0056
Evaluating pCR after neoadjuvant systemic treatment of invasive breast cancer using DWI in comparison to DCE-based kinetic analysis1Department of Diagnostic Imaging and Nuclear Medicine, Kyoto University graduate school of medicine, Kyoto, Japan, 2Kyoto Medical Center, Kyoto, Japan, 3Department of Pathology, Kyoto University Hospital, Kyoto, Japan, 4Department of Breast Surgery, Kyoto University Hospital, Kyoto, Japan
Synopsis
This study aimed to examine the performance of DWI in diagnosing pCR before surgery. Kinetic analysis from standard DCE-MRI were analyzed for comparison. ROC analysis for diagnosing pCR based on DWI score/Kinetic score by two readers was performed. Kinetic score showed slightly higher AUC while 95% confidence interval overlapped with that of DWI score. Both kinetic score and DWI score demonstrated excellent diagnostic performance among triple negative subtype compared to other subtypes.
Introduction:
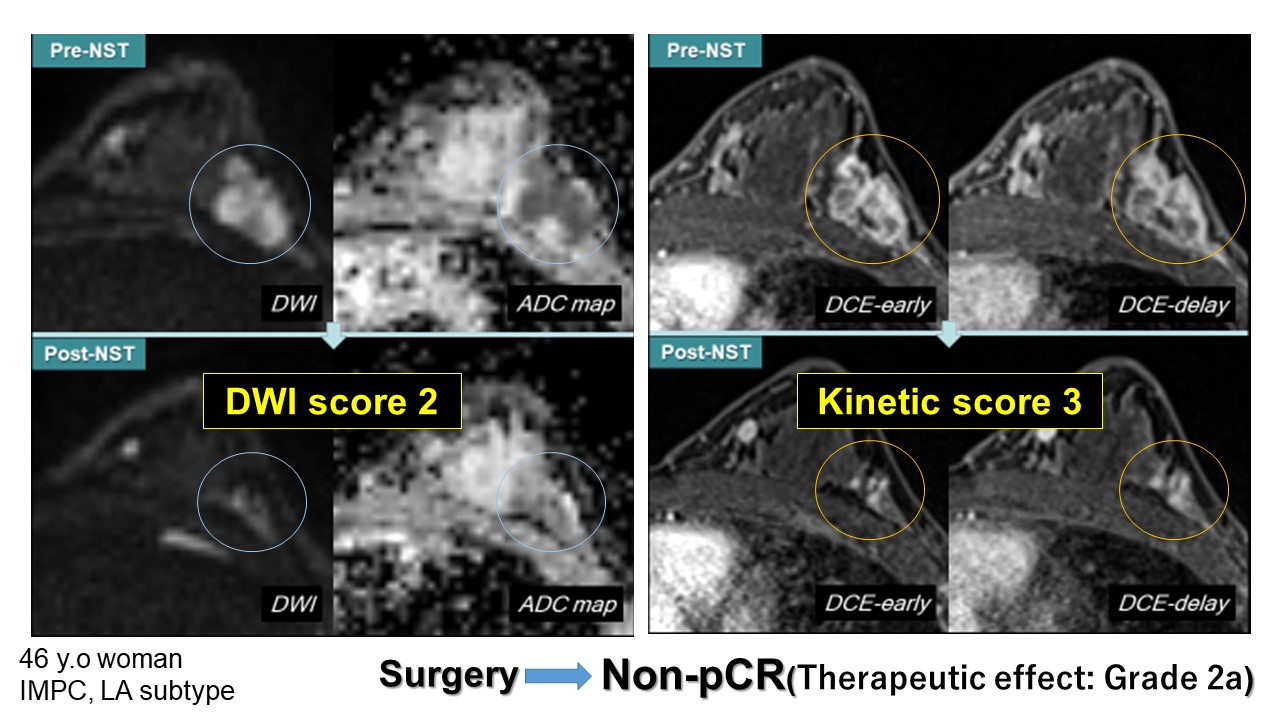
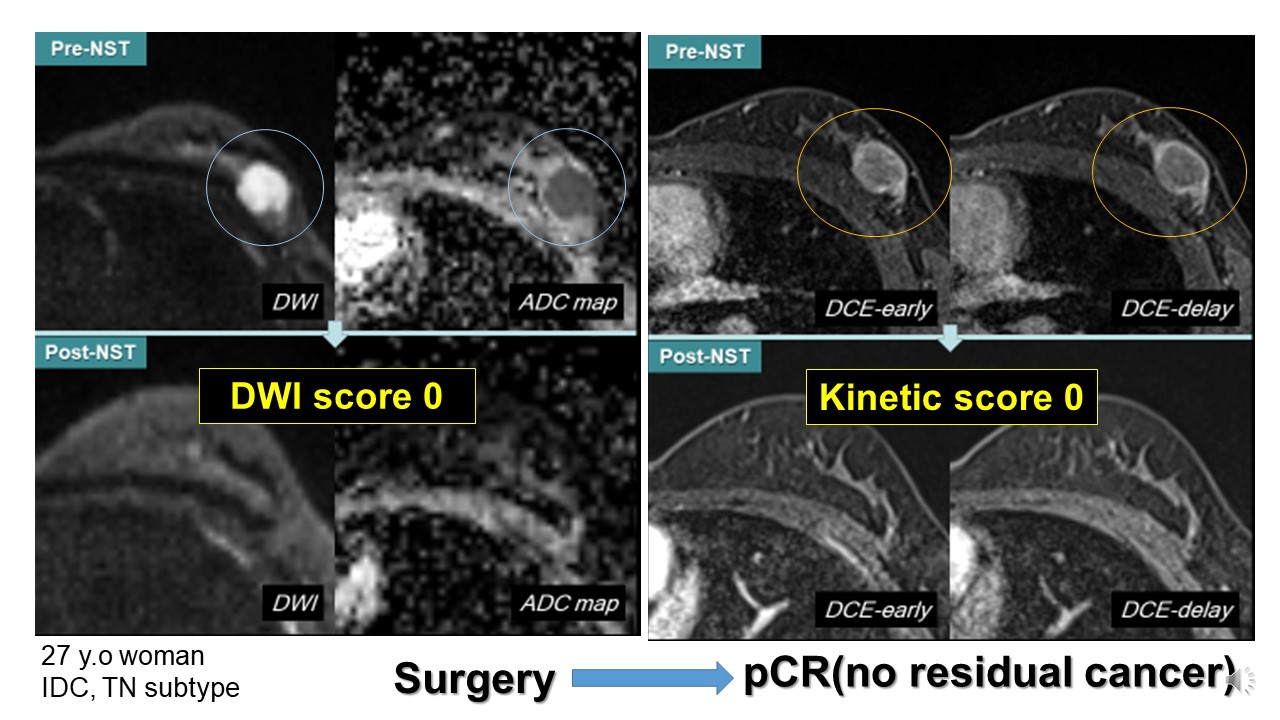
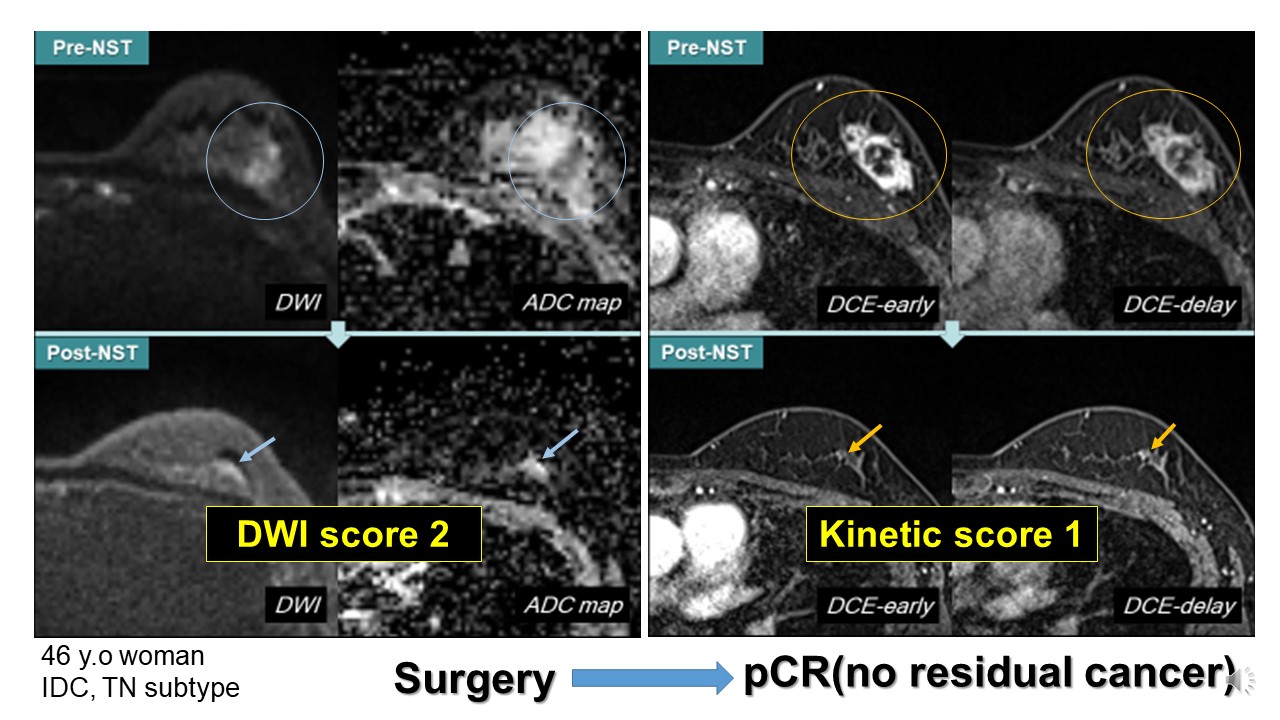
For locally-advanced breast cancer, preoperative neoadjuvant systemic treatment (NST) is recommended. When the cancer shrinks and even disappears (pathological complete response: pCR) after NST, surgery may be minimized with favorable outcome. Breast MRI is used in evaluating residual cancer. However, accurate diagnosis of pCR is difficult due to various enhancement pattern after treatment. Fibrosis or inflammation may be enhanced, mimicking residual tumor. Incorporating kinetic analysis may help in identifying viable tumor1,2, while diffusion-weighted images (DWI) can be used to evaluate residual tumor. This study aimed to examine the performance of DWI in diagnosing pCR before surgery. Kinetic analysis from standard DCE-MRI were analyzed for comparison.Materials & Methods:
In total 116 lesions from 114 patients who underwent pre-surgical MRI evaluation after NST were included. Breast MRI was performed with a 3T scanner (Prisma /Trio : Siemens AG, Erlangen, Germany). MR images were obtained using routine protocols sequence: T1WI, T2WI, DWI (axial single-shot EPI; TR/TE, 6300-7000/50-62ms; pixel size 2x2x3 mm; NEX, 3; b=0, 1000sec/mm2), Dynamic MRI (pre, 1-2, 5-6 min post-contrast; axial VIBE with fat suppression; TR/TE, 3.8/1.4ms; 0.9x 0.9x1 mm). DWI of the target lesion was scored as 3-point scale (2: obvious high signal intensity, 1: small focus of high – intermediate signal intensity, 0: no abnormal signal). Kinetic patterns of the lesions on DCE-MRI were scored as 3: washout, 2: plateau, 1: persistent, and 0: no enhancement.Results:
Pathological diagnosis of the 116 lesions were as follows; invasive ductal carcinoma (n=103), invasive lobular carcinoma (n=2), invasive micro papillary carcinoma (n=5), mucinous carcinoma (n=3), metaplastic carcinoma (n=2) invasive apocrine carcinoma (n=1). out of 116 (42.2%) lesions achieved pCR while 67 out of 116 (57.8%)lesions were categorized as non-pCR.DWI score: The number of patients scored as DWI 2, 1, 0 were 59, 23 and 34 for reader 1, 52, 32 and 32 for reader 2. DWI score of the two readers agreed on 106 lesions (88.3%) with kappa value of 0.85 (95% Confidence Interval (CI): 0.78-0.93), suggesting excellent agreement. DWI score was associated with residual disease in both reader 1 and 2. ROC analysis showed area under the ROC curve (AUC) of 0.84 (95% CI: 0.75-0.90) for reader 1. A cut-off value of score 1 or above resulted in sensitivity /specificity of 75.7% and 84.0%. For reader 2, ROC analysis showed AUC of 0.84 (95% CI: 0.76 - 0.90).
Kinetic score: The number of patients scored as kinetic score 3, 2, 1, 0 were 45, 18, 33 and 20, for reader 1, 42, 12, 38 and 24 for reader 2 respectively. Kinetic score of the two readers agreed on 93 lesions (80.2%) with kappa value of 0.81 (95%CI: 0.73-0.89), suggesting excellent agreement. Kinetic score was associated with residual disease in both reader 1 and 2. ROC analysis showed AUC of 0.87 (95% CI: 0.80 -0.93) and 0.85 (0.76 - 0.91) for reader 2 respectively.
Subtype analysis: In general, kinetic score showed slightly higher AUC while 95% confidence interval overlapped with that of DWI score. Both kinetic score and DWI score demonstrated excellent diagnostic performance among triple negative subtype compared to other subtype with AUC of 0.88-0.95. For luminal subtype, DWI score tended to perform better than kinetic score.
Discussion:
Our results suggest that DWI-based analysis showed diagnostic performance similar to kinetic analysis. Kinetic analysis looked at the vascularity as a marker of viable residual tumor, while DWI-based images are associated with cellular component of the residual tumor. Both kinetic and DWI score performed better in predicting pCR for triple-negative subtype with AUC of nearly 90%. Although the DWI showed slightly lower AUC, DWI has the advantage of non-contrast images and may be better in predicting residual tumor among luminal subtype The above results indicate the need of different strategy based on subtype when evaluating residual tumors after NST.Conclusions:
DWI score can be used to evaluate pCR with diagnostic performance similar to that in kinetic score. in triple negative subtypes.Acknowledgements
No acknowledgement found.References
- Shin, H. J., et al. (2016). "Tumor apparent diffusion coefficient as an imaging biomarker to predict tumor aggressiveness in patients with estrogen-receptor-positive breast cancer." NMR Biomed 29(8): 1070-1078.
- Kim, S. Y., et al. (2018). "Dynamic Contrast-enhanced Breast MRI for Evaluating Residual Tumor Size after Neoadjuvant Chemotherapy." Radiology 289(2): 327-334.
- Marinovich, M.L., et al., Meta-analysis of magnetic resonance imaging in detecting residual breast cancer after neoadjuvant therapy. J Natl Cancer Inst, 2013. 105(5): p. 321-33.
- Liu, S., et al., Diffusion-weighted imaging in assessing pathological response of tumor in breast cancer subtype to neoadjuvant chemotherapy. J Magn Reson Imaging, 2015. 42(3): p. 779-87
- Gao, W., et al. (2018). "Diffusion-weighted imaging in monitoring the pathological response to neoadjuvant chemotherapy in patients with breast cancer: a meta-analysis." World J Surg Oncol 16(1): 145.
- Partridge, S. C. and E. S. McDonald (2013). "Diffusion weighted magnetic resonance imaging of the breast: protocol optimization, interpretation, and clinical applications." Magn Reson Imaging Clin N Am 21(3): 601-624.
- Khokher, S., et al. (2012). "Comparison of WHO and RECIST criteria for evaluation of clinical response to chemotherapy in patients with advanced breast cancer." Asian Pac J Cancer Prev 13(7): 3213-3218.
Figures
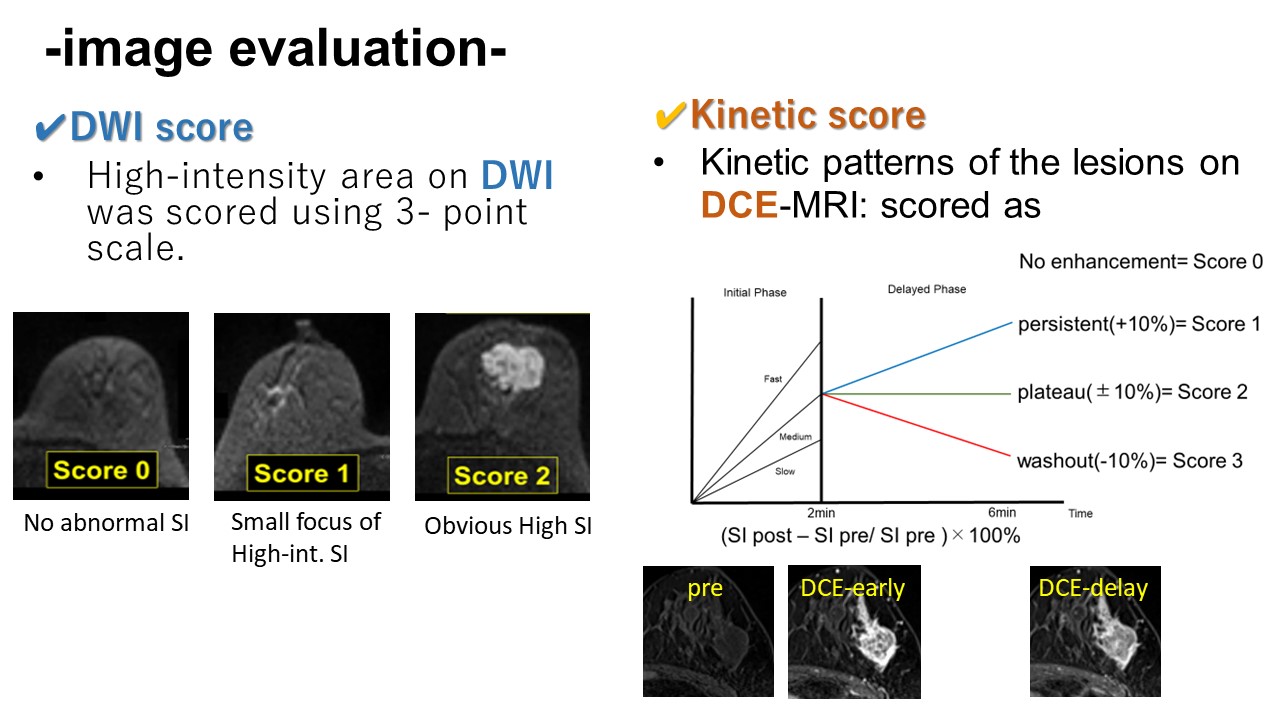
-Image evaluation-
- DWI score
DWI of the target lesion was evaluated and categorized as 3-point scale.
0: no abnormal signal, 1: small focus of high - intermediate signal intensity, 2: obvious high signal intensity.
- Kinetic score
Kinetic patterns of the lesions on DCE-MRI was scored as
0 : no enhancement, 1 : persistent, 2 : plateau and 3 : washout.
For both scores Low score indicates pCR.
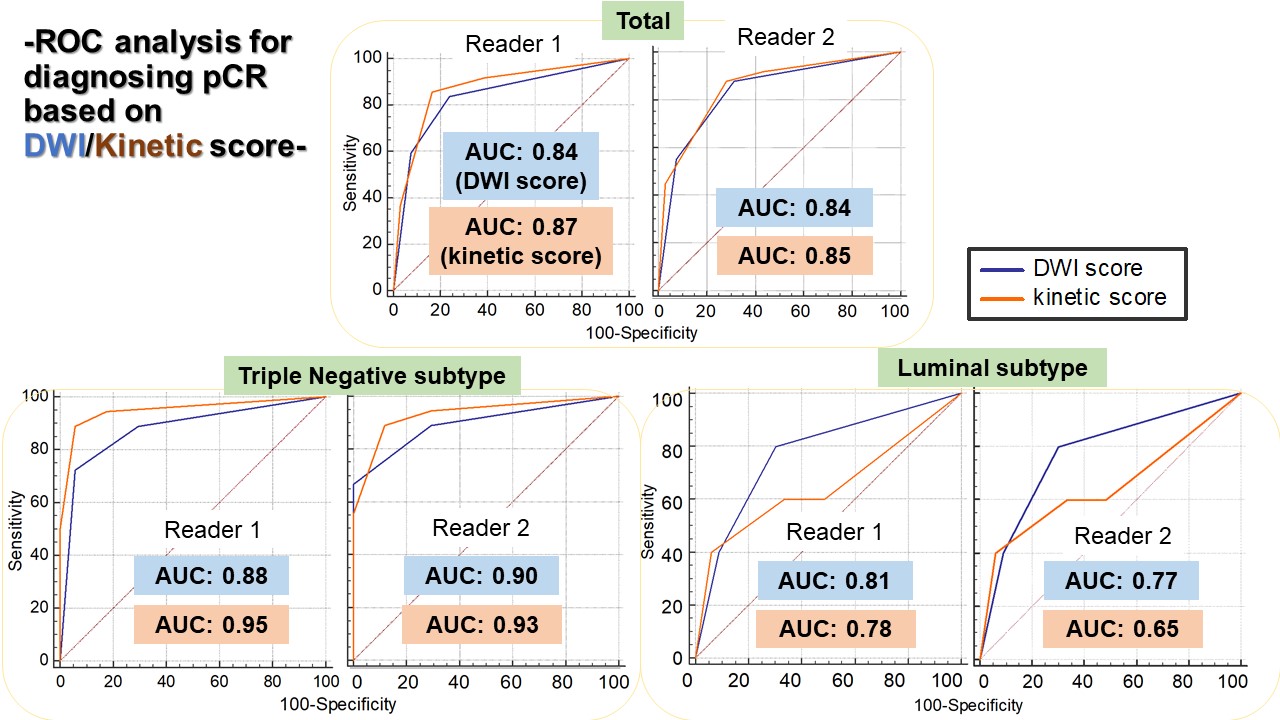
-ROC analysis for diagnosing pCR based on DWI score/Kinetic score-
Kinetic score showed slightly higher AUC while 95% confidence interval overlapped with that of DWI score. Both kinetic score and DWI score demonstrated excellent diagnostic performance among triple negative subtype compared to other subtype with AUC of 0.88-0.95. For luminal subtype, DWI score tended to perform better than kinetic score.