Abbreviated breast MRI: How have we achieved it?
1Radiology, Royal Melbourne Hospital, Melbourne, Australia
Synopsis
An abbreviated breast MRI protocol has been developed utilising an ultrafast view sharing technique.
Background
Given the now global recognition that breast MRI demonstrates the highest sensitivity of all imaging modalities1, the demand for breast MRI continues to escalate. Several international studies have been conducted to determine if an abbreviated breast MRI protocol provides the same information, as a standard MRI2. The initial studies have demonstrated a lack of specificity due to the absence of dynamic enhancement data. This has occurred in an attempt to accelerate protocols by the truncation of the traditional 4-5 dynamic scans acquired up to 7 minutes post contrast. The advent of ultrafast scanning has provided the opportunity to bring breast screening MRI closer to fruition. The more recent studies have demonstrated that an ultrafast protocol enables detection of an equal number of cancers when compared to a standard protocol3. The use of ultrafast view sharing techniques provides higher temporal and spatial resolution, enabling characterization of breast lesions by utilizing a time intensity curve obtained during the first minute of scanning post contrast4.Teaching Point
Our breast MRI protocol has evolved from the standard protocol, utilizing a 30 minute MRI scanner allocation, to an abbreviated ultrafast protocol taking a 15-20 minute scanner allocation. This is very patient dependent driven by whether the patient is a first timer or a serial attendee. Over the last 18 months we have trialed various combinations of sequencing to meet the needs of lesion detection, whilst improving scanner efficiency, and decreasing radiologist interpretation time.We utilize a Siemens 3T Skyra, 16Ch Sentinelle breast coil, gadobutrol by weight, a power injector at a rate of 2.0mls/sec and a saline flush. The standard breast MRI protocol consists of an Axial T2 SPAIR, T1WI, T1 3D VIBE pre and 4 post contrast dynamic VIBEs, and DWI. This entails 20 minutes of scanning and 7 minutes of patient turnaround time. After several versions the current abbreviated protocol utilizes a key sequence,TWIST-VIBE with a voxel of 1 x 1 x 2mm. This aims to replace the 4 passes of the usual dynamic sequence. There is a decrease in the acquisition time enabling the faster imaging of the inflow of contrast and the generation of time intensity curves. The TWIST-VIBE with water excitation is acquired in between a high resolution T1WI fat saturated VIBE sequence immediately before and during contrast administration for 57 seconds. A T2 SPAIR is also acquired to assist with lesion classification, where a T2 hyperintensity may confirm a benign finding and the fat saturated image assists in the evaluation of fat necrosis2. DWI is no longer acquired. This protocol has an 8 minute scan time and approximately 7 minute patient turnaround time (Fig.1). The 11 phases of the TWIST-VIBE are acquired with a first pass pre contrast (10.5 secs) allowing the filling of the entire k-space and then the subsequent 10 repetitions (4.5 secs) updating only a small part of the central k-space (zone A= 20%) and randomly sampling a percentage of the peripheral k-space (zone B = 25%). To improve the temporal resolution, we have utilised iPAT with a factor of 2 and also a Caipirinha “Caipi” factor of 2, enabling a total acceleration factor of 4, where by “Caipi” allows data reduction to be carried out in two phase-encoding directions in this 3D acquisition. The TWIST-VIBE sequence affords less motion artifacts than the VIBE due to the fast acquisition and data sharing between the dynamic phases, however, there is the presence of artifacts in the upper outer quadrant due to the decrease in signal to noise ratio3.
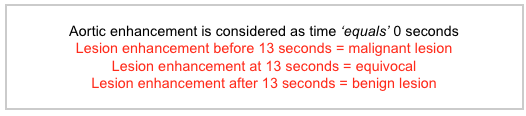
A new diagnostic sign has also been detected with the utilization of the TWIST-VIBE. The presence of afferent vessels is a depiction of dynamic enhancement of breast cancer due to tumoral neoangiogenesis. Breast cancers enhance faster than glandular and benign lesions. This sign increases the specificity as the risk of cancer is 26 x greater when afferent vessels are present3. Another key indicator is the time to enhancement (TTE) during a TWIST-VIBE sequence, and it is the time between where the aorta begins to enhance and where a lesion begins to enhance. This is an important parameter for distinguishing a malignant lesion from a benign one (Fig.2)5 . This finding has correlated well to pathological testing of lesions that have been biopsied and excised, confirming that fast acquisition times are important in distinguishing benign from malignant lesions.
Summary
The limitations of breast MRI to date have included the high cost, study length, the use of contrast, reduced specificity and the interpretation time of thousands of images acquired in a standard protocol. With the current set of sequences, our center is demonstrating high sensitivity and specificity in the class of women with a high risk and those with dense breast tissue, due to the improved contrast over mammography. The sensitivity and specificity of the sequence is equal to the standard protocol. There is no ionizing radiation which is important when high risk women may begin their screening regime early in life. Faster scanning has the additional benefit of improved patient tolerance, and increased efficiency, potentially making MRI of the breast more readily available as a screening modality for moderate to high risk patients.Acknowledgements
A special mention to Dr Allison Rose who has inspired and provided guidance for this presentation with her passion for MRI breast imaging and drive to make it a workable screening tool.References
1. W.A Berg, et al. Detection of breast cancer with addition of annual screening ultrasound or a single screening MRI to mammography in women with elevated breast cancer risk. JAMA 307 (2012) 1394-1404
2. V. Mango et al. Abbreviated protocol for breast MRI: Are multiple sequences needed for cancer detection? European Journal of Radiology 84 (2015) 65-70
3. G. Oldrini et al. Abbreviated breast magnetic resonance protocol: Value of high-resolution temporal dynamic sequence to improve lesion characterization. European Journal of Radiology 95 (2017) 177-185
4. R. Mann et al. A novel approach to contrast enhanced breast magnetic resonance imaging for screening: high-resolution ultrafast dynamic imaging. Investigative Radiology, 49 (2014) 579-585
5. R. D. Mus et al. Time to enhancement derived from ultrafast breast MRI as a novel parameter to discriminate benign from malignant breast lesions. European Journal of Radiology 89 (2017) 90-96
Figures