S74
Respiratory Pacing – A Low-Tech Solution to a Universal Struggle?1Radiology, Johns Hopkins University, Baltimore, MD, United States, 2Canon Medical Research Unit, Mayfield VIllage, OH, United States, 3Cardiology, Johns Hopkins University, Baltimore, MD, United States, 4Canon Medical Systems, Otawara-Shi, Tochigi, Japan
Synopsis
For respiratory triggered and gated acquisitions, variance in the natural respiratory cycle often complicates workflow, extending scan times and reducing image quality. This abstract discusses the hypothesis that by providing continuous auditory guidance, or "respiratory pacing", the efficacy of respiratory triggered and gated sequences may be improved. The importance of mimicking natural respiratory patterns was quickly noted, as were key differences in the success of respiratory pacing when applied to different acquisitions. Other interesting observations included an observable increase in diaphragmatic travel when respiratory pacing was applied and the extension of scan lengths due to diaphragmatic fatigue over time.
Background:
Despite many emerging technologies, respiratory motion artifact remains problematic in magnetic resonance imaging (MRI). Many standard techniques still require the complicated coordination of image acquisition with specific moments in each patient’s physiologic respiratory cycle(1,2,3). Protocols commonly requiring such coordination (e.g.: 3D assessment of biliary ducts and coronary arteries) generally defeat respiratory artifacts by applying a "gating" or "triggering" method (Figure 1) . Unfortunately, even with such methods in place, patient-specific respiratory cycle variation throughout the scan duration can cause complications such as:- Extended scan time due to slowed respiration or diaphragmatic shift outside of established acceptance and/or trigger threshold
- Reduced image quality should respiration increase to a point that acquisition points are no longer targeted to stationary periods
Teaching Points:
In the following IRB-approved investigation, a variety of 3D acquisitions were obtained on five separate subjects using a 3T Galan MR Scanner (Canon Medical Systems). The three most common methods of respiratory gating/triggering were employed: 2D RMC ("Realtime Motion Correction" using a single low Flip Angle navigator beam centered on diaphragm); 1D RMC ("Realtime Motion Correction" using continuous gating with two crossed navigator pulses centered on diaphragm); and Respiratory Gating triggered by an external sensor placed atop patient's torso at the point of maximum expansion following inhalation and monitored by an MR conditional gating device [Invivo MRI SpO2 transmitter].Our preliminary attempts to incorporate RP relied upon pre-recorded instructions that continuously guided patients to breathe "in-in-in" and "out-out-out", with each change of respiratory direction demarcated by the beat of a merged metronome track. This approach suffered from two significant limitations:
- Using the same beat for alternating both inspiration and expiration meant the proposed cycle was divided into equal parts. This posed a problem as the typical respiratory pattern of adults consists of a 1:2 ratio of inspiration vs. expiration(4); patients reported difficulty in maintaining the equally divided respiratory pattern.
- Pre-recording the track required significant preparation and resulted in a track with inflexible timing. Providing real-time modifications became difficult; each patient was forced to conform to the same timing.
Patients were able to match the metronome-based RP without significant issue. However, the ability to follow along with the specified respiratory pace did not necessarily improve all outcomes. In fact, in our initial tests, we found that scan length for gated coronary artery acquisitions was negatively affected, with an average increase of over 22% when RP was applied (Figure 2). This phenomenon was attributed to an observed increase in diaphragmatic movement when respiratory pacing was applied (Figure 3). In coronary artery acquisitions, where continuous scanning is acquired and points falling outside of the user-defined threshold are discarded, the increased diaphragmatic travel led to a decrease in accepted data and subsequently extended scan time.
For triggered sequences, this increased movement did not cause a problem, as triggers were still steadily received and shot sizes were small enough to avoid blur. Additionally, when RP was targeted near the patient's natural rate, decreases in scan length were often observed, with an average decrease of 14% on triggered sequences using optimized RP (Figure 4).
Summary of Conclusions:
Patients subjected to respiratory pacing were capable of successfully modifying their respiratory rates. This can be specifically impactful for prolonged acquisitions using standard respiratory triggering. When RP was optimized, we observed encouraging decreases in scan length on triggered sequences without significant impact on image quality (Figures 4 & 5).Unfortunately, when 1D RMC was specifically used, an observed increase in diaphragmatic travel resulted in the exclusion of significant data points. We suspect that this effect could be mitigated by specifically instructing patients to "inhale in a shallow manner" when the metronome beat is heard, however further testing is needed to validate this hypothesis.
Finally, unusual patterns in the waveform detected by the external respiratory bellows sometimes developed when respiration was pushed to rates significantly different from the patient's natural rhythm. For sequencing triggered by these waveforms rather than a navigator beam, careful placement of the external gating device may be critical to success, with the resulting waveform ideally being confirmed with the patient following the pacing track during exam preparation or coil set-up.
Acknowledgements
The authors would like to acknowledge Ben Hoshino and Mahamadou Diakite, both from CMRU, for their valuable help in logging key data.References
(1) Zaitsev, M. et al., Motion Artifacts in MRI: A Complex Problem with Many Partial Solutions. (2015). Journal of Magnetic Resonance Imaging. doe: DOI: 10.1002/jmri.24850
(2) Scott, A. D., Keegan, J., & Firmin, D. N. (2009). Motion in Cardiovascular MR Imaging. Radiology, 250(2), 331–351. doi: 10.1148/radiol.2502071998
(3) Lewis, C. E., Prato, F. S., Drost, D. J., & Nicholson, R. L. (1996). Comparison of Respiratory Triggering and Gating Techniques for the Removal of Respiratory Artifacts in MR Imaging. Radiology, 160, 803–810. Retrieved from https://mriquestions.com/uploads/3/4/5/7/34572113/resp_gatingradiology2e1602e32e3737921.pdf
(4) Thompson, C. University of Sydney. Anesthesia Discipline. (2018, September 7). VENTILATION, VENTILATORS and HUMIDFICATION. Retrieved from http://www.anaesthesia.med.usyd.edu.au/resources/lectures/ventilation_clt/ventilation.html.
(5) My Metronome, Groove Vibes, LLC
Figures
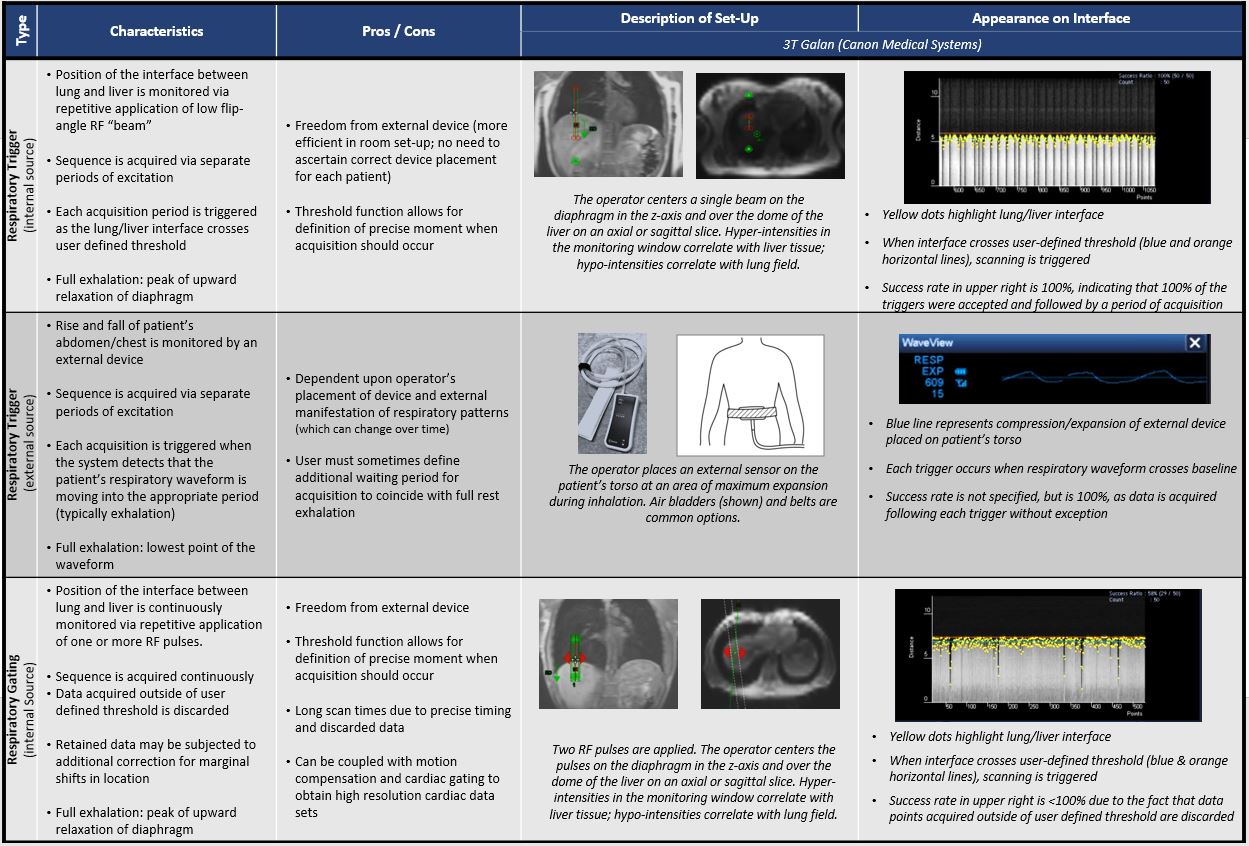
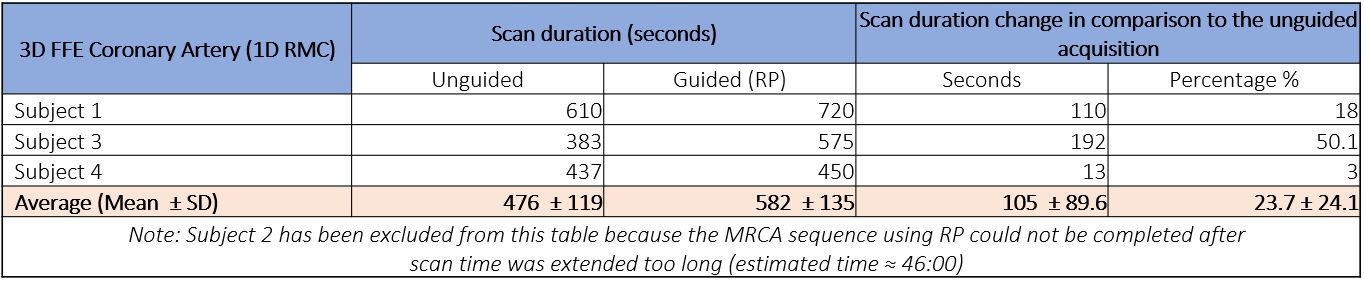
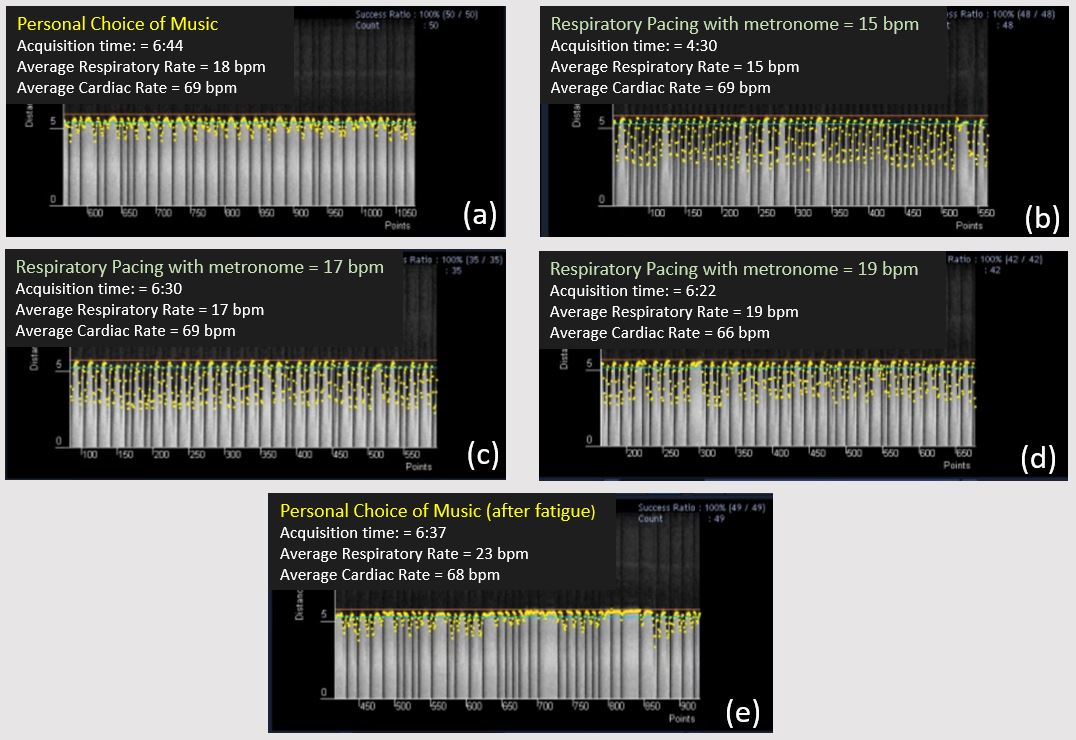
Figure 3: Screen captures showing M-Power system interface (Canon Medical Systems) for respiratory triggering via 2D RMC navigator pulse.
Of note, acquisitions acquired with RP (b, c, d) show increased diaphragmatic travel versus those acquired during the patient’s natural cycle (a & e). Additionally, diaphragmatic fluctuations become evident in repeat of non-RP triggered acquisition (e), indicating potential fatigue, and eliciting greater variance in diaphragmatic motion versus original scan (a).
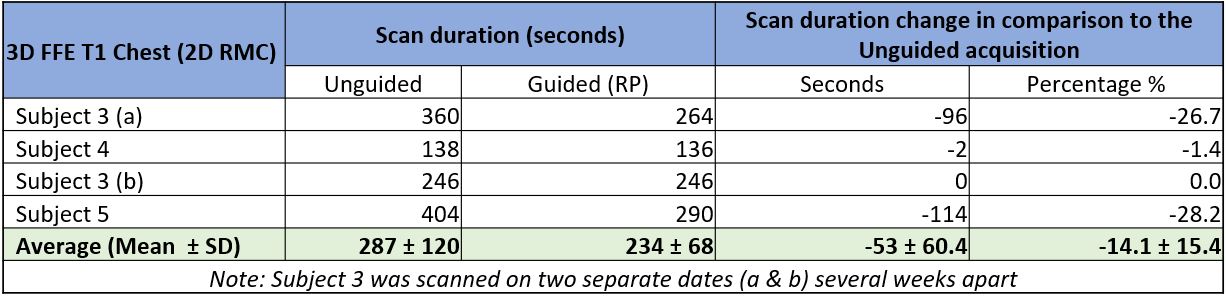
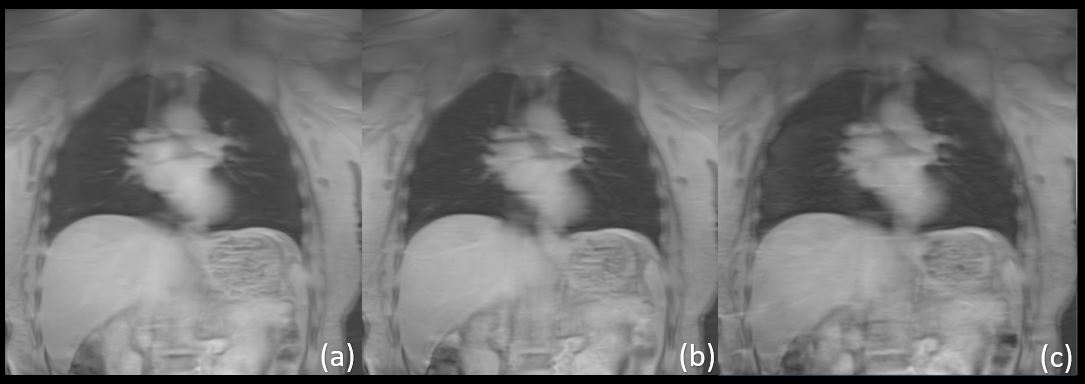
Figure 5: Qualitative Image Review: (a) = Personal choice of music; (b) = Patient subject to RP = 15 BPM; (c) = Repeat of (a) after fatigue. Images display similar sensitivity to detail, clarity and signal to noise ratio.
Protocol: FFE3D; TR 4.9ms; TE 1.9ms; FA 20; FOV 40x40; Matrix: 384 x 384; Slice thickness: 8m; continuous scan time ≈ 3:00