0038
Highly Accelerated Wave-CAIPI 3D SPACE FLAIR Compared to Standard 3D SPACE FLAIR for Epilepsy Imaging at 3T1Department of Radiology, Massachusetts General Hospital, Boston, MA, United States, 2Department of Radiology, Athinoula A. Martinos Center for Biomedical Imaging, Charlestown, MA, United States, 3Department of Radiology, Siriraj Hospital, Bangkok, Thailand, 4Siemens Shenzhen Magnetic Resonance Ltd., Shenzhen, China, 5Siemens Healthcare GmbH, Erlangen, Germany, 6Siemens Medical Solutions Inc., Boston, MA, United States
Synopsis
We performed a systematic comparison of highly accelerated Wave-CAIPI 3D SPACE FLAIR versus standard 3D SPACE FLAIR for the imaging evaluation of 77 patients with seizures or established epilepsy undergoing 3T MRI. There were no significant differences between the two sequences for the detection of lesions and overall diagnostic quality, despite a 2.5- to 4-fold decrease in acquisition time using Wave-CAIPI SPACE FLAIR. The application of highly accelerated 3D imaging using Wave-CAIPI technology may improve use of MRI resources while reducing motion artifacts and patient anxiety.
Introduction
High spatial resolution magnetic resonance imaging (MRI) is essential to the diagnosis and treatment of epilepsy. MRI has become the primary tool for the precise identification of lesions, particularly when surgery is being considered in the management of drug-resistant epilepsy1. High-resolution FLAIR sequences, such as SPACE, CUBE, or VISTA, are best suited for assessing signal abnormalities at the gray-white matter interface and to detect gray matter hyperintensities2. However, these three-dimensional (3D) isotropic sequences have prolonged acquisition times, which contribute to patient anxiety and increased artifacts due to motion3. The goal of this study was to investigate the diagnostic performance of an accelerated Wave-CAIPI 3D SPACE FLAIR (Wave-SPACE FLAIR) sequence that provides 2.5- to 4-fold reduction in acquisition time compared to standard 3D SPACE FLAIR in patients undergoing evaluation of seizures.Methods
Under an IRB-approved and HIPAA compliant protocol, 77 patients undergoing brain MRI for the evaluation of seizures or established epilepsy were prospectively enrolled. All patients were scanned on a 3T MRI system (MAGNETOM Prisma, Siemens Healthcare, Erlangen, Germany). In addition to conventional structural imaging sequences, all patients were scanned with a prototype isotropic 3D Wave-CAIPI SPACE FLAIR sequence4 (acceleration factor [R] = 9, acquisition time [TA] = 1:50 min on a 32-channel coil, or R = 6, TA = 2:45 min on a 20-channel coil) and a standard 3D SPACE FLAIR sequence (R = 2, TA = 7:15 min for both coils). Two neuroradiologists (9 and 8 years of experience) blinded to sequence type performed an independent head-to-head comparison of both image series. The assessment of findings relevant to epilepsy diagnosis, including the visualization of cortical, white matter, deep gray matter, infratentorial, and hippocampal lesions, were rated using a predefined 5-point scale. Reviewers also evaluated the presence of pulsation artifacts (due to blood or CSF flow), motion artifacts, noise, and the overall diagnostic quality. A third neuroradiologist with over 20 years of experience adjudicated any discrepancies between the initial reviewers. We tested for non-inferiority of Wave-SPACE FLAIR compared to the standard sequence in the head-to-head analysis. A non-inferiority margin (Δ) of 15% was chosen with the null hypothesis that the proportion of cases where standard SPACE FLAIR was preferred over Wave-SPACE FLAIR was > 15%.Results
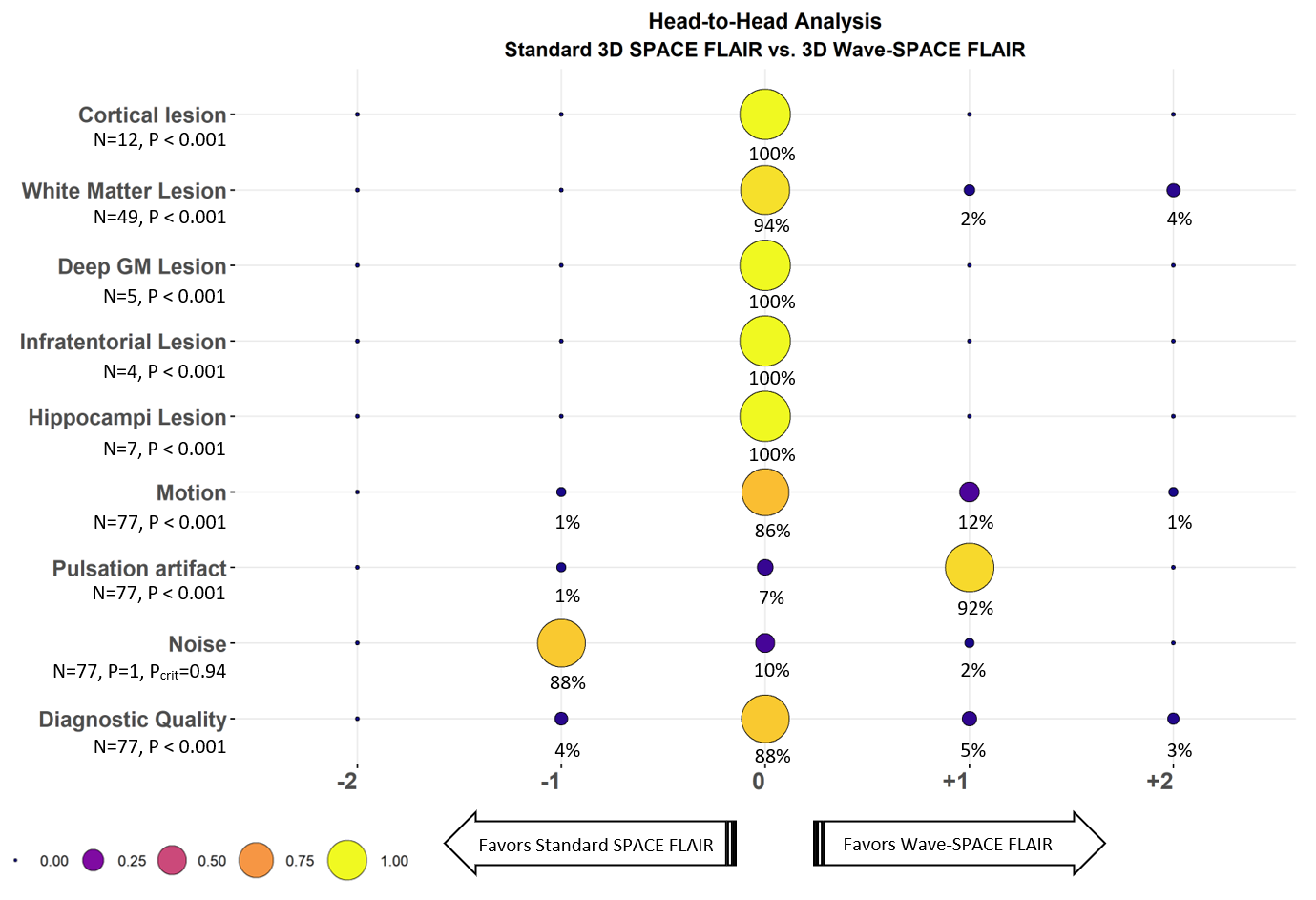
All 77 patients were successfully evaluated. We found abnormal signal intensity lesions on both Wave and standard SPACE FLAIR images in the cortex (12 cases, 15.6%), in the white matter (49 cases, 63.3%), in the deep gray matter (5 cases, 6.5%), in the infratentorial compartment (4 cases, 5.2%), and in the hippocampi (7 cases, 9%). 3D Wave-SPACE FLAIR was non-inferior to the standard 3D SPACE FLAIR for detection of lesions in all locations (P < 0.001), with 100% agreement between raters in the visualization of cortical, deep gray matter, infratentorial and hippocampal lesions. The lesions in the white matter were rated as equally visualized in 46/49 cases (93.8%) and were better visualized with Wave-SPACE FLAIR in 3/49 cases (6.2%). Wave-SPACE FLAIR was also non-inferior in the comparison for motion and flow related artifacts, as well as for the overall diagnostic quality (P < 0.001). For motion, Wave-SPACE FLAIR was considered equivalent or preferred over the standard sequence in 76/77 cases (99%). Wave-SPACE FLAIR was preferred over the standard sequence in 71/77 cases (92%) for showing fewer flow related artifacts and was rated equivalent in 5/77 cases (7%). With respect to image noise, however, the standard SPACE FLAIR was preferred in 68/77 cases (88%), was considered equivalent in 8/77 cases (10%), and had the Wave-SPACE FLAIR preferred in only 1/77 cases (2%).Discussion
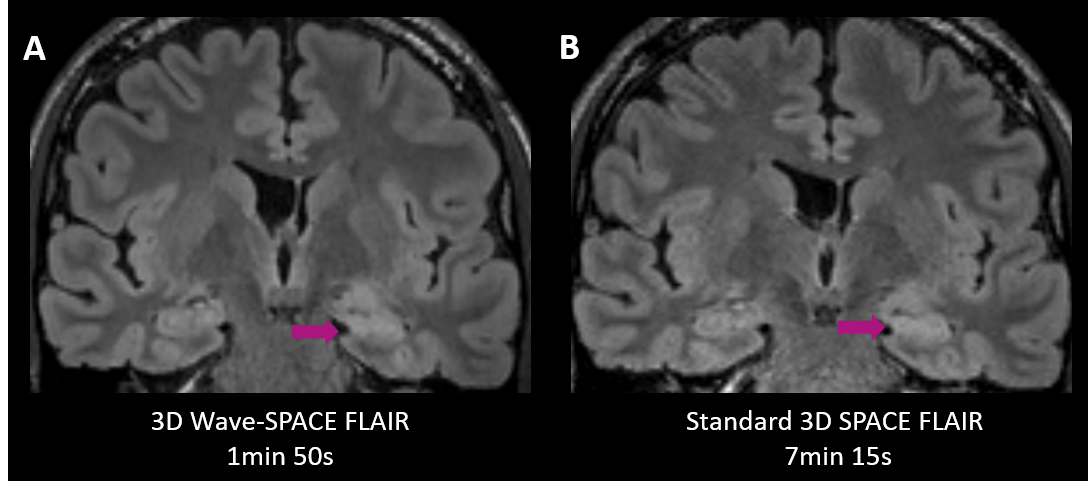
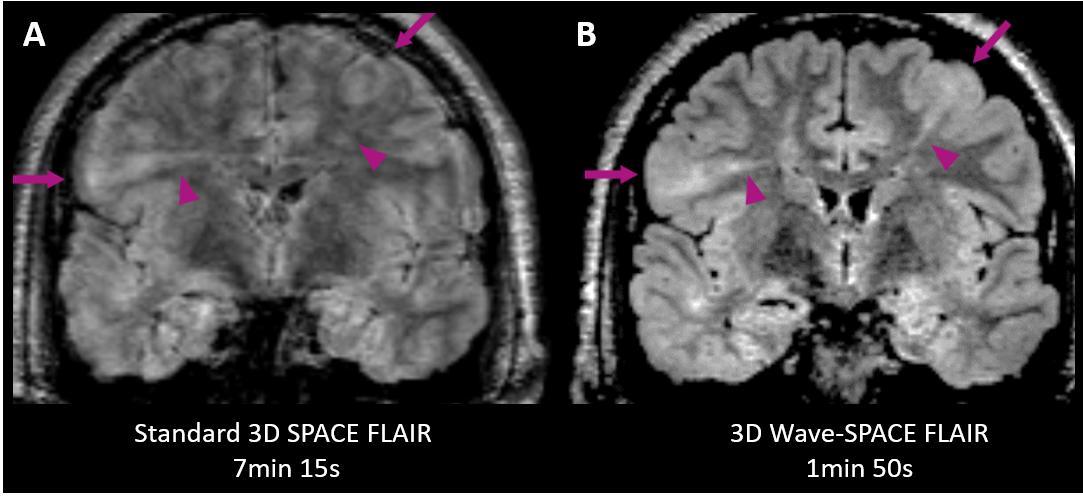
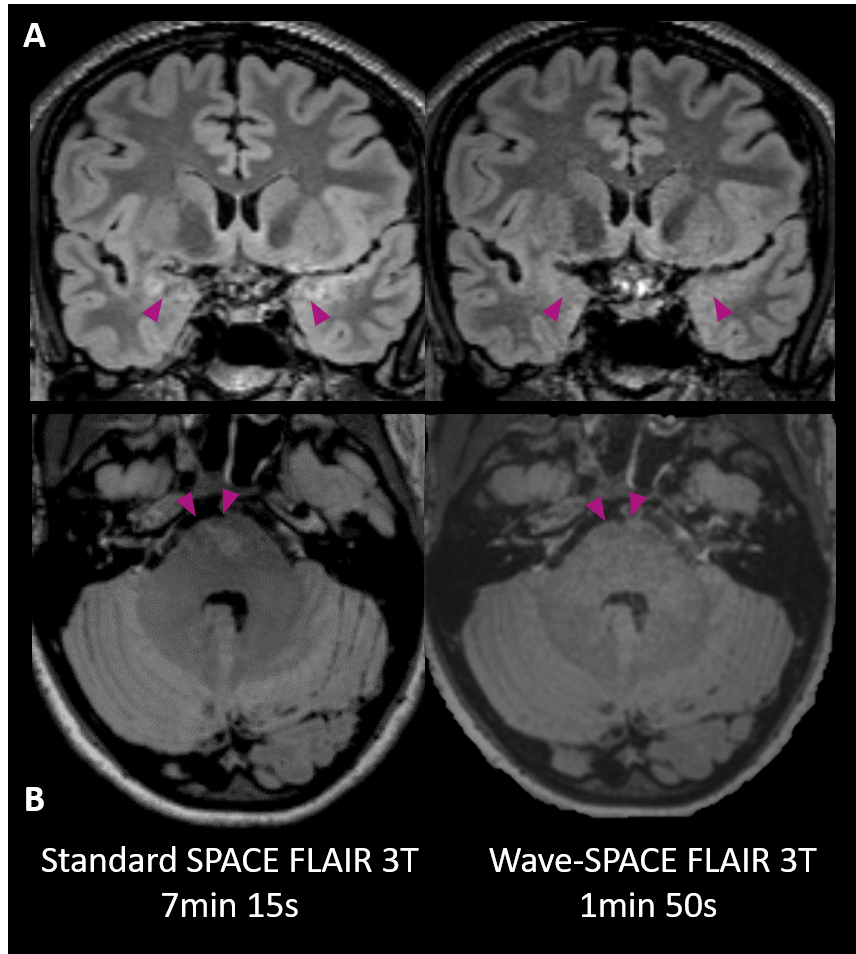
3D Wave-CAIPI SPACE FLAIR was non-inferior to standard 3D SPACE FLAIR for detection of lesions in the cortex, white matter, deep gray matter, infratentorial compartment and hippocampi, and was 4x faster with a 32-channel coil (1:50 min vs 7:15 min) and 2.5x faster with a 20-channel coil (2:45 min vs 7:15 min). Our findings show that the highly accelerated Wave-SPACE FLAIR sequence provides comparable diagnostic performance with reduced motion and flow-related artifacts, at the cost of mildly increased image noise. Moreover, we observed less severe artifacts due to blood or CSF flow in the posterior fossa and around the mesial temporal lobes, which can be particularly beneficial in the evaluation of temporal lobe epilepsy. The results support the understanding that the Wave-CAIPI technique can successfully the accelerate 3D SPACE FLAIR sequence, while providing high resolution multiplanar views for the optimal diagnosis of epileptogenic lesions and potentially resulting in fewer non-diagnostic exams due to motion.Conclusion
High-resolution 3D imaging is central to the identification of structural lesions in patients with seizures, and the deployment of accelerated imaging techniques may improve the efficiency of these historically lengthy acquisition protocols. Our results suggest that Wave-CAIPI SPACE FLAIR can be adopted in place of standard SPACE FLAIR in epilepsy MRI examinations, decreasing scan time and improving utilization of MRI resources that may ultimately improve access for patients.Acknowledgements
This study was supported by a research grant from Siemens Healthineers.References
1. Bernasconi A, Cendes F, Theodore WH, et al. Recommendations for the use of structural magnetic resonance imaging in the care of patients with epilepsy: A consensus report from the International League Against Epilepsy Neuroimaging Task Force. Epilepsia. 2019;60(6):1054-1068. doi:10.1111/epi.15612
2. Mellerio C, Labeyrie MA, Chassoux F, et al. 3T MRI improves the detection of transmantle sign in type 2 focal cortical dysplasia. Epilepsia. 2014;55(1):117-122. doi:10.1111/epi.12464
3. Havsteen I, Ohlhues A, Madsen KH, Nybing JD, Christensen H, Christensen A. Are movement artifacts in magnetic resonance imaging a real problem?-a narrative review. Front Neurol. 2017;8(MAY):1-8. doi:10.3389/fneur.2017.00232
4. Bilgic B, Gagoski BA, Cauley SF, et al. Wave-CAIPI for highly accelerated 3D imaging. Magn Reson Med. 2015;73(6):2152-2162. doi:10.1002/mrm.25347
Figures