0050
Whole heart SMS-bSSFP perfusion imaging with high resolution at 1.5T1King's College London, London, United Kingdom, 2IRCCS San Camillo Hospital, Venice, Italy, 3Siemens Healthcare Limited, Frimley, United Kingdom, 4Siemens Healthcare GmbH, Erlangen, Germany, 5Siemens Healthcare Ltd, Melbourne, Australia
Synopsis
First-pass cardiac magnetic resonance (CMR) perfusion imaging is widely used for non-invasive assessment of coronary artery disease (CAD). Conventional CMR perfusion sequences are limited in spatial coverage and resolution. We have developed a SMS-bSSFP sequence with a total acceleration factor of 16 (multiband (MB) acceleration of 3 x in-plane acceleration of 5.5) and compressed sensing reconstruction to enable 1.5 T CMR perfusion with whole-heart coverage and high (1.4 x 1.4 mm2) in-plane spatial resolution. The results from a preliminary study in 6 patients comparing the proposed acquisition against a conventional 3-slice acquisition are presented.
Introduction
First-pass cardiac magnetic resonance (CMR) perfusion imaging is widely used for non-invasive assessment of coronary artery disease (CAD). However, conventional CMR perfusion sequences at 1.5T are limited in spatial coverage and resolution, limiting the assessment of subendocardial perfusion defects and transmural perfusion gradients and precluding assessment of total myocardial ischemic burden. We have previously demonstrated that simultaneous multi-slice (SMS) bSSFP with a multiband factor of 2 and in-plane acceleration of 5.5 can be combined with compressed sensing reconstruction to acquire a 6-slice CMR perfusion sequence at 1.5T with high spatial resolution1. However, a 6-slice acquisition is not sufficient for full left-ventricular coverage in most patients. SMS-bSSFP has recently been extended to a multiband (MB) factor of 32, enabling a further increase in spatial coverage. The aim of the current study is to use SMS-bSSFP with MB3 to achieve high resolution 1.5T SMS-bSSFP perfusion imaging with whole heart coverage.Methods
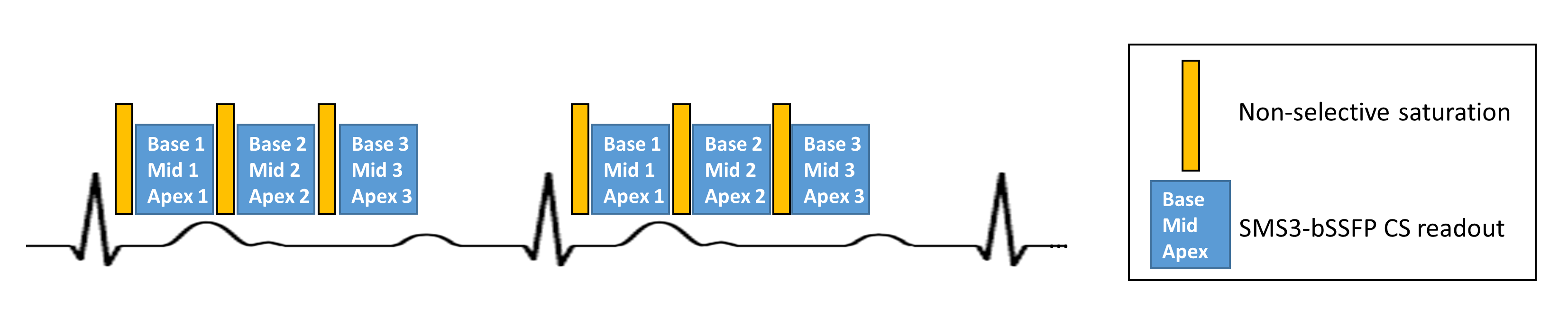
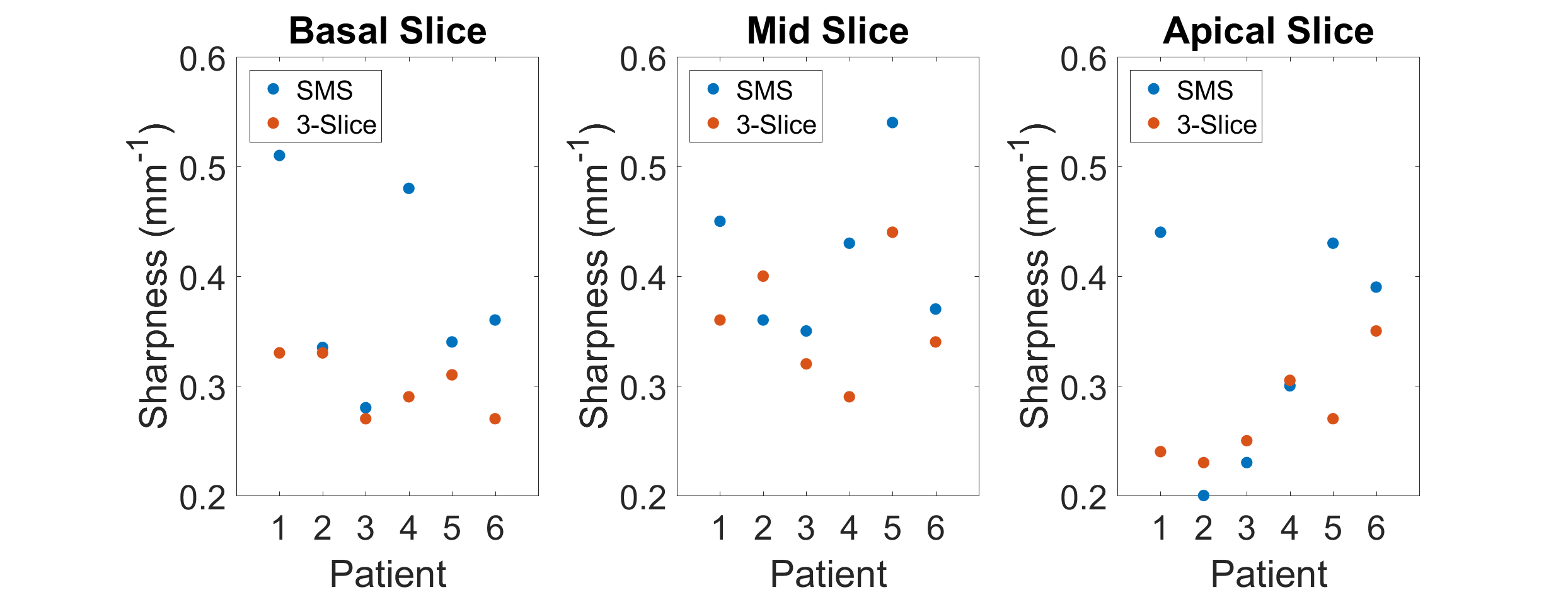
A prototype SMS-bSSFP sequence with CAIPIRINHA encoding3, GC-LOLA correction4 and pseudo-random undersampling was used (see Figure 1). The pseudorandom undersampling scheme for SMS-bSSFP MB3 is analogous to that proposed for MB21. To extend this algorithm to MB3, the fully sampled central region is maintained, and the under-sampled (peripheral) k-space lines are sorted into 3 bins which correspond to the 3 phase-cycling steps for each slice (slice 1: 0, 2π/3, 4π/3, slice 2: 0, 0, 0, slice 3: 0, 4π/3, 2π/3). An equal number of k-space lines are randomly selected from each bin and the selected lines are acquired sequentially from each bin to maintain the required SMS-bSSFP phase cycling and CAIPIRINHA phase ramp in k-space. Two first-pass rest perfusion acquisitions (proposed and conventional), separated by 10 minutes and with a contrast dose of 0.075 mmol/kg each, were acquired in a random order in 6 patients (2M, mean age 53±10) undergoing routine clinical CMR studies at 1.5T (MAGNETOM Aera, Siemens Healthcare, Erlangen, Germany). The patients were instructed to hold their breath during the first-pass of the contrast agent. To enable whole-heart coverage and high in-plane spatial resolution, the total acceleration of proposed SMS-bSSFP sequence is 16 (in-plane acceleration: 5.5, MB factor 3). The in-plane acceleration of the conventional 3-slice (single-band) sequence is 3. Other imaging parameters are matched as closely as possible: TR/TE/α: 2.97ms/1.26ms/40° (proposed), TR/TE/α: 2.73ms/1.37ms/40° (conventional), voxel size: 1.4x1.4x10mm3 (proposed), 1.9x1.9x10mm3 (conventional), typical FOV: 360x360mm2, TS 99ms (proposed) 94ms (conventional), total acquisition duration: 558ms (proposed), 567ms (conventional), bandwidth 1015Hz/Px. The conventional sequence was reconstructed using a standard GRAPPA reconstruction, while the proposed sequence was reconstructed using an inline SMS-compatible5 prototype compressed sensing reconstruction6. The sharpness was measured as previously described1,7 at the septal blood-myocardium interface on the dynamic frame corresponding to peak blood pool signal intensity. The measurement was performed on all slices acquired with the conventional sequence, and on the 3 SMS slices with matched cardiac phase and position to the conventional acquisition.Results
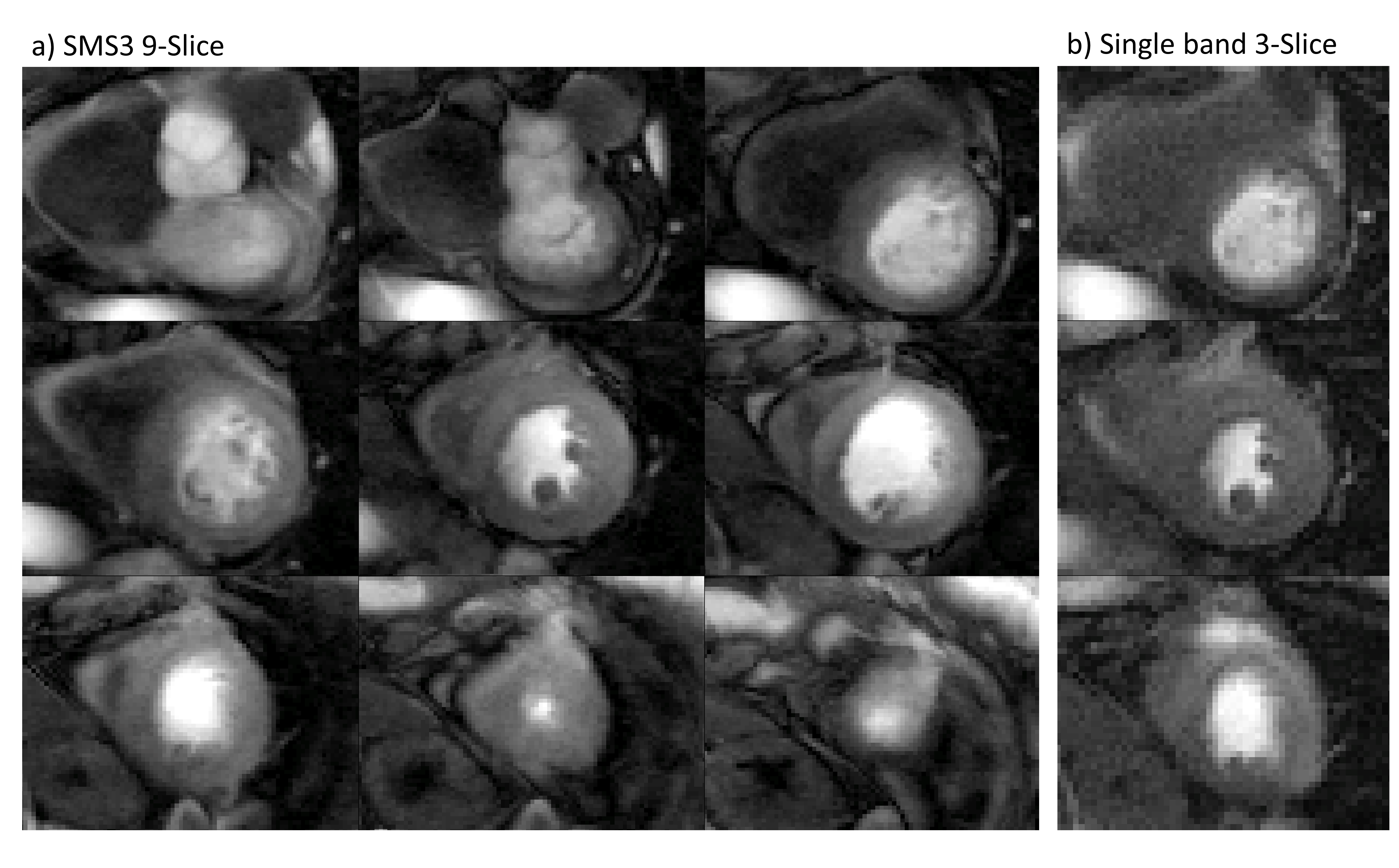
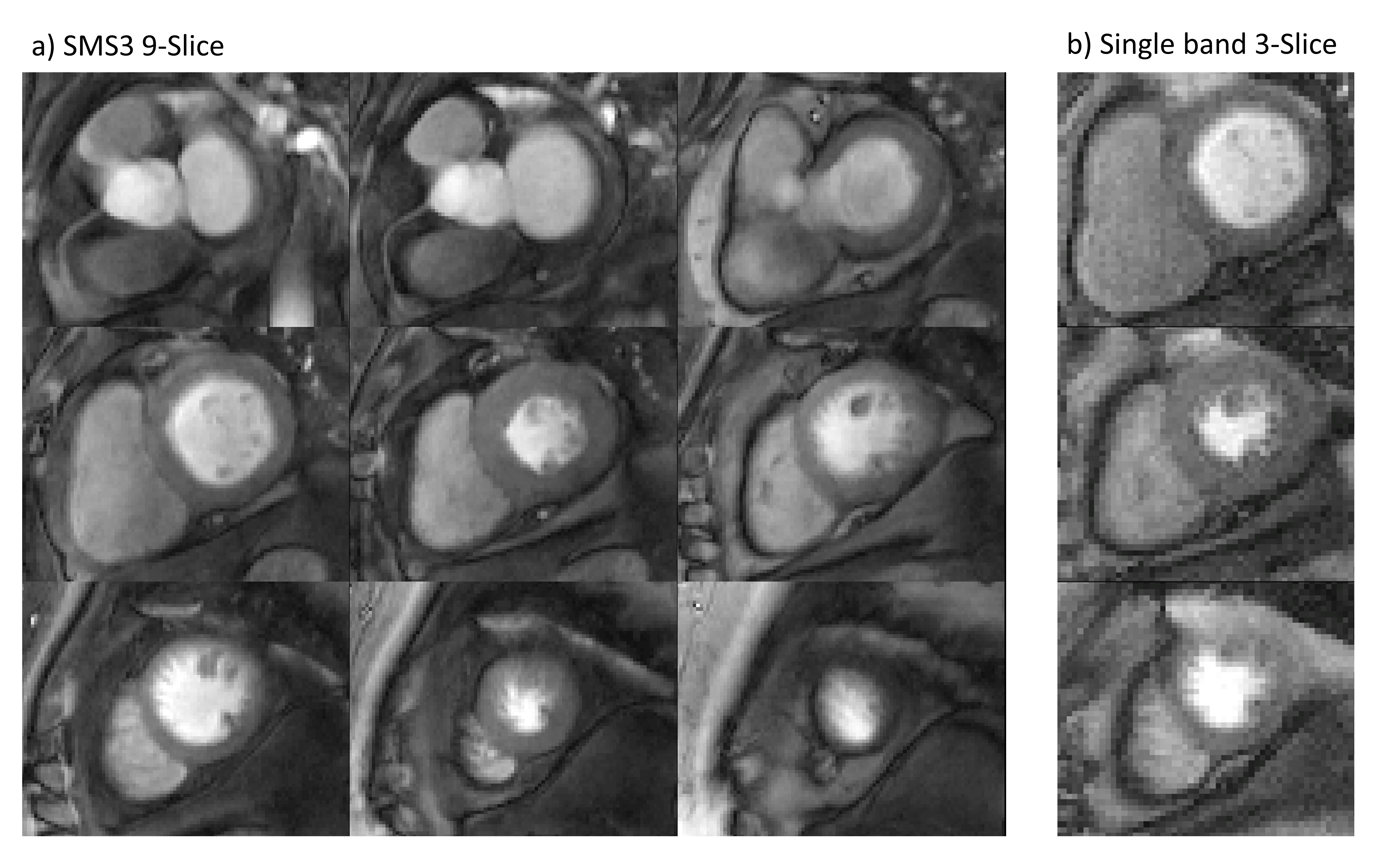
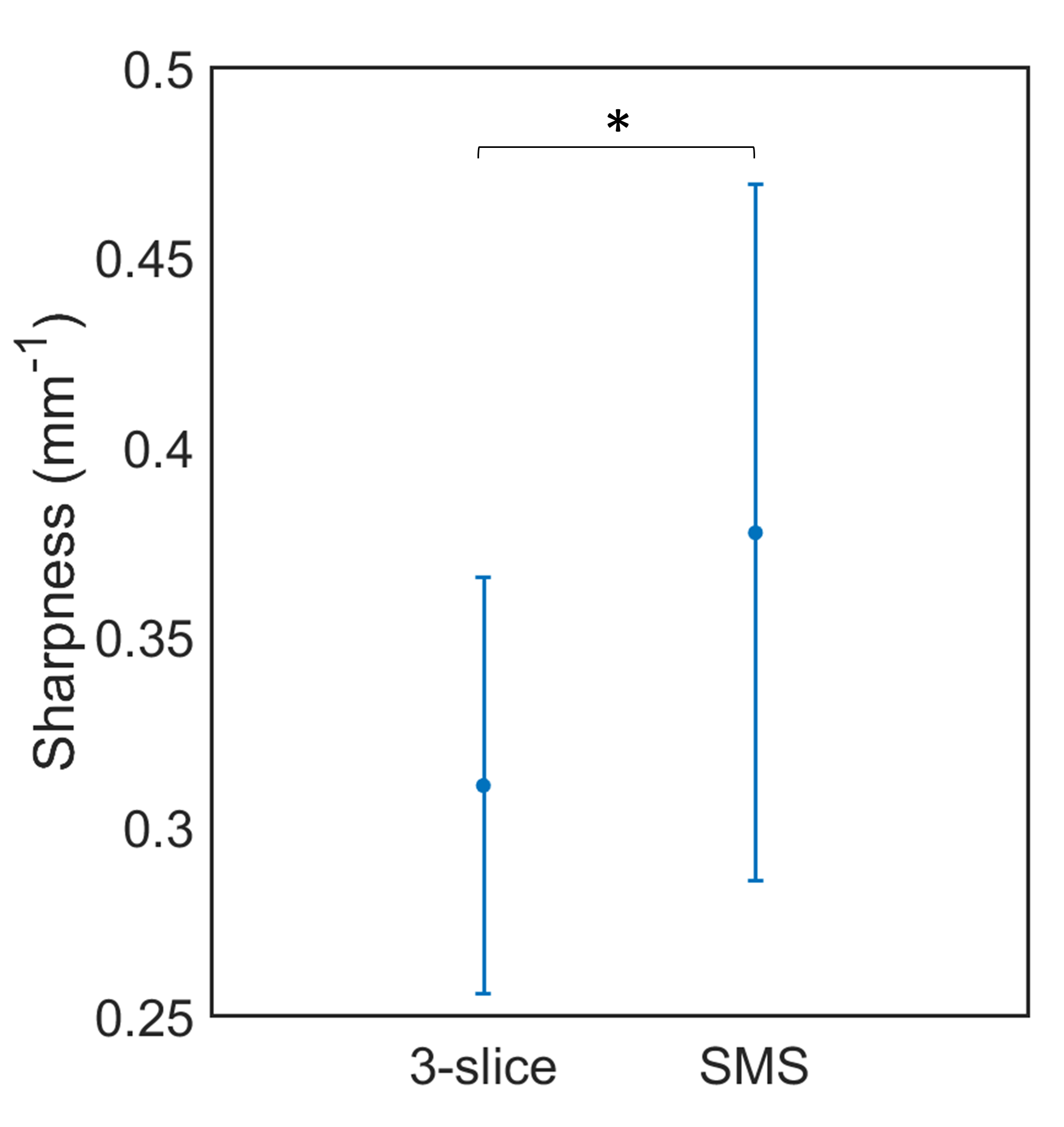
Whole heart coverage was achieved in all patients using the proposed SMS-bSSFP sequence. Figures 2-3 show examples of first-pass perfusion acquisitions in two patients with no suspected CAD, using the proposed SMS-bSSFP perfusion sequence with 9 slices and high in-plane spatial resolution (1.4x1.4mm2) and a conventional 3-slice sequence with in-plane resolution = 1.9 x 1.9 mm2. All images are shown at peak myocardial signal enhancement. Sharpness measurements across 3 slices and 6 patients were higher using the proposed 9-slice SMS sequence vs. a conventional 3-slice sequence (0.31 ± 0.06 mm-1 vs. 0.38 ± 0.09 mm-1, p = 0.002, Figure 5).Discussion
This study demonstrates that SMS-bSSFP with a MB factor of 3 can be used to acquire whole-heart CMR perfusion imaging at 1.5 T with high in-plane spatial resolution. The temporal regularisation employed in the iterative reconstruction results in blurring and artefacts outside of the first-pass (breath-hold) section of the acquisition. Development of a motion-compensated acquisition-reconstruction framework for SMS-bSSFP is warranted to ensure the image quality is not degraded in the case of a sub-optimal breath-hold or free-breathing acquisition. The current study was carried out at rest in patients without suspected CAD, therefore further validation of the sequence in patients with CAD and in stress conditions is required to evaluate the diagnostic value of this sequence.Conclusion
SMS-bSSFP with a total acceleration factor of 16 and compressed sensing reconstruction enables whole-heart CMR perfusion imaging at 1.5 T with high in-plane spatial resolution (1.4 x 1.4 mm2).Acknowledgements
This work was supported by the Engineering and Physical Sciences Research Council (EPSRC) grant (EP/R010935/1), the British Heart Foundation (BHF) (PG/19/11/34243), the Wellcome EPSRC Centre for Medical Engineering at King’s College London (WT 203148/Z/16/Z), the National Institute for Health Research (NIHR) Biomedical Research Centre based at Guy’s and St Thomas’ National Health Service (NHS) Foundation Trust and King’s College London, and Siemens Healthineers. The views expressed are those of the authors and not necessarily those of the NHS, the NIHR or the Department of Health.References
1 McElroy, S. et al. Combined simultaneous multislice bSSFP and compressed sensing for first‐pass myocardial perfusion at 1.5 T with high spatial resolution and coverage. Magn Reson Med. 84, 3103-3116, doi: 10.1002/mrm.28345 (2020).
2 Ferrazzi, G. et al. Dual-contrast and dual-phase first-pass myocardial perfusion using simultaneous multi-slice imaging. 23rd Annual Meeting of SCMR.
3 Stab, D. et al. CAIPIRINHA accelerated SSFP imaging. Magn Reson Med. 65, 157-164, doi:10.1002/mrm.22600 (2011).
4 Stab, D. & Speier, P. Gradient-controlled local Larmor adjustment (GC-LOLA) for simultaneous multislice bSSFP imaging with improved banding behavior. Magn Reson Med. 81, 129-139, doi:10.1002/mrm.27356 (2019).
5 Stab, D. et al. in 23rd Annual Meeting of ISMRM. 981.
6 Liu, J. et al. 2D bSSFP real-time cardiac CINE-MRI: compressed sensing featuring weighted redundant Haar Wavelet regularization in space and time. J Cardiovasc Magn Reson. 15, 1-2 (2013).
7 Larson, A. C. et al. Preliminary investigation of respiratory self-gating for free-breathing segmented cine MRI. Magn Reson Med. 53, 159-168, doi:10.1002/mrm.20331 (2005).
Figures