S78
Evaluation of an ultra-fast 4D MRI sequence for the diagnosis of breast lesions1Master of Science in Health Sciences, HES-SO /UNIL, Lausanne, Switzerland, Lausanne, Switzerland, 2Institut de radiologie, Clinique des Grangettes, Chêne-Bougeries, Geneva, Switzerland, Geneva, Switzerland, 3Geneva School of Health Sciences, HES-SO // University of Applied Sciences and Arts of Western Switzerland, Geneva, Switzerland
Synopsis
Breast MRI is promoted as a tool for breast cancer screening because of its high sensitivity. Possibility of differentiating between benign and malign lesions has been studied using lesion enhancement parameters on DCE, thus helping to reduce examination time. This study was designed to verify sensitivity and specificity for lesion characterization. Time to Enhancement and Maximum Slope of the enhancement curve obtained from an ultrafast sequence were evaluated. Preliminary results tend to confirm that performing breast lesions screening using ultrafast-DCE is a valuable alternative to the standard MRI Breast protocol, possibly opening diagnostic perspectives to a wider population of women.
Purpose
Breast MRI is promoted as a tool for breast cancer screening because it is a very sensitive technique [1]. At present, a complete breast MRI examination lasts about 20 minutes according to clinical protocols, but the possibility of shortening the examination time (3 minutes) [2], by focusing on important sequences such as the DCE sequences is increasingly investigated [3], thus helping to reduce examination time and accessibility of the MRI for women. Lesion differentiation between benign and malignant can be performed with ultrafast dynamic contrast enhanced sequences using kinetic parameters within the first post contrast minute. This study was designed to verify sensitivity and specificity for lesion characterization in a clinical high-risk setting including 24 patients after informed consent. We evaluated specifically Time to Enhancement and Maximum Slope of the enhancement curve obtained from a 4D-THRIVE MRI sequence and compared results with histopathology and/or follow-up.Methods
24 breast MRI examinations with visible lesions and performed with a Philips 3T Ingenia MRI scanner were retrospectively collected. The early enhancement kinetics parameters acquired with 4D-THRIVE sequence were analyzed using a Philips Intellispace© console. Maximum slope and Time to enhancement performances in differentiating benign from malignant lesions were evaluated [4,5]. The MS was calculated using Intellispace© automatic parameters calculation (MS1) and manually calculating the steepest part of the MRI signal time evolution (ΔSI/ΔT) (MS2). The agreement between these two methods was assessed. Cutoff values for classification of the lesions in 3 curve types [4] (<5.5%/sec = Type I; >5.5%/sec to <9%/sec = Type II; >9%/sec =Type III) were defined, given by MS values and lesion morphology, on a training data set different from the test dataset described and evaluated here. TTE was calculated as the difference between the time of visible enhancement of the lesion and the time of visible enhancement in the aorta. Both MS and TTE diagnosis were confronted to the histopathology and/or with the follow-up. To assess intra and inter observer variability, three ROI (Region of Interest) per lesion were performed by two expert MR technologists and four novice MR technologists. ROC analysis was performed to compare MS and TTE.This pilot study was approved by the Ethics Committee Geneva (CCER). Project-ID: 2019-0716.
Results
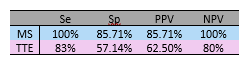
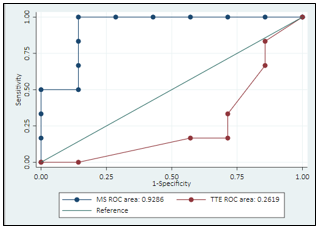
A total of 26 lesions were identified: 15 were benign (including 9 lymph nodes), 8 were malignant and 3 were uncertain lesions, as there was no histopathological result. Lymph nodes and patients who received chemotherapy treatment were excluded. Our first results show that MS performs better than TTE, with regards to sensitivity and specificity. (table 1)Following ROC analysis (Figure 1), areas under curve (AUC) of 0.93 and 0.26 were respectively computed for MS and TTE.
Relatively good agreement between the two MS methods was found (figure 2), but we observed that non-continuous enhancement curves (e.g., caused by potential respiratory movements) worsened the agreement. This explains one of the measurements with very low agreement.
Preliminary results for the intra-observer evaluation suggest good reproducibility for observer A, and good agreement between observers. However, some results show bad inter observer agreement especially in lesions with complex morphology, suggesting a possible learning curve for novice radiographers that was not evaluated in this study.
The main limitation of our study is the small size of the collected dataset and the frequent presence of lymph nodes in our data.
Conclusion
MS calculation appears to be more robust and performs better than TTE estimation in differentiating benign from malignant lesions. The two methods of MS calculation can be used because of the good agreement. The first results of intra observer assessment suggest a good reproducibility. We are currently including more patients as more data are required for a quantitative analysis. Our Preliminary results tend to confirm that performing breast lesions screening using ultrafast dynamic MRI is a valuable alternative to the standard – more time consuming – MRI Breast protocol, possibly opening diagnostic perspectives to a wider population of women.Acknowledgements
No acknowledgement found.References
[1] Kuhl, CK & Schild, H. (2000). Dynamic image interpretation of MRI of the breast. Journal of magnetic Resonance. 12:965-974
[2] Kuhl, CK., Schrading, S., Strobel, K., Schild, HH., Hilgers, R-D., & Bieling. H.B. (2014). Abbreviated Breast Magnetic Resonance Imaging (MRI): First Postcontrast Subtracted Images and MaximumIntensity Projection—A Novel Approach to Breast Cancer Screening With MRI. Journal of Clinical Oncology 32, (22): 2304 10.
[3] Sheth, D., & Hiroyuki Abe. (2017). Abbreviated MRI and Accelerated MRI for Screening and Diagnosis of Breast Cancer. Topics in Magnetic Resonance Imaging 26, (5): 183 89 4.
[4] Mann, R.M, Mus, R.D., Van Zelst, J., Geppert, C., Karssemeijer, N. & Platel, B. (2014). A novel approach to Contrast-Enhanced Breast Magnetic Resonance Imaging for Screening: High-Resolution Ultrafast Dynamic Imaging. Investigative Radiology, 49 (9) 579-685.
[5] Mus, R.D, Borelli, C., Bult, P., Weiland, E., Karssemeijer, N., Barentsz, J.O., Gubern-Merida, A., Platel, B. & Mann, R.M. (2017). Time to enhancement derived from ultrafast breast MRI as novel parameter to discriminate benign from malignant breast lesions. European Journal of Radiology 89, 90-96.
Figures