0017
Predictive Value of Myo-inositol Measured by MRSI during Anti-angiogenic Treatment in Recurrent Glioblastoma1Radiology / Martinos Center for Biomedical Imaging, Massachusetts General Hospital, Charlestown, MA, United States, 2Neurology / Cancer Center, Massachusetts General Hospital, Boston, MA, United States, 3Radiology, Massachusetts General Hospital, Boston, MA, United States, 4Neurosurgery, Massachusetts General Hospital, Boston, MA, United States, 5Neurology, Brigham and Women's Hospital, Boston, MA, United States
Synopsis
Patients with recurrent glioblastoma (rGBM) are commonly treated with anti-angiogenic agents such as bevacizumab (BEV), but not all benefit from this therapy. We examined whether MR spectroscopic imaging (MRSI) of myo-inositol (mI) could distinguish short-term survivors from longer term survivors (>9 month). We scanned twenty-two rGBM patients with MRSI at baseline prior to bevacizumab-based therapy, as well as 1-2 days, 4 weeks, 6-8 weeks and 16 weeks after treatment. We found that low tumoral myo-inositol normalized by creatine (Cr) on the contralateral site (mI/c-Cr) prior to and during anti-angiogenic therapy is predictive of poor survival.
Introduction
Glioblastomas are among the most challenging cancers to treat, and long term favorable clinical outcomes in patients with rGBM are difficult to achieve [1]. Treatment with anti-angiogenic agents, such as BEV, has shown promise in prolonging progression-free survival and improving quality of life in some patients, but it is difficult to predict who benefits from such treatment. Because the use of BEV is associated with substantial reduction in contrast enhancement on T1-weighted MRI, it is often difficult to distinguish a favorable tumoral response from pseudo-response using conventional MRI [2, 3]. Our group and others have shown that intermediate TE MRSI can detect treatment failure to BEV through changes in N-Acetylaspartate (NAA), Choline (Cho) and Lactate over time [4, 5], but not at baseline. Myo-inositol (mI) is an osmo-regulator in the brain that is elevated in low grade tumors and decreased in high grade tumors, and it can be measured with short TE MRSI [6]. We hypothesize that mI, among other metabolites, can predict response to BEV and clinically distinguish short-term survivors from longer-term survivors (> 9 month).Methods
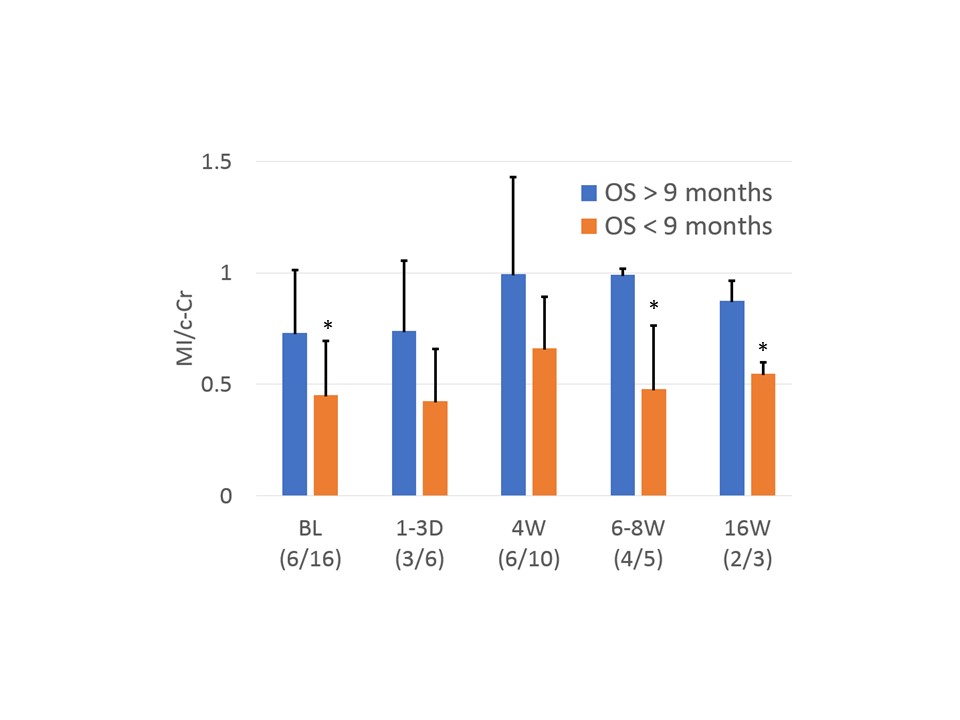
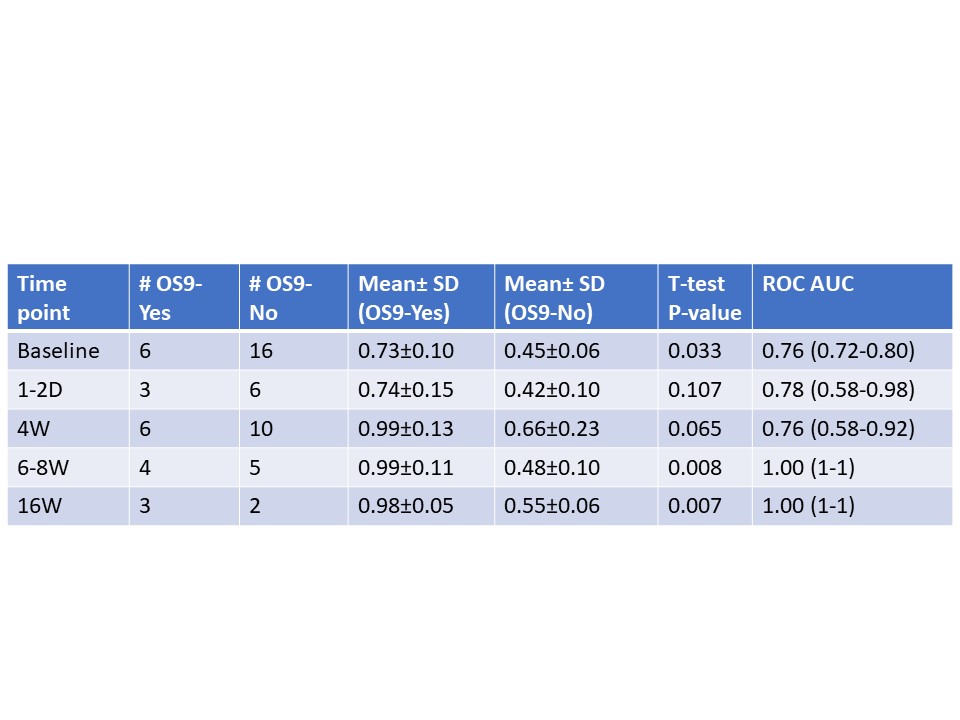
Twenty-two patients with rGBM underwent either 2D or 3D MRSI on Siemens or GE scanners at either 3T or 1.5T (Acquisition parameters included TR/TE = 1700/30 ms, Siemens: LASER Spiral MRSI [7]; GE: PRESS, phase encoding, resolution = 1-2 cm3, acquisition time = 5-6.5 min.) Scans were acquired at baseline (BL) prior to treatment, as well as 1-2 days, 4 weeks, 6-8 weeks and 16 weeks after treatment. All subjects were treated with BEV monotherapy, or BEV-based chemotherapy with either lomustine, temozolomide, or pembrolizumab. The MRSI data were overlaid on the post-contrast T1-weighted images. Voxels were classified into contrast enhancing tumor, non-enhancing peritumoral area (periphery), and contralateral normal white matter (Figure 2). Of note, tumor voxels identified in the baseline scan were followed throughout the visits regardless of enhancement. MRSI data were analyzed using LCModel to quantify metabolites mI, Cr, NAA and Cho averaged across the tumor as previously described[4]. Metabolites were normalized by Cr in the contralateral hemisphere (mI/c-Cr). Receiver operating characteristic (ROC) curves were constructed using overall survival at 9 months (OS-9) as the outcome measure. Furthermore, t-tests were performed between 9-month survivors and non-survivors at all timepoints. Figure 1 shows short TE MRS spectra for patients with low and high mI levels.Results
Table 1 summarizes the patient demographics. Of the 22 patients, 6 survived past 9 months. Figure 2 shows lower mI/c-Cr ratios at baseline in the tumor compared to periphery (p<0.0001), and contralateral hemisphere volumes of interest (VOI) (p<0.0001). Periphery mI/c-Cr ratios were also lower compared to contralateral mI/c-Cr (p=0.0068). Lower mI levels in the tumor relative to periphery and contralateral VOIs are consistent with the prevailing theory that higher-grade tumors have lower mI. Ratios of mI/c-Cr in the tumor at BL were significantly higher in the 9-month survivors than non-survivors (p=0.033). Analysis of the areas under the ROC curves (AUC) revealed that mI/Cr at baseline predicted OS-9 (AUC=0.76). Furthermore, mI/c-Cr was higher in 9-mo survivors relative to non-survivors at 6-8, and 16 weeks post BEV-based therapy (Figure 3, Table 2).Conclusion
Lower mI levels prior to and during anti-angiogenic therapy are predictive of poor survival. Low mI levels might be a consequence of disruption of the blood-brain barrier leading to a disturbance of osmotic equilibrium, and increased leakage [8, 9]. Future work will combine intermediate and short TE MRS metabolic markers with traditional MR metrics, including cerebral blood volume with dynamic susceptibility contrast imaging.Acknowledgements
This research was supported by NIH/NCI grants R01CA190901 and R01CA129371. We would like to thank all participating MGH Neuro-oncologists, Cancer Center and Radiology staff, and Quantitative Tumor Imaging staff for assisting in this study. We also thank all patients and their families.References
1. Stupp R, Mason WP, van den Bent MJ, Weller M, Fisher B, Taphoorn MJ, et al. Radiotherapy plus concomitant and adjuvant temozolomide for glioblastoma. N Engl J Med. 2005;352(10):987-96.
2. Hygino da Cruz LC, Jr., Rodriguez I, Domingues RC, Gasparetto EL, Sorensen AG. Pseudoprogression and pseudoresponse: imaging challenges in the assessment of posttreatment glioma. AJNR Am J Neuroradiol. 2011;32(11):1978-85.
3. Jain RK. Normalization of tumor vasculature: an emerging concept in antiangiogenic therapy. Science. 2005;307(5706):58-62.
4. Ratai EM, Zhang Z, Snyder BS, Boxerman JL, Safriel Y, McKinstry RC, et al. Magnetic resonance spectroscopy as an early indicator of response to anti-angiogenic therapy in patients with recurrent glioblastoma: RTOG 0625/ACRIN 6677. Neuro Oncol. 2013;15(7):936-44.
5. Nelson SJ, Li Y, Lupo JM, Olson M, Crane JC, Molinaro A, et al. Serial analysis of 3D H-1 MRSI for patients with newly diagnosed GBM treated with combination therapy that includes bevacizumab. J Neurooncol. 2016;130(1):171-9.
6. Castillo M, Smith JK, Kwock L. Correlation of myo-inositol levels and grading of cerebral astrocytomas. AJNR Am J Neuroradiol. 2000;21(9):1645-9.
7. Andronesi OC, Gagoski BA, Sorensen AG. Neurologic 3D MR spectroscopic imaging with low-power adiabatic pulses and fast spiral acquisition. Radiology. 2012;262(2):647-61.
8. Papadopoulos MC, Saadoun S, Binder DK, Manley GT, Krishna S, Verkman AS. Molecular mechanisms of brain tumor edema. Neuroscience. 2004;129(4):1011-20.
9. Steidl E, Pilatus U, Hattingen E, Steinbach JP, Zanella F, Ronellenfitsch MW, et al. Myoinositol as a Biomarker in Recurrent Glioblastoma Treated with Bevacizumab: A 1H-Magnetic Resonance Spectroscopy Study. PLoS One. 2016;11(12):e0168113.
Figures
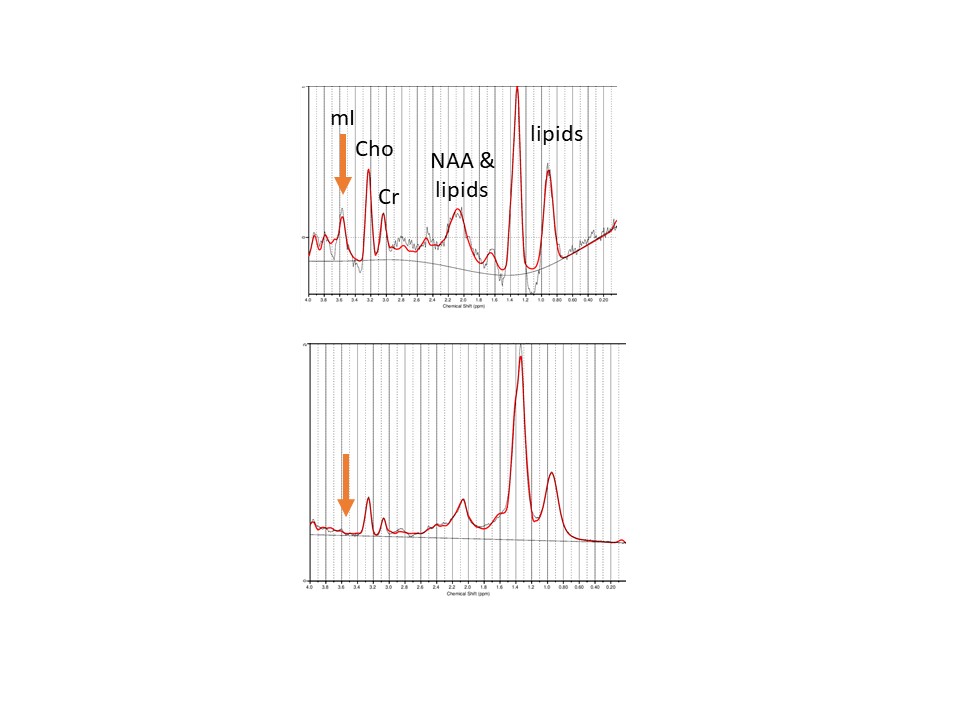
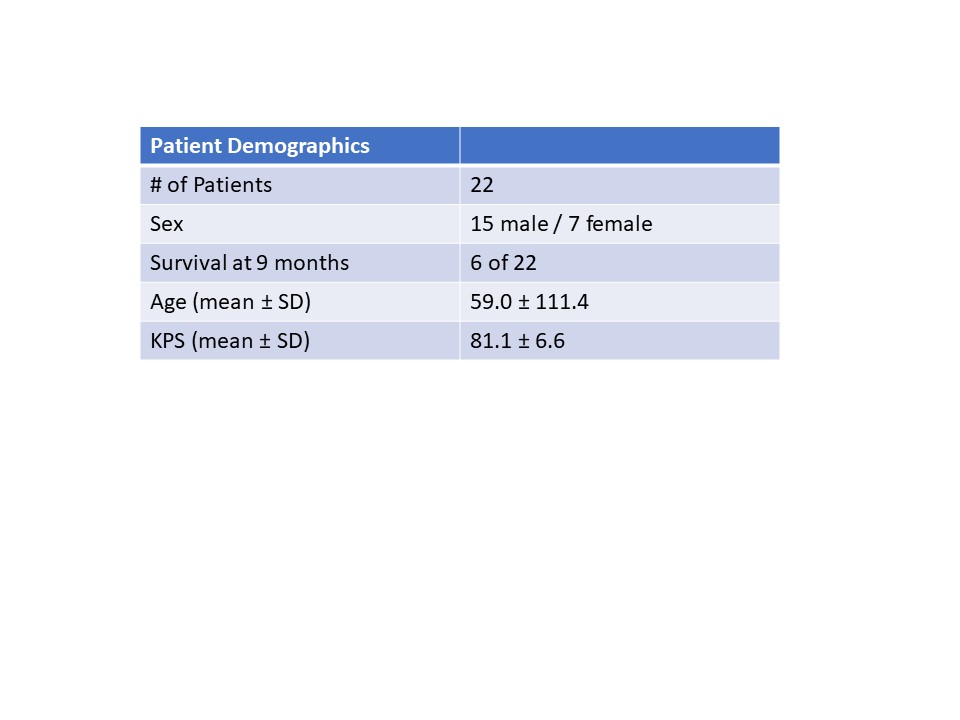

Figure 2. Left: Representative MRS voxel selection on a T1WI post-contrast image, tumor voxels (red), peritumoral (green), and contralateral normal voxels (blue) were selected for analyses.
Right: mI/c-Cr ratios at baseline in the tumor, (T) periphery (P), and contralateral (C) volumes of interest (VOI). Box plots indicate quartiles. Mean and standard deviations of mI/c-Cr in each VOI with t-tests indicating each VOI pair is significantly different.