0309
Abnormal aortic kinetic energy and viscous energy loss in patients with repaired tetralogy of Fallot
Yu-Ru Yang1, Meng-Chu Chang1, Ming-Ting Wu2, Ken-Pen Weng3, and Hsu-Hsia Peng1
1Biomedical Engineering and Environmental Sciences, National Tsing Hua University, Hsinchu, Taiwan, 2Radiology, Kaohsiung Veterans General Hospital, Kaohsiung, Taiwan, 3Pediatrics, Kaohsiung Veterans General Hospital, Kaohsiung, Taiwan
1Biomedical Engineering and Environmental Sciences, National Tsing Hua University, Hsinchu, Taiwan, 2Radiology, Kaohsiung Veterans General Hospital, Kaohsiung, Taiwan, 3Pediatrics, Kaohsiung Veterans General Hospital, Kaohsiung, Taiwan
Synopsis
We aim to evaluate aortic kinetic energy (KE) and viscous energy loss (EL) in repaired tetralogy of Fallot (rTOF) patients with different degrees of aortic regurgitation fraction (RF). The rTOF1 group (RF<2%) demonstrated decreased systolic KE in arch and descending aorta, suggesting the mild altered aortic flow. The rTOF2 group (RF≧2%) presented significantly elevated RF in arch and descending aorta, increased systolic KE from distal ascending aorta to proximal descending aorta, and decreased systolic EL in ascending aorta and distal arch. In conclusion, the systolic KE may provide earlier evidence of abnormal aortic flow before serious aortic regurgitation.
Introduction
Aortic dilatation and regurgitation are prevalent in patients with repaired tetralogy of Fallot (rTOF) [1]. Aortic regurgitation may contribute to progressive aortic root dilatation in rTOF patients [2]. Recently, pathologic conditions such as regurgitation or aneurysm were reported to cause additional aortic viscous energy loss (EL), describing the friction produced by fluid viscosity, and consequently result in ventricular remodeling [3]. Secondary helices were found in ascending aorta of rTOF patients and abnormal aortic flow was associated with increased EL [4]. Ventricular kinetic energy (KE) was proposed to provide a new insight to assess ventricular performance in rTOF patients [5]. However, a systematic investigation of aortic regurgitation, KE and EL in patients with rTOF is deficient. The purpose of this study was to evaluate the aortic KE and EL in rTOF patients with different degrees of aortic regurgitation.Methods
The study population comprised 15 patients with rTOF (age 21.7±3.3 years, 7 females) and 12 age-matched normal volunteers (age 21.3±0.6 years, 6 females). The 4D flow data were acquired in a 3 Tesla MR scanner (Tim Trio or Skyra, Siemens) with prospective ECG-triggering (acquire 85%-90% of RR interval) and navigator-gating to synchronize with heartbeat and respiratory motion, respectively. Typical scanning parameters were: TR/TE=10.8/2.9 ms, voxel size=3.2x1.4x3.5 mm3, flip angle=7°, Venc=150 cm/s, and temporal resolution=41.6 ms. Fourteen planes were localized perpendicularly to the long-axis of aorta in the 4D flow data-derived MR angiography (Figure 1a). The rTOF patients were divided to rTOF1 group (n=8) with aortic regurgitation fraction (RF)<2% and rTOF2 group (n=7) with RF≧2%. The threshold of 2% was decided by the mean+standard deviation of RF of the 14 planes along the aorta in normal group. The regions-of-interest (ROI) of the aortic lumen were manually determined in magnitude images and transferred to phase images for computation of aortic flow. The aortic peak diameter index is the maximum aortic diameter during the cardiac cycle normalized by body surface area. The aortic RF was calculated by (Figure 1b): $$RF=\frac{retorgrade flow}{antegrade flow}\times100%$$The systolic KE was calculated by (Figure 1c): $$KE=\frac{1}{2}{\rho}Vv^{2}$$ where V is the volume of voxel, v is velocity and ρ is the blood density with a value of 1060 kg/m3. The aortic EL of each time frame was calculated by: $$Φv=\frac{1}{2}\sum_i\sum_j{[(\frac{\partial v_{i}}{\partial v_{j}}+\frac{\partial v_{j}}{\partial v_{i}})-\frac{2}{3}(\triangledown{v})\delta_{ij}]}^{2}, where δij=1 for i=j, δji=0 for i≠j, EL=\mu\sum_{i=1}^{num voxel}ΦvVi $$where Φv is the rate of viscous energy dissipation of each voxel, i and j represent the principal directions x, y, z, and μ is the viscosity of blood as 0.004 Pa·s in Newtonian fluid. The aortic systolic EL was computed by the integration of EL during systolic phases (Figure 1d). Student t test was performed when appropriate p<0.05 was considered statistically significant.Results
The demographics and hemodynamic characteristics in normal and two rTOF groups were summarized in Table 1. Compared to normal group, both rTOF1 and rTOF2 groups exhibited dilated indexed right ventricular end diastolic (p<0.001 and p=0.004) and systolic (both p=0.002) volumes. The rTOF2 group showed significantly lower right ventricular ejection fraction than normal and rTOF1 groups (both p<0.05). In Figure 2, both rTOF1 and rTOF2 groups presented increased peak diameter index at ascending aorta (p<0.05). Solely in rTOF2 group, patients exhibited higher RF in aortic arch and descending aorta (p<0.05) than that in normal and rTOF1 groups. In comparison to normal group, both rTOF subgroups demonstrated decreased systolic KE in planes of aortic arch and descending aorta (p<0.05); meanwhile, rTOF2 group also displayed reduced systolic KE in distal ascending aorta (p<0.05). As for systolic EL, only the rTOF2 group presented significantly decreased systolic EL in ascending aorta and distal aortic arch (p<0.05).Discussion and conclusion
In this study, rTOF2 group presented significantly dilated ascending aorta, elevated RF in arch and descending aorta, increased systolic KE from distal ascending aorta to proximal descending aorta, and decreased systolic EL in ascending aorta as well as in distal arch. The rTOF1 group, who possess comparable RF with normal group, only demonstrated increased diameter in ascending aorta and decreased systolic KE in arch and descending aorta, suggesting the mild altered aortic flow. Viscous energy loss, which is formed by the friction between moving blood and vessel walls, is unavoidable but can be reduced by slight increase in the radius of the vessel [3]. Therefore, we speculated that the increase of aortic diameter might lead to reduced systolic EL in rTOF2 group, particularly in ascending aorta. Intraventricular kinetic energy is required to generate flow and may provide earlier evidence of ventricular dysfunction [5]. In this study, we further investigated the aortic KE in rTOF patients. We found that the rTOF1 group presented normal RF and preserved systolic EL while the systolic KE in planes from arch to descending aorta already exhibited decreased systolic KE, suggesting that systolic KE might be an earlier indication for altered aortic flow patterns. In conclusion, the systolic KE in aorta may provide earlier evidence of abnormal aortic flow before serious aortic regurgitation and altered energy loss.Acknowledgements
No acknowledgement found.References
[1] Capelli, Horacio, Donald Ross, and Jane Somerville. "Aortic regurgitation in tetrad of Fallot and pulmonary atresia." The American Journal of Cardiology 49.8 (1982): 1979-1983. [2] Dodds III, G. Alfred, Carole A. Warnes, and Gordon K. Danielson. "Aortic valve replacement after repair of pulmonary atresia and ventricular septal defect or tetralogy of Fallot." The Journal of thoracic and cardiovascular surgery 113.4 (1997): 736-741. [3] Akins, Cary W., Brandon Travis, and Ajit P. Yoganathan. "Energy loss for evaluating heart valve performance." The Journal of thoracic and cardiovascular surgery 136.4 (2008): 820-833. [4] Schäfer, Michal, et al. "Abnormal aortic flow conduction is associated with increased viscous energy loss in patients with repaired tetralogy of Fallot." European Journal of Cardio-Thoracic Surgery 57.3 (2020): 588-595. [5] Jeong, Daniel, et al. "Ventricular kinetic energy may provide a novel noninvasive way to assess ventricular performance in patients with repaired tetralogy of Fallot." The Journal of thoracic and cardiovascular surgery 149.5 (2015): 1339-1347. [6] Barker, Alex J., et al. "Viscous energy loss in the presence of abnormal aortic flow." Magnetic resonance in medicine 72.3 (2014): 620-628. [7] Maurer, Gerald. "Aortic regurgitation." Heart 92.7 (2006): 994-1000.Figures
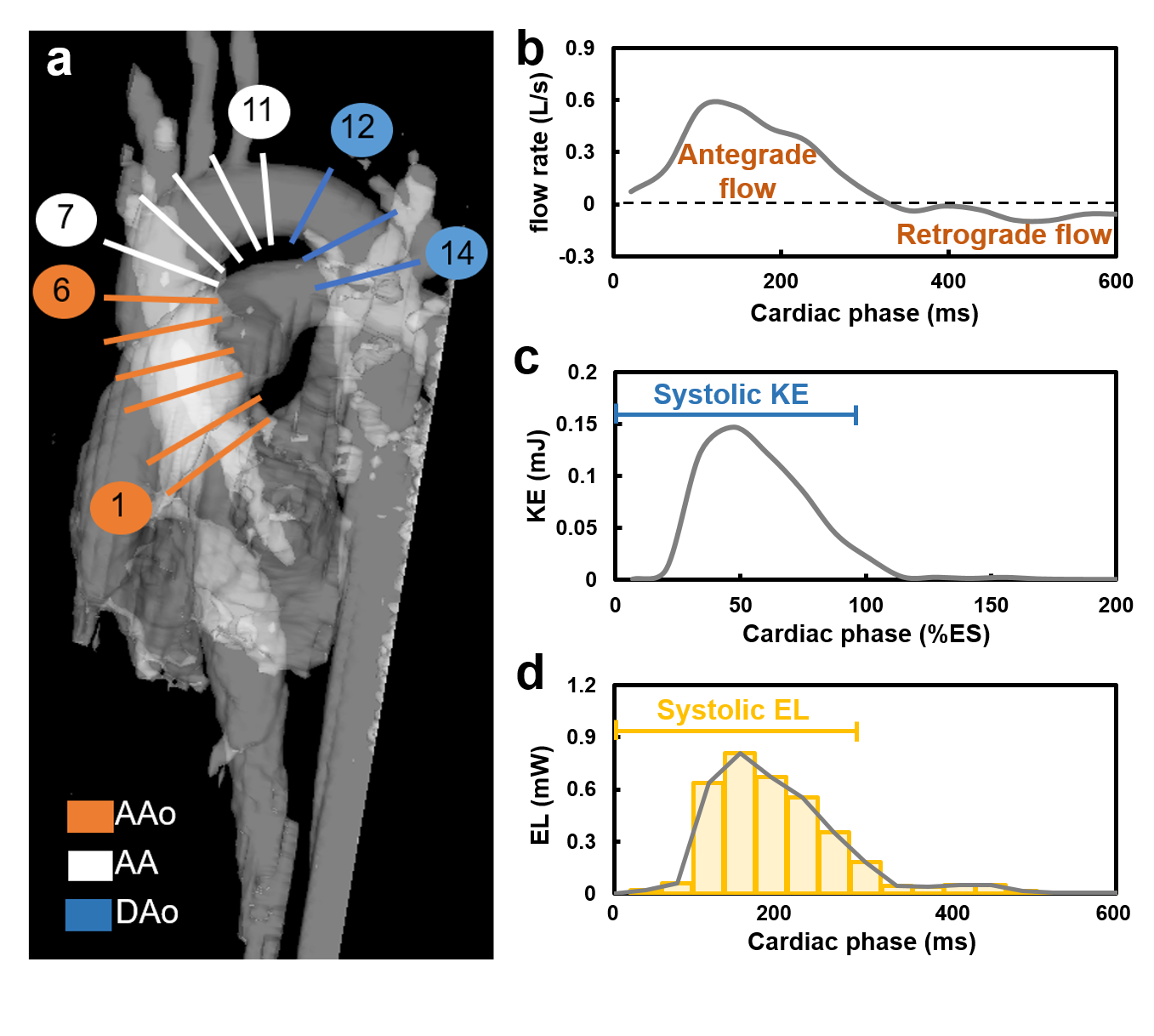
Figure 1.
(a)
Fourteen planes were localized perpendicularly to the long-axis of aorta in the
4D flow data-derived MR angiography. The definition of regurgitation fraction,
systolic kinetic energy, and systolic energy loss were displayed in the
representative time course of flow rate (b), kinetic energy (c) and viscous
energy loss (d) of plane 1 in one normal volunteer.
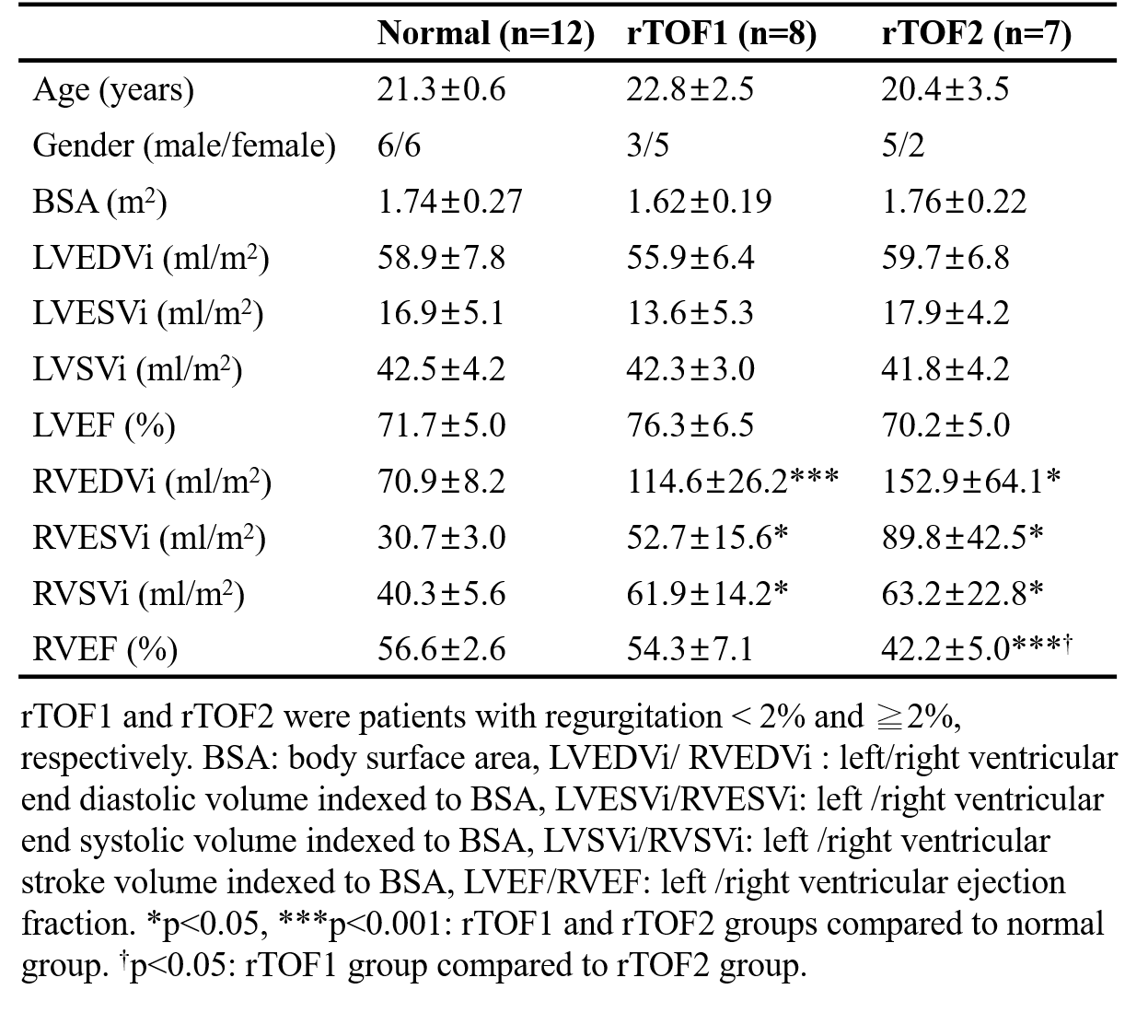
Table 1. Demographic
characteristics
of the study population.
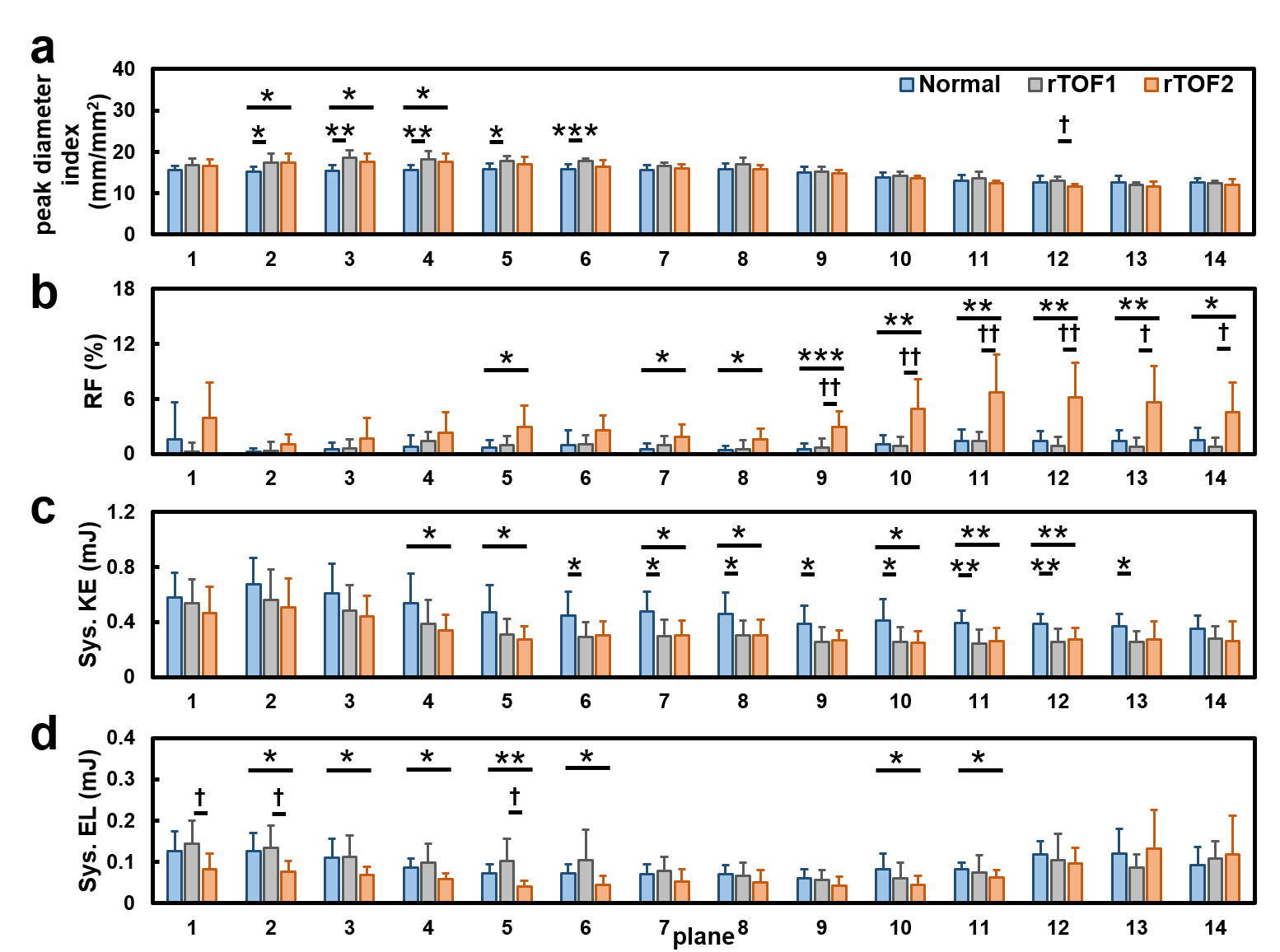
Figure 2.
The
(a) peak diameter index, (b)
regurgitation fraction, (c) systolic kinetic energy and (d) systolic viscous
energy loss in 14 planes of normal, rTOF1, and rTOF2 groups.
*p<0.05, **p<0.01, ***p<0.001,
rTOF1 and rTOF2 patients compared to normal volunteers.
†p<0.05,
† † p<0.01, † † † p<0.001, rTOF1 patients compared to
rTOF2 patients.