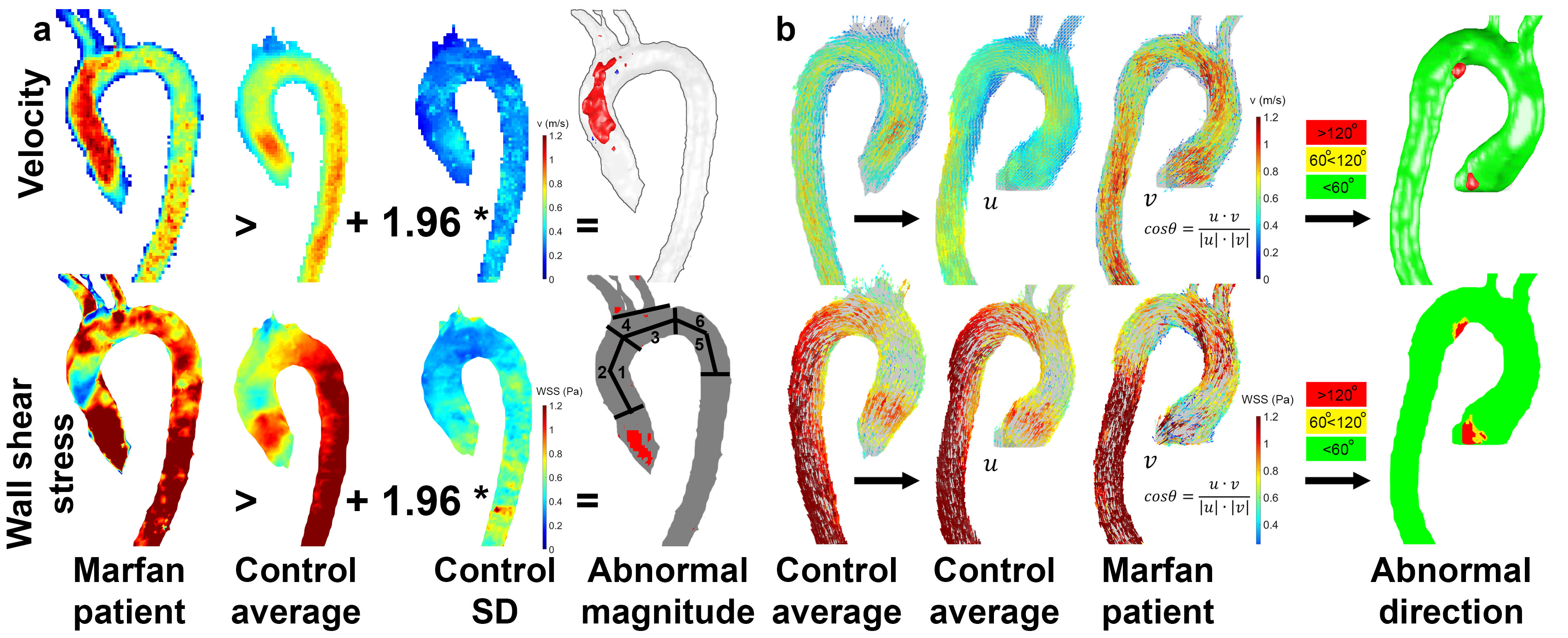
Figure 2. a) Maps showing abnormally elevated
velocity and WSS (a) are created by comparison with the control averaged and SD
velocity and WSS maps. Regions of interest 1-6 are indicated in the WSS maps.
b) Maps showing abnormally directed velocity and WSS are created by comparison
with the control averaged velocity and WSS maps.
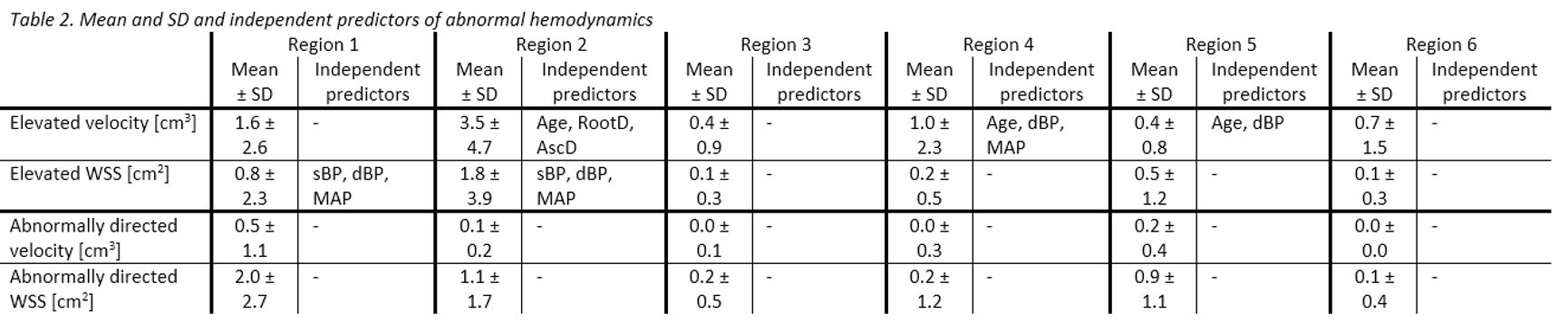
Table 2. Mean and SD and independent predictors of
abnormal hemodynamics
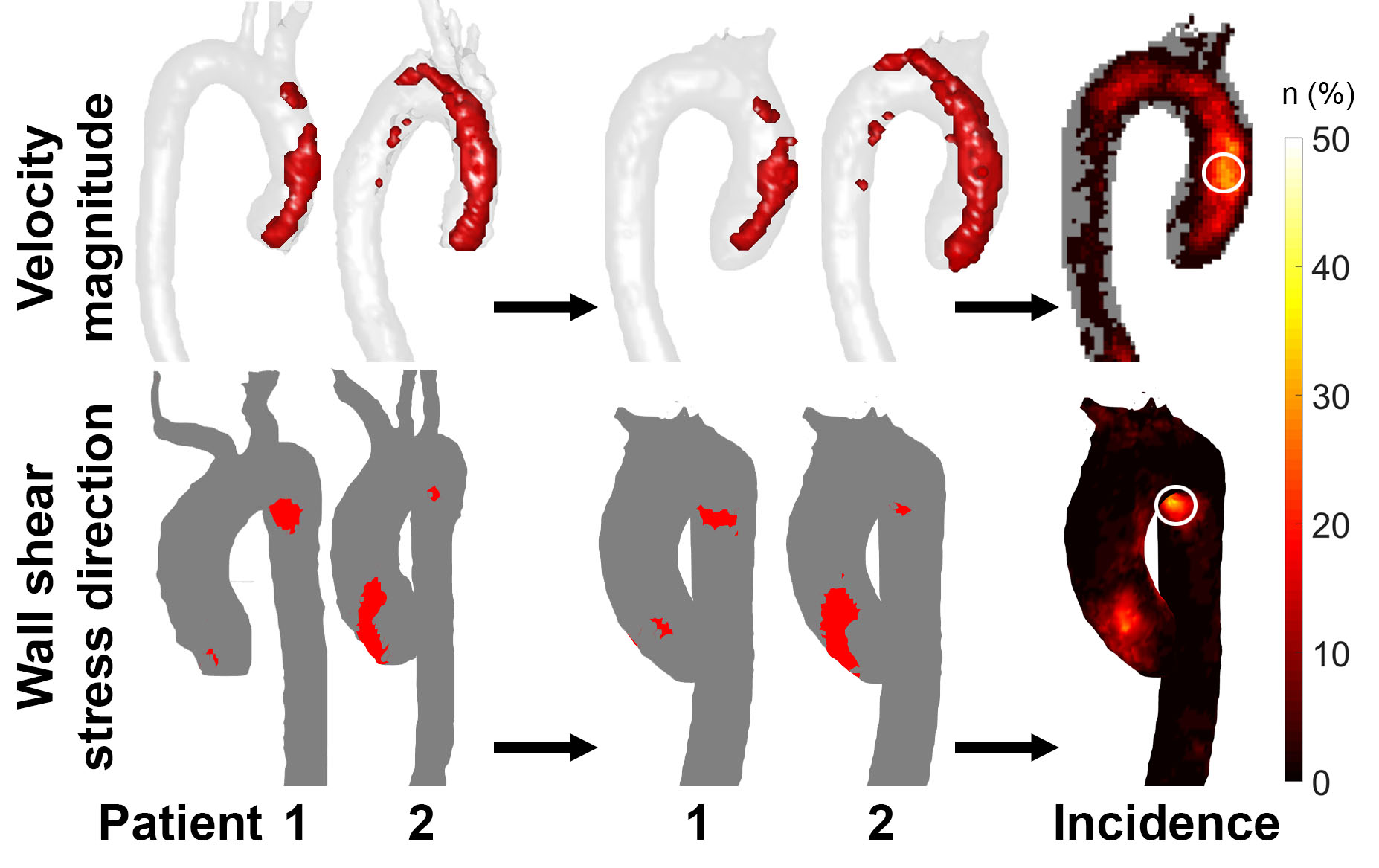
Figure 3. Maps for abnormally elevated velocity
(top) and abnormally directed WSS (bottom) in the Marfan cohort. Maximum
incidence is delineated in the white circles.