0307
Insight of right ventricular dysfunction and impaired efficiency via 4D flow CMR in repaired tetralogy of Fallot
Xiaodan Zhao1, Liwei Hu2, Ru-San Tan1,3, Ping Chai4, Marielle Fortier3,5, Rong Zhen Ouyang2, Shuo Zhang6, Wen Ruan1, Ting Ting Low4, Shuang Leng1, Jun-Mei Zhang1,3, Bryant Jennifer1, Lynette Teo4, Rob van der Geest7, Teng Hong Tan3,5, James W. Yip4, Ju Le Tan1,3, Yumin Zhong2, and Liang Zhong1,3
1National Heart Centre Singapore, Singapore, Singapore, 2Shanghai Children’s Medical Centre, Shanghai, China, 3Duke-NUS Medical School, Singapore, Singapore, 4National University Hospital Singapore, Singapore, Singapore, 5KK Women’s and Children’s Hospital, Singapore, Singapore, 6Philips Germany, Humburg, Germany, 7Leiden University Medical Center, Leiden, Netherlands
1National Heart Centre Singapore, Singapore, Singapore, 2Shanghai Children’s Medical Centre, Shanghai, China, 3Duke-NUS Medical School, Singapore, Singapore, 4National University Hospital Singapore, Singapore, Singapore, 5KK Women’s and Children’s Hospital, Singapore, Singapore, 6Philips Germany, Humburg, Germany, 7Leiden University Medical Center, Leiden, Netherlands
Synopsis
4D flow CMR enables qualitative and quantitative assessment of intra-cardiac flow. Kinetic energy (KE) and pathline-derived four flow components for left ventricular (LV) and right ventricular (RV) were analyzed and compared in repaired tetralogy of Fallot (rTOF) and age-matched controls. For RV, rTOF had increased peak systolic, systolic and peak E-wave KE normalized to end-diastolic volume while decreased efficiency index. RV direct flow decreased while RV residual volume increased from controls to rTOF with preserved RVEF (rTOFpEF) to rTOF with reduced RVEF. ROC analysis showed RV direct flow and efficiency index were sensitive markers to detect RV dysfunction in rTOFpEF.
Introduction
Four-dimensional flow cardiovascular magnetic resonance (4D flow CMR) allows quantification of biventricular blood by flow components and kinetic energy (KE) analyses generating unique insights for comprehensive hemodynamic assessment. This study aimed to compare the differences of 4D flow parameters for left ventricle (LV) and right ventricle (RV) in repaired tetralogy of Fallot (rTOF) and age-matched controls, and identify sensitive markers to differentiate rTOF with preserved RV ejection fraction (EF) from controls.Methods
54 rTOF patients (14 pediatric, 40 adult; age 29 ± 16 years; 26M:28F) and 54 age-matched controls (14 pediatric, 40 adult; age 31 ± 16 years; 27M:27F) were recruited from four centers. CMR acquisition was performed using 3.0T Ingenia (Philips Healthcare, he Netherlands), 1.5T Magneton Tim Trio (Siemens Medical Solutions, Erlangen, Germany), and 3.0T (GE Healthcare, Waukesha, WI) magnetic resonance scanners. Typical 4D flow scanning parameters are summarized in Figure 1. Volumetric, 2D phase-contrast flow and 4D flow analyses were performed using MASS software (Leiden University Medical Center, Leiden, The Netherlands). Individual pathlines were generated from velocity vectors for all voxels found within the segmented LV or RV endocardial borders. Depending on pathline trajectories within the LV or RV during the analyzed cardiac cycle, four flow components were discernible: (1) direct flow enters and exits the chamber in the same cycle; (2) retained inflow enters but does not exit the chamber during the cycle; (3) delayed ejection flow starts within the chamber and exits during the cycle; and (4) residual volume remains in the chamber for at least two cycles. LV and RV flow components were indexed to LV or RV end-diastolic volumes (EDV), respectively. For each voxel, kinetic energy (KE) was calculated as KE=1/2·ρblood·Vvoxel·v2, where ρblood is blood density (1.06 g/cm3); Vvoxel, voxel volume; and v, velocity magnitude. By summing individual voxel KE values across all time points, the total KE throughout the cardiac cycle is obtained. All KE parameters are normalized to EDV (KEiEDV) with units expressed in μJ/ml. KEiEDV parameters - peak systole, average systole and peak E-wave - were extracted from the time-resolved KE curve (Figure 2). In the RV, we defined efficiency index = effective cardiac index/RV systolic KEiEDV, where effective cardiac index = effective cardiac output/body surface area and effective cardiac output = heart rate x (RV stroke volume – pulmonary backward flow). rTOF patients were stratified into preserved RV ejection fraction (EF) ≥45% and reduced RVEF <45% groups for comparison. Statistical analysis was performed using SPSS 22, and P value <0.05 was considered significant.Results
4D flow analysis was feasible in all subjects. See Figure 3 and Figure 4 for results. rTOF patients had significantly greater RV volumes and lower RVEF, effective cardiac output and effective cardiac index compared with controls. rTOF patients had significantly lower RV direct flow and efficiency index, higher RV residual volume, peak systolic, systolic, and peak E-wave KEiEDV, lower LV delayed ejection flow, higher LV retained inflow and peak E-wave KEiEDV than controls (all P<0.05). RV direct flow progressively decreased and RV residual volume progressive increased from controls to rTOF with preserved EF to rTOF with reduced EF (all P<0.05). ROC analysis showed that RV direct flow and efficiency index were more sensitive (AUC=0.805 and 0.806) for discriminating rTOF with preserved EF from controls (Figure 5).Conclusion
RV kinetic energy and flow components analysis from 4D flow CMR in rTOF patients showed that reduced efficiency index and RV direct flow were superior to traditional measurements for discriminating rTOF with preserved RVEF from controls.Acknowledgements
No acknowledgement found.References
No reference found.Figures
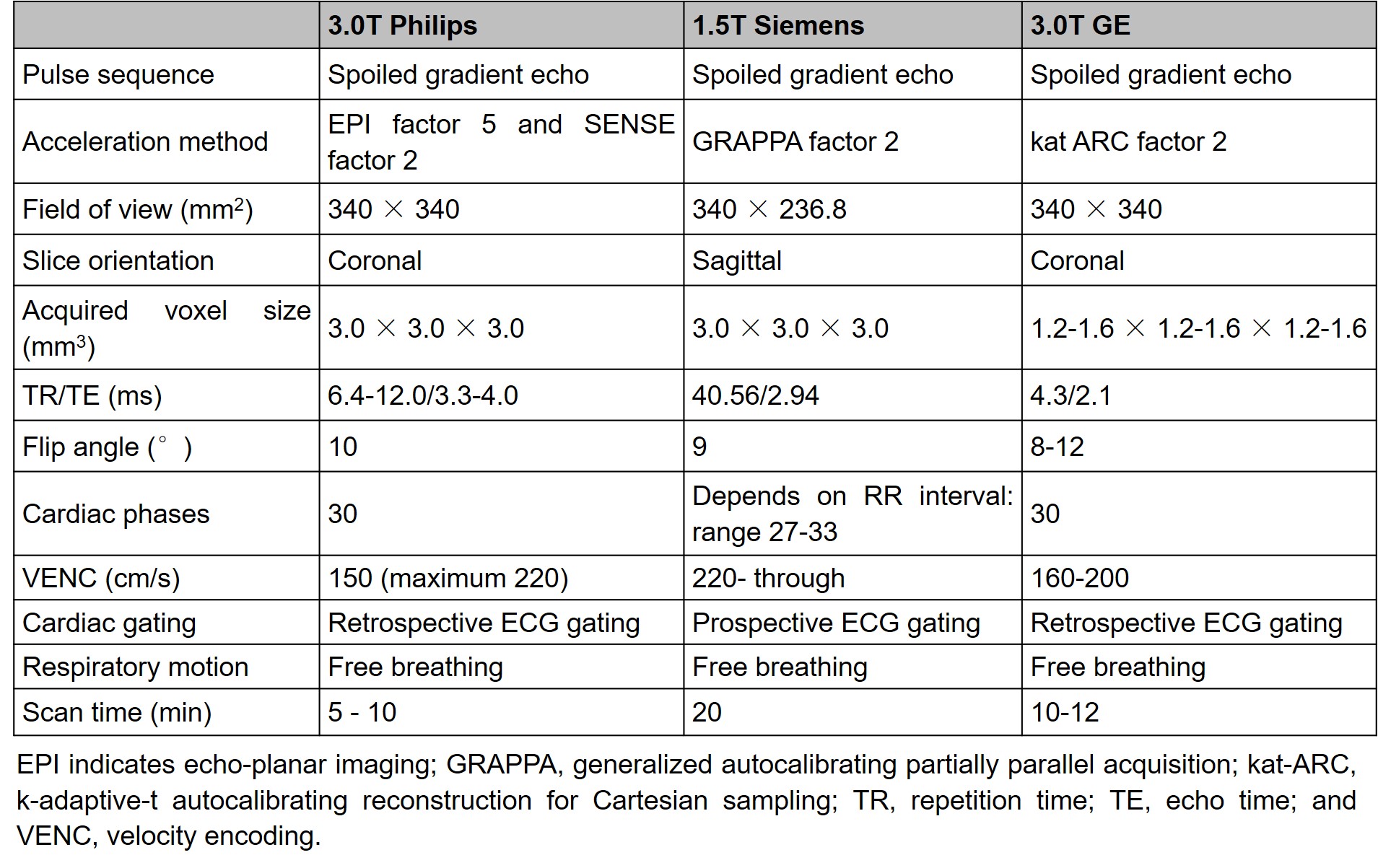
Acquisition parameters of 4D
flow CMR imaging in different centers.
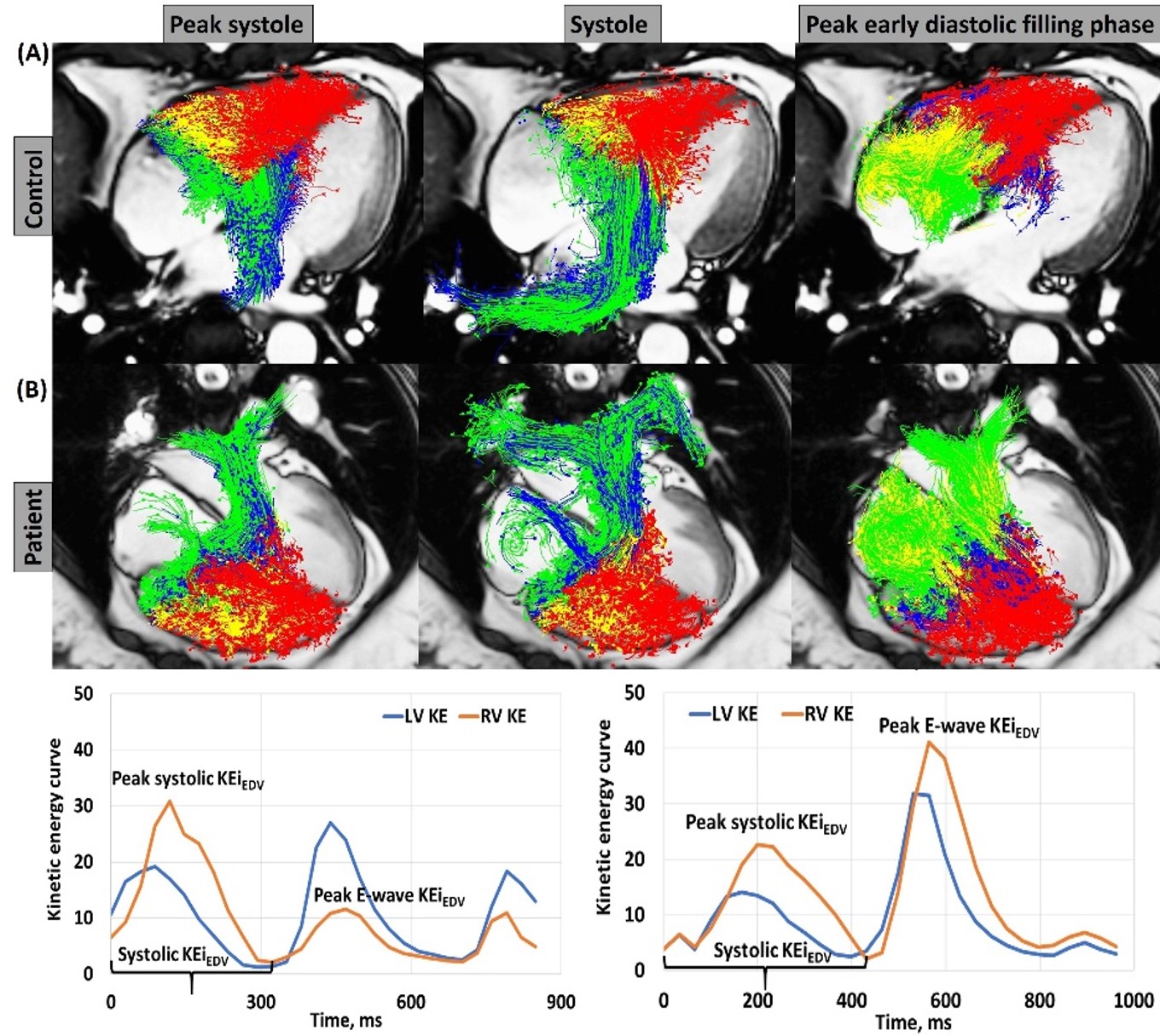
Four-chamber views with particle tracing overlayed at peak
systole, systole and peak early diastolic filing (top) and LV/RV
kinetic energy (KE) curve normalized to end-diastolic volume (KEiEDV)
(lower) in a 46-year-old male control (A) and a 25-year-old female rTOF
(B). Red color: residual volume; blue color: delayed ejection flow; yellow
color: retained inflow; green color: direct flow. Peak systolic KEiEDV, peak KEiEDV of blood flow during systole; systolic KE, average
KEiEDV of blood flow during systole; peak E-wave KEiEDV, peak KEiEDV of blood flow during early mitral filling.
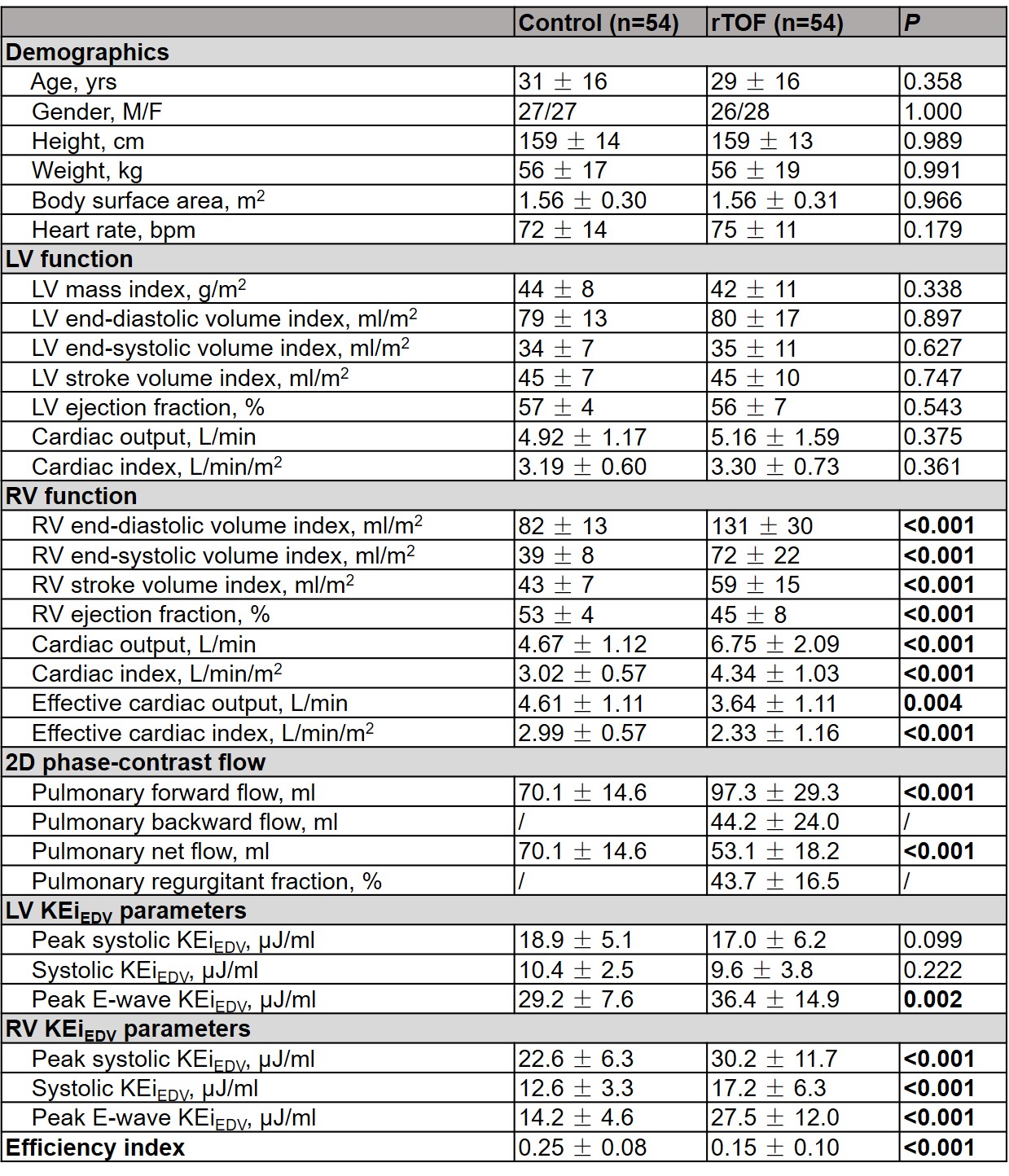
Demographics, left ventricular (LV) and right ventricular (RV)
flow analysis parameters in controls and repaired tetralogy of Fallot (rTOF)
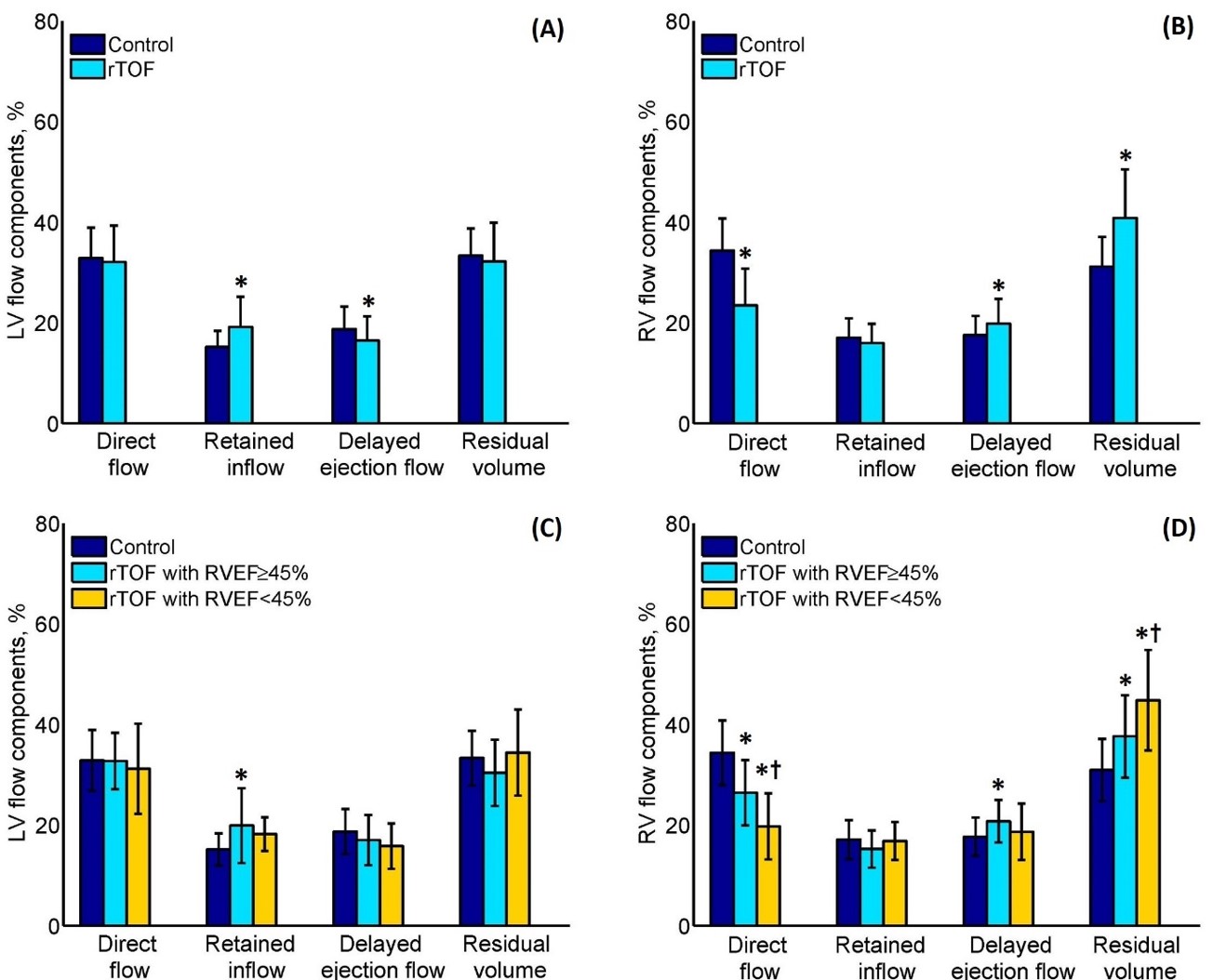
Comparison of left ventricular (LV) and
right ventricular (RV) flow components between repaired tetralogy of Fallot
(rTOF) and controls (A)-(B), and between rTOF with RV ejection fraction
(EF)≥45%, RVEF<45% and controls (C)-(D). *Significant difference compared
with control; †significant
difference compared with rTOF with RVEF≥45%.
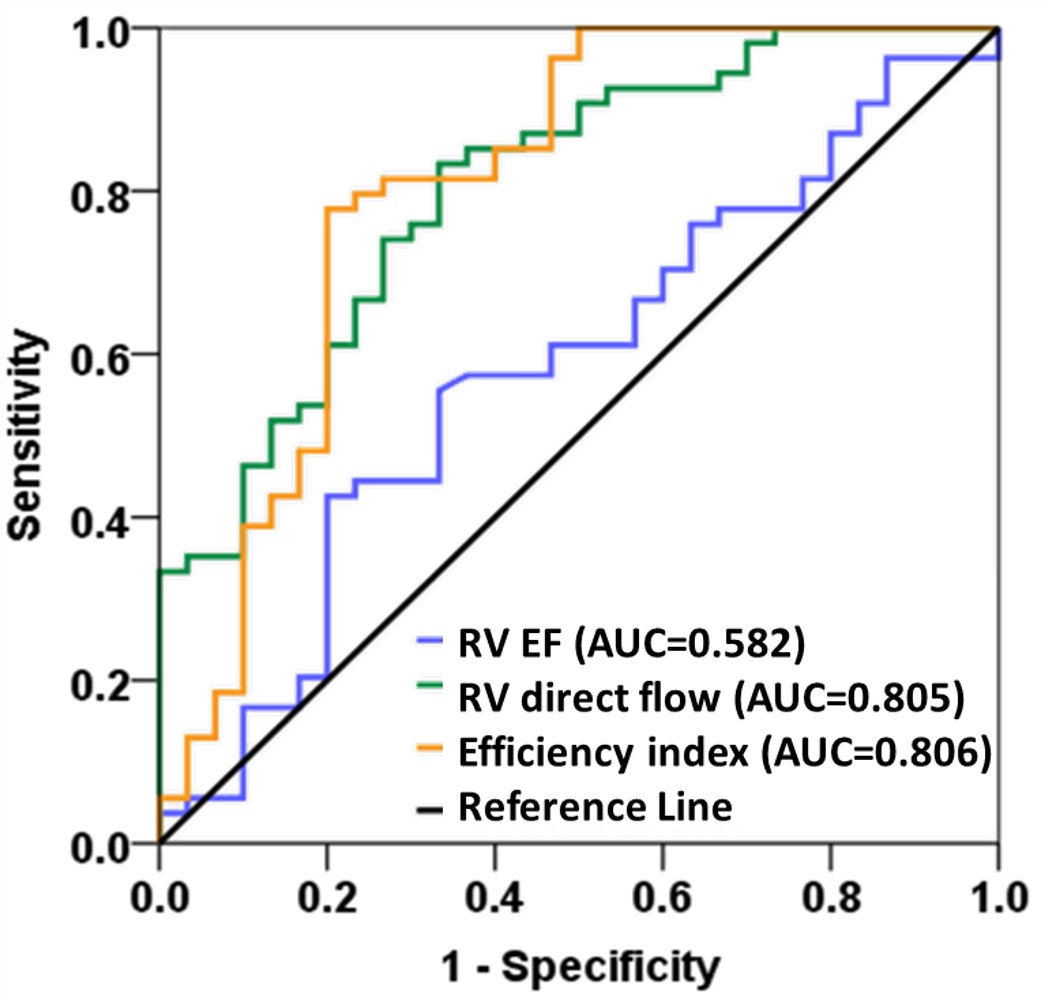
Detection of rTOF with preserved EF: ROC curves
comparing the diagnostic performance of RV direct flow, efficient index and RV
EF with respective AUC values. rTOF: repaired tetralogy of Fallot; EF: ejection
fraction; RV: right ventricle; efficiency index: effective cardiac index/RV
systolic KEiEDV; KEiEDV: kinetic energy normalized to
end-diastolic volume.