0220
Assessing pulmonary findings of COVID-19 with ultrashort TE magnetic resonance imaging1Shanghai Public Health Clinical Center, Shanghai, China, 2Central Research Institute, United Imaging Healthcare, Shanghai, China
Synopsis
Chest computed tomography (CT) has played significant role in assessing the pulmonary findings of COVID-19. However, MRI, a radiation-free imaging technique has hardly been applied for assessing the pulmonary abnormalities of patients with COVID-19. Ultra shot echo time MRI (UTE-MR) is broadly regarded as a valuable tool for pulmonary imaging. This research, hence, aims to evaluate the COVID-19 with UTE-MR. The results indicated that there was no significant difference of image quality between the UTE-MR and CT for identifying the representative abnormalities. Besides, the intermethod agreement of UTE-MR and CT for assessing the pulmonary abnormalities were all determined excellent.
Introduction
As of December 13, there is a total of over 69,808,588 confirmed cases with COVID-19 in more than 220 countries. All humans have reached the consensus that this is an unprecedented serious worldwide public health crisis.1 At present, chest computed tomography (CT) examination is strongly encouraged for aiding the prevention and control of COVID-19. However, the potential bio-safety concerns were raised as CT is an ionizing imaging technique.2 Therefore, non-invasive image modality is thus of great clinical significance for evaluating the COVID-19. Although possessing the advantages of high soft-tissue resolution, radiation-free character and so on, the pulmonary application of magnetic resonance imaging (MRI) has been limited by fast signal decay caused by T2* effect, respiratory motions and relatively low proto content. Meaningfully, recent advances in ultrashort echo time MRI (UTE-MRI) have pave the way for evaluating the pulmonary structure and function with increased signal-to-noise ratio and less vulnerability to motion artefact.3,4 However, to the best of our knowledge, MRI has hardly been applied for evaluating the pulmonary findings of COVID-19. Therefore, in this study, we aimed to apply the UTE-MRI for evaluating the COVID-19 with the CT as a reference.Methods
A total of 20 patients with COVID-19 were included into this prospective study from February 2020 to April 2020. UTE-MR was based on a respiratory-gated three-dimensional (3D) sequence with the following parameters: repetition time (TR) = 2.2 ms, echo time (TE) = 0.08 ms, Flip angle (FA) = 3°, Field of View (FOV) = 350×350 mm2 and scanning matrix = 456×456. Image quality analysis: Both two groups of radiologists were asked to evaluate the image quality of CT and UTE-MR with the following 5-point scoring system (1: not diagnostically acceptable, 2: suboptimal/poor, 3: acceptable, 4: good and 5: excellent). Both groups of radiologists were asked to evaluate the representative pulmonary findings of COVID-19 including ground-glass opacity (GGO), consolidation, mix of GGO and consolidation, the number of lobes involved, crazy paving pattern, air-bronchogram, pseudocavity, linear opacities and total lung severity score. Wilcoxon rank sum test was performed to evaluate the difference between the image quality of two image modalities. Intraclass coefficients (ICC) were utilized for quantifying the intermethod agreement for assessing the representative image findings. The intermethod agreement is determined as excellent when ICC ranges from 0.8 to 1.0, substantial when ICC ranges from 0.6 to 0.8, moderate when ICC ranges from 0.4 to 0.6, fair when ICC ranges from 0.2 to 0.4 and poor when ICC ranges from 0.0 to 0.2. Two-sided p values of less than 0.05 indicated there was a significant difference. SPSS 26.0 (SPSS, Chicago, IL) was utilized for completing all the statistical analysis.Results
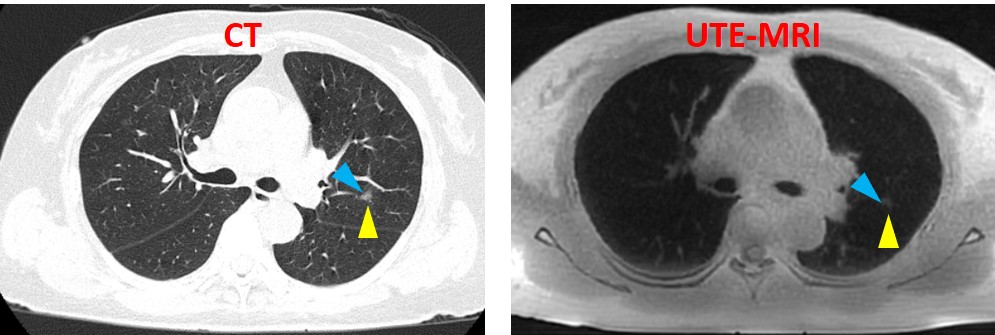
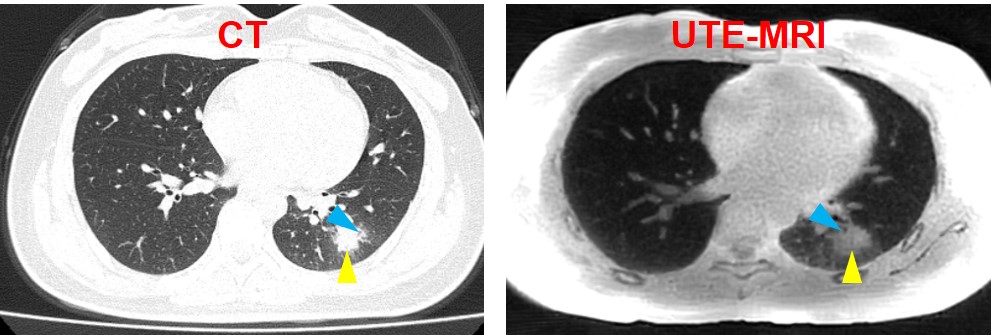
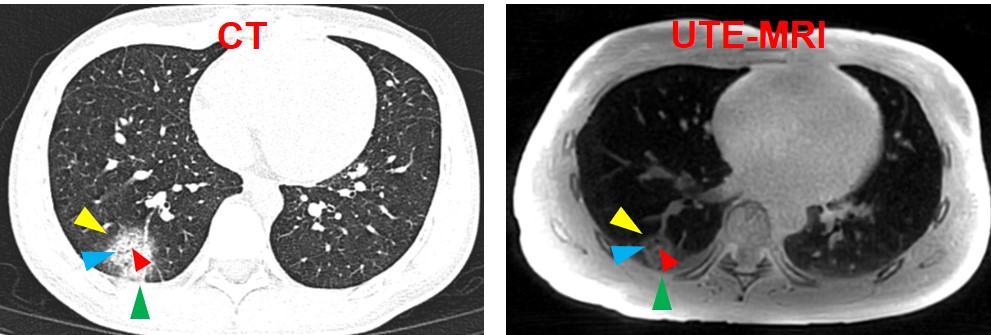
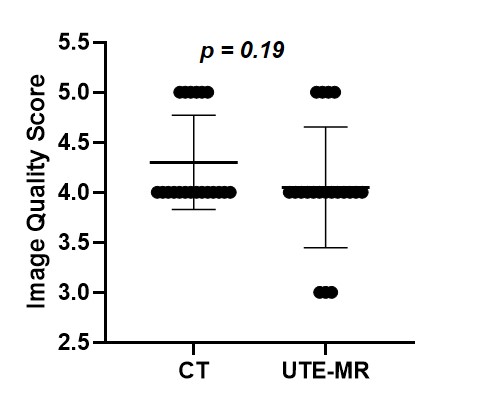
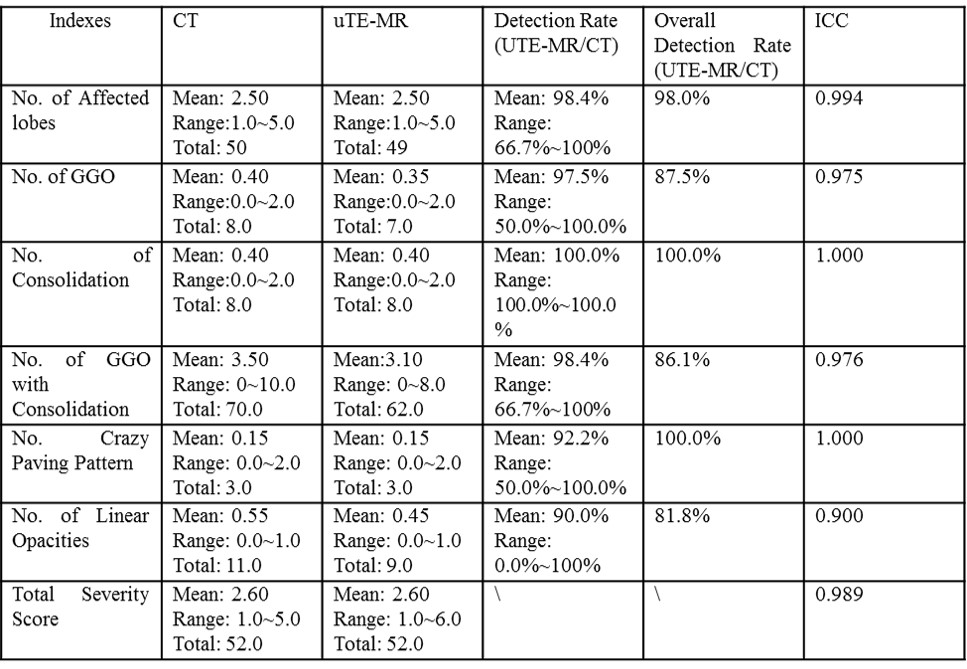
The representative image findings of COVID-19 on CT and UTE-MR were shown in Fig 1-3. As Fig. 4 demonstrated, the average image quality score of CT and UTE-MR were 4.3 (median: 4.0, mix: 4.0, max: 5.0) and 4.0 (median: 3.0, mix: 4.0, max: 5.0) (Mann-Whitney U: 159.0, p: 0.1894), which indicated both the image quality of CT and UTE-MR were determined between good to excellent without significant difference. In addition, Fig. 5 showed the intermethod agreement of UTE-MR and CT for detecting the representative image sings of COVID-19. Overall detection rate of UTE-MR for the number of affected lobes, the number of GGO, the number of consolidation, the number of GGO with consolidation, the number of crazy paving pattern and the number of linear opacities were respectively 98.0%, 87.5%, 100.0%, 86.1%, 100.0% and 81.8%. The ICCs of two image modalities for quantifying the number of Affected lobes, the number of GGO, the number of consolidation, the number of GGO with consolidation, the number of crazy paving pattern and the number of linear opacities were 0.994, 0.975, 1.000, 0.976, 1.000 and 0.900 (p < 0.001).Discussion
Our results showed that there was no significant difference between the image quality of CT and UTE-MR for evaluating the pulmonary findings of COVID-19, which suggested UTE-MR was capable of providing image quality similar to CT for visualizing the pulmonary structural variations of COVID-19. Moreover, the comparative analysis of UTE-MRI and CT for evaluating the representative radiological findings of COVID-19 showed that intermethod agreement were significant and were all determined between substantial and perfect. Nearly all the pulmonary abnormalities diagnosed by CT could be detected with UTE-MR. Given the substantial or excellent intermethod agreement, similar image quality as well as radiation-free character, this study, therefore, suggested that UTE-MR would be valuable for aiding the prevention and control of COVID-19. Above results were in accordance with several previous studies.5 Compared to the conventional MR imaging techniques, the excellent performance of UTE-MRI for pulmonary applications were due to the following aspects: 1) the non-Cartesian sampling together with the iterative reconstruction technique were applied to greatly accelerate the K-space filling, which results in a much shorter TE. As a result, the low signal-to-noise ratio caused by T2* effect was greatly improved. 2) Respiratory-gated UTE-MR is effective for reducing the image artifacts caused by respiratory motions.6Conclusion
UTE-MRI will be expected to emerge as a valuable tool for evaluating the COVID-19.Acknowledgements
NoneReferences
1. Rothan HA, Byrareddy SN. The epidemiology and pathogenesis of coronavirus disease (COVID-19) outbreak. J Autoimmun 2020:102433.
2. Leuraud K, Richardson DB, Cardis E, et al. Ionising radiation and risk of death from leukaemia and lymphoma in radiation-monitored workers (INWORKS): an international cohort study. The Lancet Haematology 2015;2(7):e276-e281.
3. Chassagnon G, Martin C, Hassen WB, et al. High-resolution lung MRI with Ultrashort-TE: 1.5 or 3 Tesla? Magn Reson Imaging 2019;61:97-103.
4. Torres L, Kammerman J, Hahn AD, et al. Structure-function imaging of lung disease using ultrashort echo time MRI. Acad Radiol 2019;26(3):431-441.
5. Ohno Y, Koyama H, Yoshikawa T, et al. Pulmonary high‐resolution ultrashort TE MR imaging: Comparison with thin‐section standard‐and low‐dose computed tomography for the assessment of pulmonary parenchyma diseases. Journal of Magnetic Resonance Imaging 2016;43(2):512-532.
6. Qian Y, Williams AA, Chu CR, Boada FE. High‐resolution ultrashort echo time (UTE) imaging on human knee with AWSOS sequence at 3.0 T. Journal of Magnetic Resonance Imaging 2012;35(1):204-210.
Figures