0159
The effect of scan length on reliability of resting-state fMRI in patients with drug-resistant epilepsy (DRE) in awake and under anesthesia1Department of Neurosurgery, Thomas Jefferson University, Philadelphia, PA, United States, 2Department of Bioengineering, Temple University, Philadelphia, PA, United States, 3Department of Anesthesiology, Thomas Jefferson University, Philadelphia, PA, United States, 4Department of Radiology, Thomas Jefferson University, Philadelphia, PA, United States
Synopsis
Resting-state fMRI suffers from poor test-retest reliability because of between-subject and within-subject variability. Scan duration is one the main factors affects the reliability of rs-fMRI studies. We showed that under anesthesia, the time needed to optimize ICC of rs-fMRI metrics including ALFF, fALFF, functional connectivity, and ReHo is lower compare with awake state. The optimum scan duration that satisfies good reliability is 14-20 min and 8-17 min in awake and under anesthesia, respectively. Also, variability of ICCs is lower under anesthesia than in awake.
Introduction
There has been a dramatic increase in the number of studies using resting-state fMRI in recent years. However, significant variability results from artifacts induced by motion, patient physiology, and differences in the task being performed by the subject that affect the reliability of estimation of brain functional connectivity. Hence, despite its potential, rs-fMRI has limited clinical utility. As such, comparisons across patients to evaluate neurological diseases as well as the ability to longitudinally follow disease progression in a single patient has been limited.1 Since induction and maintenance of general anesthesia generates a consistent brain state, virtually eliminates head motion, and increases our ability to control certain aspects of patient physiology, BOLD imaging and resultant resting-fMRI under these conditions is expected to be more consistent between subjects and within subjects with repeat testing.2,3 Scan duration is also an important factor that affects the reliability of resting-state functional connectivity. Since, it could have different effect on reliability of rs-fMRI studies in patients under general anesthesia and awake state. In this study, we evaluate the influence of scan length on test-retest reliability of rs-fMRI metrics in both conditions of awake and under volatile general anesthesia (vGA).4-8Methods
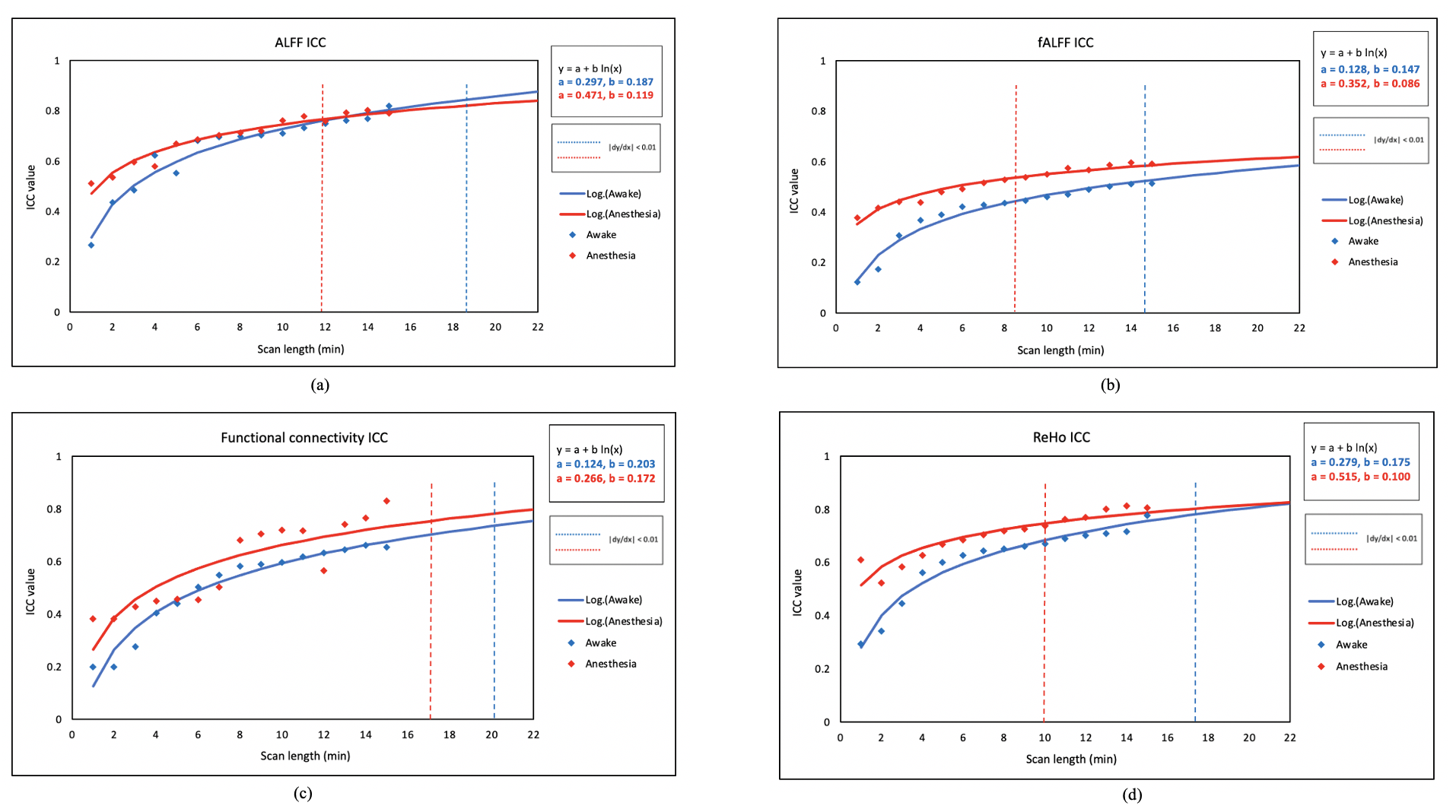
A total of 9 patients with DRE of requiring interstitial thermal therapy (LITT) were scanned in two states. The first scan was performed in an awake state before surgery. The second scan was performed two weeks later under vGA necessary for LITT surgery. At each state, two rs-fMRI sessions were obtained with a 15-minute gap between each. Each resting state scan was 15 minutes in length. We used propofol as the induction agent and sevoflurane as the maintenance anesthetic for vGA. In order to assess the effect of scan duration on the functional connectivity metrics, resting state data for each subject was truncated into 15 bins with ith bin containing the first i minutes of data acquisition. Then, voxel-wise rs-fMRI metrics including fractional and absolute amplitude of low frequency fluctuations (fALFF and ALFF respectively), functional connectivity (FC), and regional homogeneity (ReHo) was measured using DPARSF_V5.0 after preprocessing steps. Intraclass correlation coefficient (ICC) was calculated to estimate the reliability between two sessions of scanning for both states. Standardized non-linear logarithmic curves (y = a + b ln(x)) were fitted to the ICCs. The scan duration needed to optimize ICC was defined as the point where the derivative of logarithmic function (|dy/dx|) < 0.01.Results
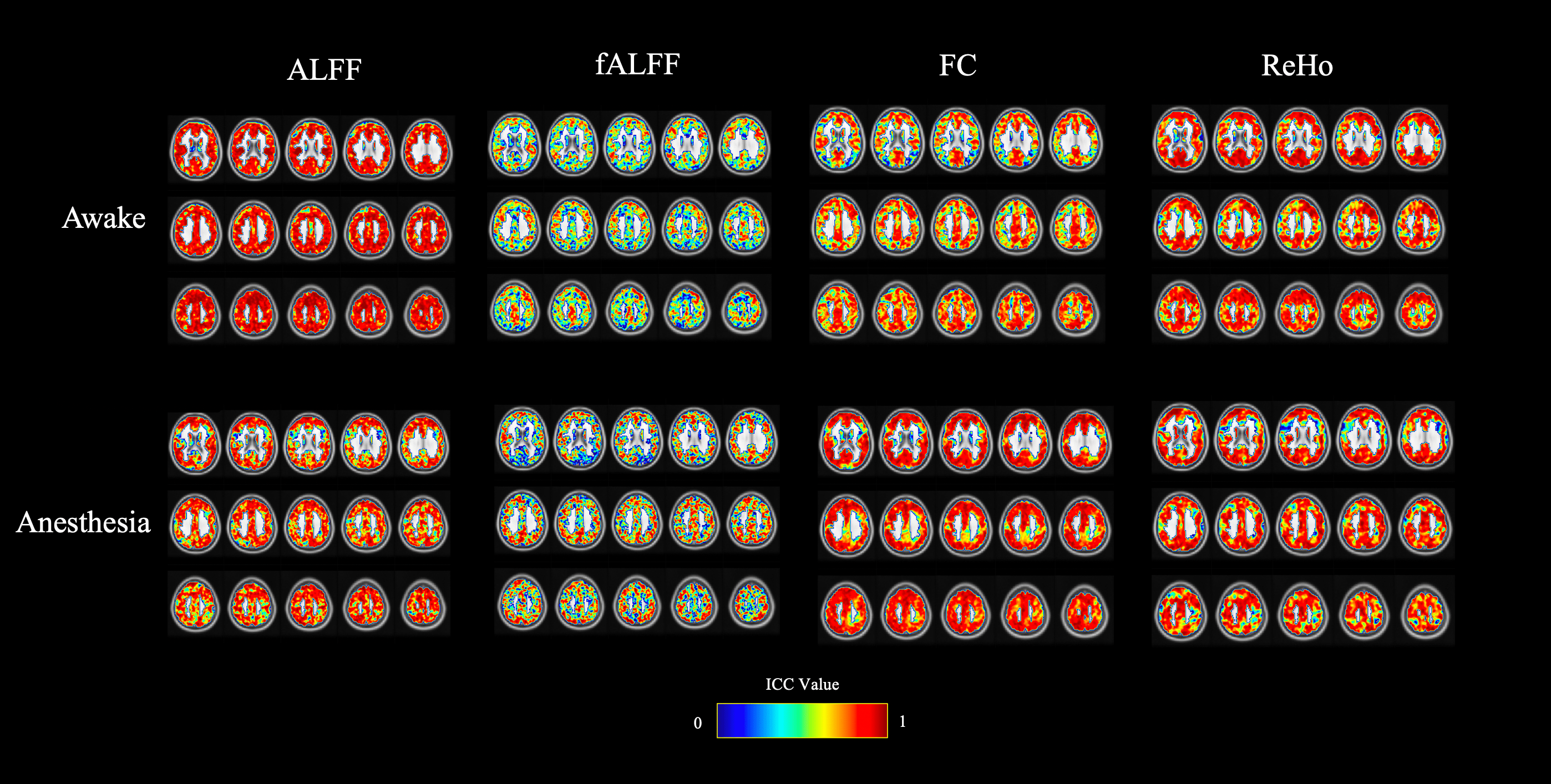
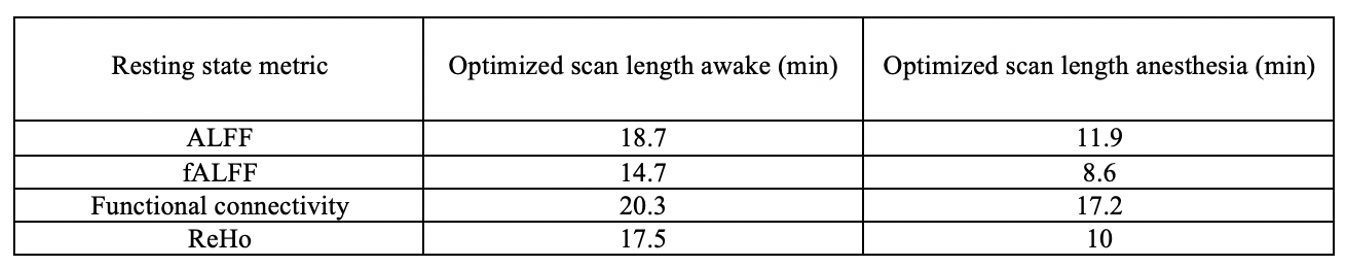
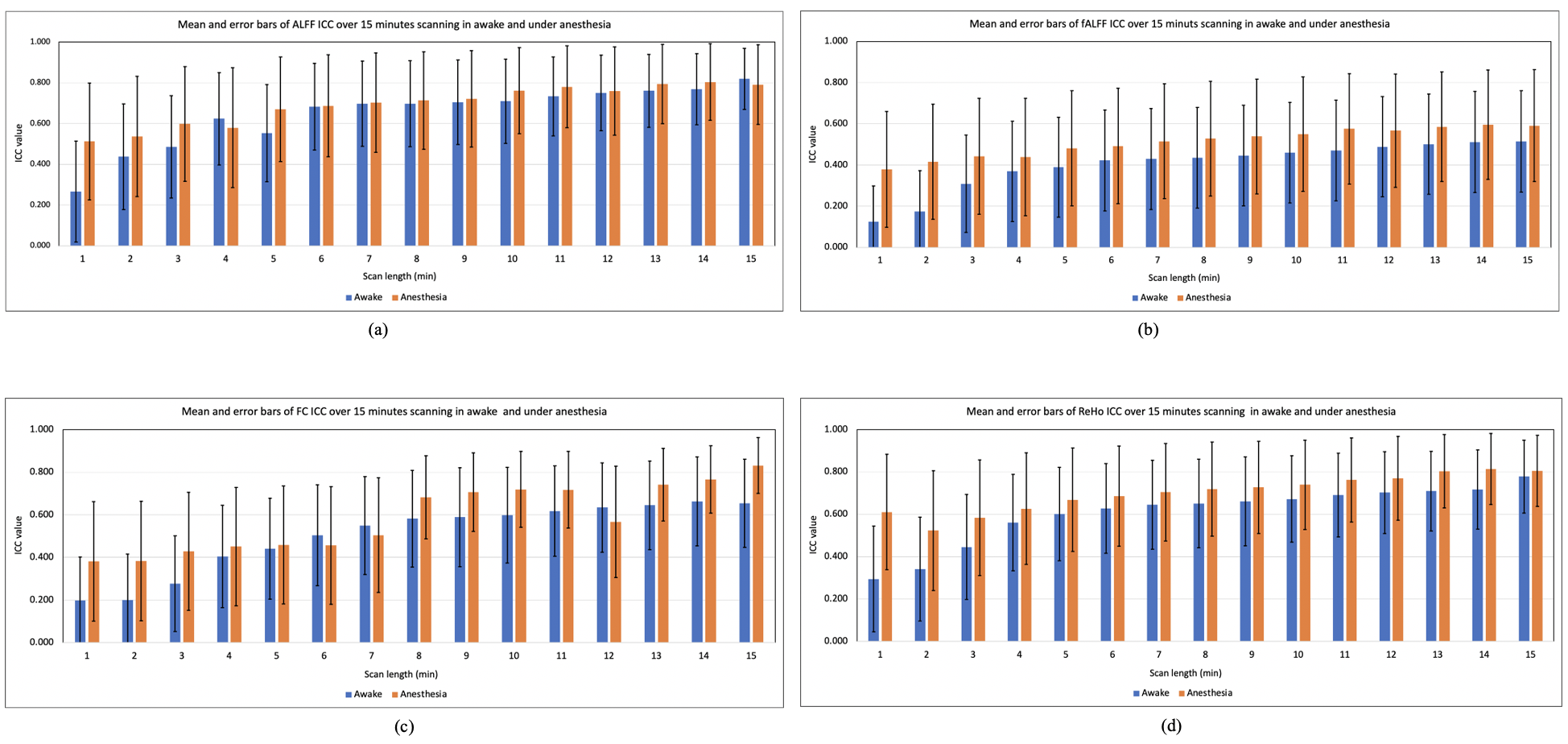
ICC calculated for each metrics showed improvement of test-retest reliability under vGA than in awake in all quantitative metrics as shown in Fig. 1. We found that the optimized scan lengths for the rs-fMRI metrics are shorter under vGA (8.6 to 17.2 min) compared with in the awake state (14.7 to 20.3 min) (Fig. 2 and Fig. 3). The variability of ICC also decreases as the function of scan length (Fig. 4). Among aforementioned quantitative maps, fALFF reaches to optimum value in the shortest scan duration (8.6 min under anesthesia and 14.7 min in awake).Discussion
To the best of our knowledge this was the first study on evaluating the effect of rs-fMRI scan duration on patients with DRE. This study provides the comprehensive evaluation of voxel-wise test-retest reliability of rs-fMRI metrics and its relationship with scan length in two states of awake and under vGA. Considering the effect of scan duration on test-retest reliability in rs-fMRI studies is crucial but must be balanced with a potential increase in motion artifact with longer scan times.1,4,9 In this study, we investigated the reliability of rs-fMRI in patients with DRE under general anesthesia. The results show that there is improvement of reliability with vGA for all metrics and scan durations less than 12 minutes. The scan duration needed to optimize ICC for all metrics was always lower for scanning in the vGA state.Conclusion
Our results help to understand the implication of anesthetic agents in reliability of rs-fMRI studies. In turn, these findings may help to increase the utility of rs-fMRI for longitudinal research and in clinical applications in patients with neurological diseases. These results are very encouraging and warrant further investigation with higher sample size.Acknowledgements
No acknowledgement found.References
1- Birn RM. The role of physiological noise in resting-state functional connectivity. Neuroimage. 2012 Aug 15;62(2):864-70.
2- Paasonen J, Stenroos P, Salo RA, Kiviniemi V, Gröhn O. Functional connectivity under six anesthesia protocols and the awake condition in rat brain. Neuroimage. 2018 May 15;172:9-20.
3- Venkatraghavan L, Bharadwaj S, Wourms V, Tan A, Jurkiewicz MT, Mikulis DJ, Crawley AP. Brain resting-state functional connectivity is preserved under sevoflurane anesthesia in patients with pervasive developmental disorders: a pilot study. Brain connectivity. 2017 May 1;7(4):250-7.
4- Birn RM, Molloy EK, Patriat R, Parker T, Meier TB, Kirk GR, Nair VA, Meyerand ME, Prabhakaran V. The effect of scan length on the reliability of resting-state fMRI connectivity estimates. Neuroimage. 2013 Dec 1;83:550-8.
5- Chou Y, Panych LP, Dickey CC, Petrella JR, Chen N. Investigation of long-term reproducibility of intrinsic connectivity network mapping: a resting-state fMRI study. AJNR Am J Neuroradiol. NIH Public Access; 2012;33:833–838.
6- Liao XH, Xia MR, Xu T, Dai ZJ, Cao XY, Niu HJ, Zuo XN, Zang YF, He Y. Functional brain hubs and their test–retest reliability: a multiband resting-state functional MRI study. Neuroimage. 2013 Dec 1;83:969-82.
7- Chou Y, Panych LP, Dickey CC, Petrella JR, Chen N. Investigation of long-term reproducibility of intrinsic connectivity network mapping: a resting-state fMRI study. AJNR Am J Neuroradiol. NIH Public Access; 2012;33:833–838.
8- Palanca BJA, Mitra A, Larson-Prior L, Snyder AZ, Avidan MS, Raichle ME. Resting-state Functional Magnetic Resonance Imaging Correlates of Sevoflurane-induced Unconsciousness. Anesthesiology. 2015;123:346–356.
9- Maknojia S, Churchill NW, Schweizer TA, Graham SJ. Resting state fMRI: Going through the motions. Frontiers in neuroscience. 2019;13:825.
Figures