0305
Impact of respiratory Gating on hemodynamic parameters from 4D flow MRI1Biomedical Imaging Center, Pontificia Universidad Católica de Chile, Santiago, Chile, 2Electrical Engineering Department, School of Engineering, Pontificia Universidad Católica de Chile, Santiago, Chile, 3ANID – Millennium Science Initiative Program – Millennium Nucleus for Cardiovascular Magnetic Resonance, Santiago, Chile, 4School of Biomedical Engineering, Universidad de Valparaíso, Valparaíso, Chile, 5Department of Radiology, School of Medicine, Pontificia Universidad Católica de Chile, Santiago, Chile
Synopsis
Hemodynamic parameters from 4D flow datasets derived in the last years have shown promising diagnostic value in different cardiovascular pathologies. However, we know little about the behavior of these parameters when the 4D flow data is corrupted by respiratory motion. The purpose of this work is to perform a quantitative comparison between hemodynamic parameters computed from 4D flow Cardiac MRI with and without respiratory self-gating. We found significant variability of the hemodynamic parameters in the ascending aorta of healthy volunteers when comparing both methods. Hemodynamic parameters measured with self-gating acquisition showed statistically significant differences compared to those measured without self-gating.
INTRODUCTION
4D flow data allow the computation of advanced hemodynamic parameters that provide valuable information to characterize cardiovascular diseases. However, the computed parameters are sensitive to changes in resolution, SNR settings, and motion compensation of the 4D flow acquisition1.In order to reduce motion artifacts, 4D flow is often acquired with respiratory self-gating2. However, this significantly increases the acquisition time of an already long 4D flow scan. Despite respiratory self-gating reduces the motion artifacts, the quantitative impact on the hemodynamic parameters remains unclear.
The purpose of this work is to perform a quantitative comparison of the precision of hemodynamic parameters obtained from 4D flow MRI data acquired with and without respiratory self-gating. This comparison will allow to evaluate whether it is worth lengthening the scan in order to have respiratory self-gating.
METHODS
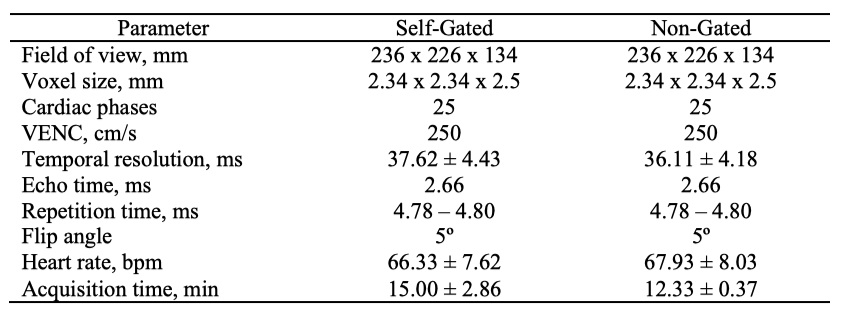
We considered 4D flow MRI data retrospectively acquired from 15 healthy volunteers (10 men and 5 women, 30.40 ± 6.23 years of age) acquired at 3T. The respiratory self-gated strategy consisted in a continuous acquisition of the k0-profile and a cross correlation to determine the respiratory positions3. A window of 7 mm was used to accept the data during expiration3. A summary of the acquisition parameters is shown in the table of Figure 1.Both 4D Flow MRI data sets (with and without respiratory self-gating) were post-processed using an in-house MATLAB toolbox (MathWorks, Natick, MA, USA). The image processing steps involved segmentation of the thoracic aorta and generation of a tetrahedral finite element mesh (characteristic length 1 mm)4. Velocity, Wall Shear Stress (WSS), Wall Shear Stress Axial (WSSA), Wall Shear Stress Circumferential (WSSC), vorticity, viscous dissipation, kinetic energy, and energy loss were obtained from 4D flow images of the thoracic aorta. These parameters have shown potential importance for diagnostic. Angiographic 4D flow images were segmented using a semiautomatic process, based on thresholding, labeling, and manual separation of vessels. The analysis was performed at the peak systolic phase.
We calculated the DICE coefficient5 between the segmentations of the data obtained with and without respiratory self-gating and the local differences between the mesh surfaces of each section. The local differences between both meshes were calculated using the Euclidean distance6.
We analyzed the mean, standard deviation and coefficient of variation (CV) of each hemodynamic parameter. Wilcoxon signed rank test and Bland-Altman plots were also performed between respiratory self-gated and non-gated data, using a statistical significance of 0.05.
RESULTS
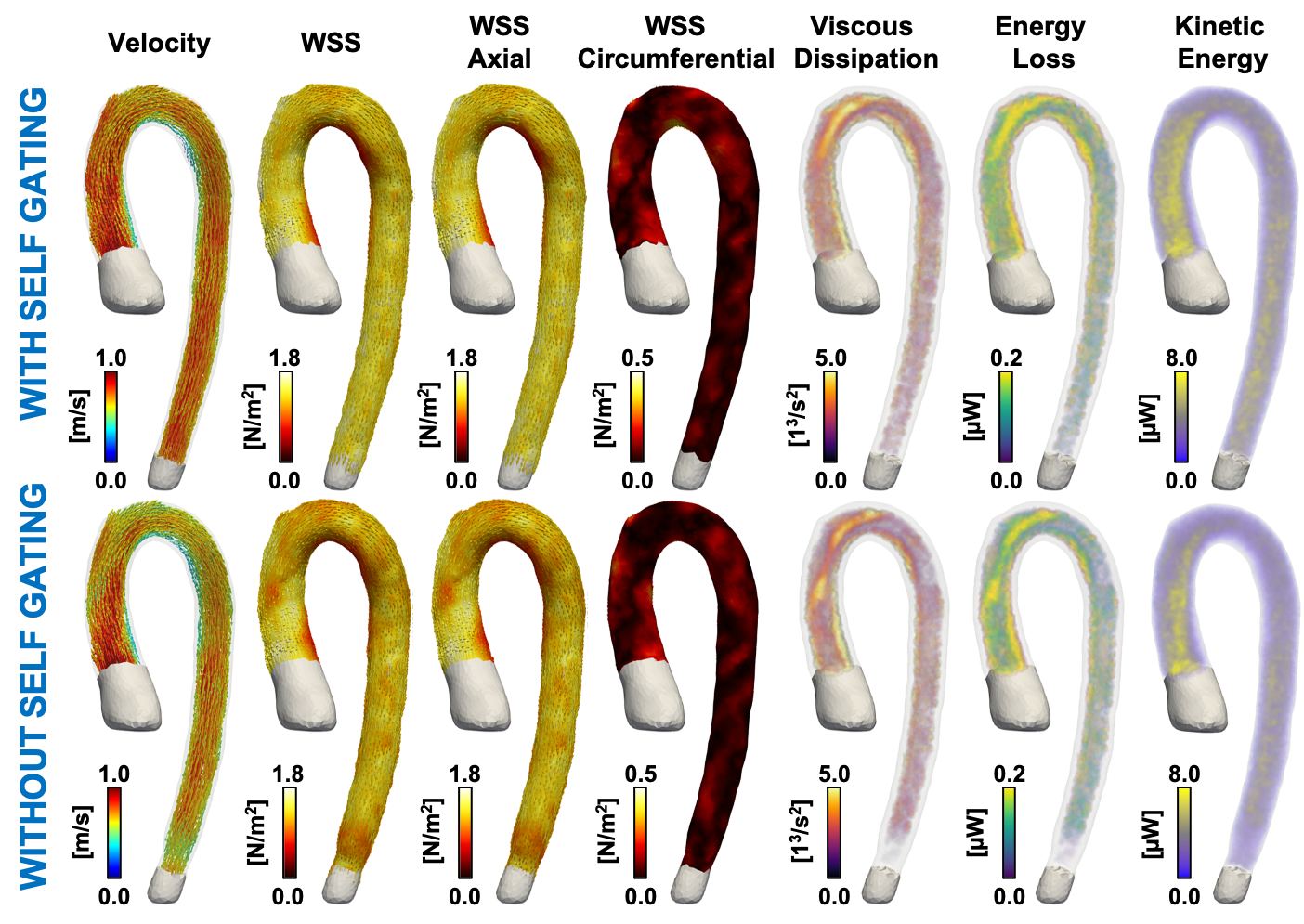
The mean and range of DICE coefficient between the segmentation of the self-gated and non-gated data were 0.918 ± 0.056. This result, which considered the whole segmented aorta, showed a high intersection between both segmentations. The local differences of both meshes showed an almost perfect agreement, with only few negligible discrepancies at both extremes of the aorta.Despite images with and without respiratory self-gating looked similar, they showed differences in WSS, viscous dissipation, energy loss and kinetic energy (Figure 2).
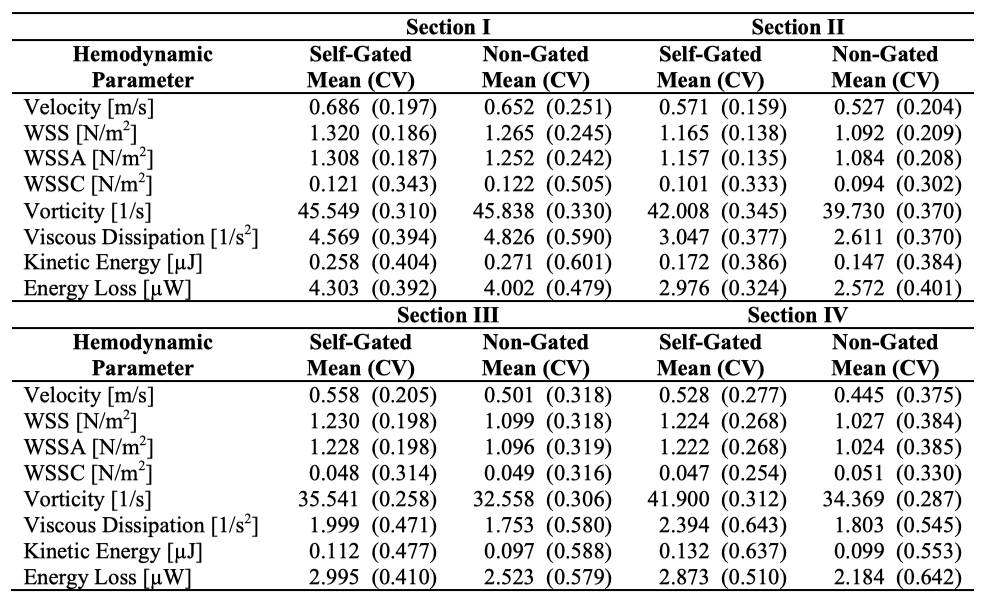
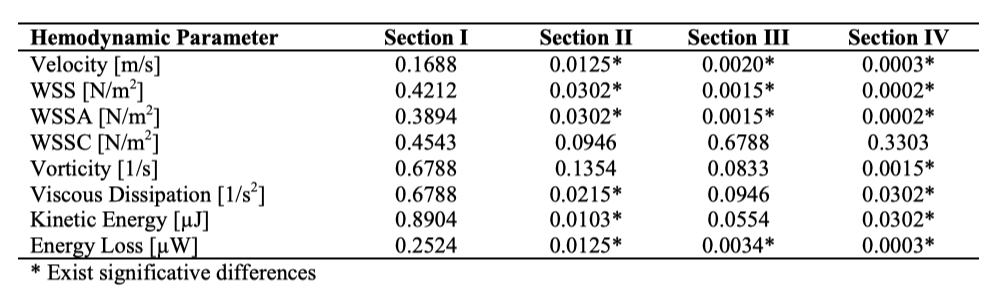
The mean and CV of hemodynamic parameters at each section of the aorta (Figure 3) showed significant differences (Figure 4) between respiratory self-gating and non-respiratory gating in sections II, III, and IV. Differences in velocity, WSS, and WSSA were observed at section II, III, and IV. There were also statistical differences for viscous dissipation, kinetic energy and energy loss at Section II and IV.
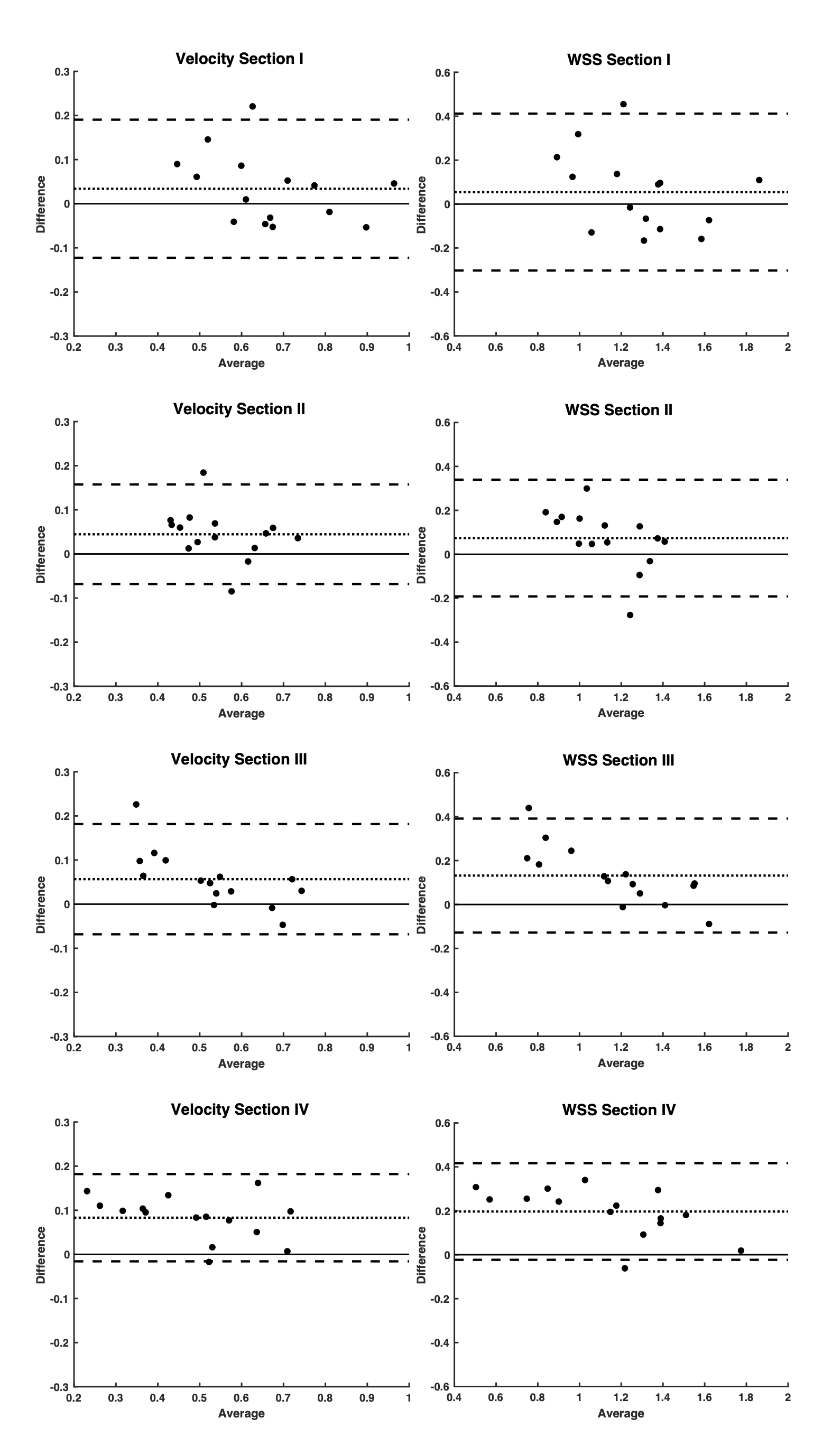
Bland Altman plots showed that hemodynamic parameters computed from 4D flow without respiratory self-gating increasingly underestimated the ones computed with self-gating along the sections (Figure 5).
CONCLUSION
In this work we compared hemodynamic parameters computed from thoracic aorta 4D flow MRI data obtained with and without respiratory self-gating.Segmentation variability analysis using DICE and local differences showed high intersection of both acquisitions, and thus, the variations in the parameter values introduce by the segmentation process is minimal.
The statistical analysis showed that the data obtained with self-gating have less variability than the data obtained without self-gating. The Wilcoxon signed rank test showed significant differences in most of the parameters measured between both acquisitions at sections II, III, and IV and minimal differences at section I (AAo). Nevertheless, measurements at section I showed greater variability for both methods.
We found that measurements of hemodynamic parameters from 4D flow data using self-gating acquisition showed statistical differences with measurement computed from acquisitions without respiratory compensation for aortic arch and descending and diaphragmatic aorta in healthy volunteers. Our results suggest that the use of respiratory motion compensation techniques is mandatory for the accurate evaluation of 4D flow hemodynamics parameters.
Acknowledgements
This work has been funded by ANID-PIA-ACT192064 and ANID – Millennium Science Initiative Program – NCN17_129. Also, FONDECYT # 1181057. Sotelo J. thanks to CONICYT - FONDECYT Postdoctorado 2017 #3170737. Andia M. thanks to FONDECYT # 1180525. Arrieta C. was partially funded by CONICYT FONDECYT Postdoctorado 2019 #3190763, CONICYT PCI REDES 180090, and ANID-FONDECYT de Iniciación en Investigación 2020 #11200481.References
1. Markl M, Frydrychowicz A, Kozerke S, Hope M, Wieben O. 4D flow MRI. Journal of Magnetic Resonance Imaging. 2012;36(5):1015-1036. doi:10.1002/jmri.23632
2. Montalba C, Urbina J, Sotelo J, et al. Variability of 4D flow parameters when subjected to changes in MRI acquisition parameters using a realistic thoracic aortic phantom. Magnetic Resonance in Medicine. 2018;79(4):1882-1892. doi:10.1002/mrm.26834
3. Uribe S, Beerbaum P, Sørensen TS, Rasmusson A, Razavi R, Schaeffter T. Four-dimensional (4D) flow of the whole heart and great vessels using real-time respiratory self-gating. Magnetic Resonance in Medicine. 2009;62(4):984-992. doi:10.1002/mrm.22090
4. Sotelo J, Dux-Santoy L, Guala A, et al. 3D axial and circumferential wall shear stress from 4D flow MRI data using a finite element method and a laplacian approach. Magnetic Resonance in Medicine. 2018;79(5):2816-2823. doi:10.1002/mrm.26927
5. Odille F, Steeden JA, Muthurangu V, Atkinson D. Automatic segmentation propagation of the aorta in real-time phase contrast MRI using nonrigid registration. Journal of Magnetic Resonance Imaging. 2011;33(1):232-238. doi:https://doi.org/10.1002/jmri.22402
6. Arrieta C, Uribe S, Ramos-Grez J, et al. Quantitative assessments of geometric errors for rapid prototyping in medical applications. Rapid prototyping journal. 2012;18(6):431-442.
Figures