S3
Clinical MRI protocol used for patients with cerebrovascular diseases
Helle Juhl Simonsen1, Ulrich Lindberg2, Karina Elin Segers3, Bente Sonne Møller3, and Henrik B.W. Larsson2
1Functional Imaging Unit Dept. of Clinical Physiology, Nuclear Medicine and PET, Rigshospitalet, Glostrup, Hvidovre, Denmark, 2Functional Imaging Unit, Dept. of Clinical Physiology, Nuclear Medicine and PET, Rigshospitalet, Glostrup, Glostrup, Denmark, 3Department of Radiology, Rigshospitalet, Glostrup, Glostrup, Denmark
1Functional Imaging Unit Dept. of Clinical Physiology, Nuclear Medicine and PET, Rigshospitalet, Glostrup, Hvidovre, Denmark, 2Functional Imaging Unit, Dept. of Clinical Physiology, Nuclear Medicine and PET, Rigshospitalet, Glostrup, Glostrup, Denmark, 3Department of Radiology, Rigshospitalet, Glostrup, Glostrup, Denmark
Synopsis
To investigate the cerebral blood flow, patients with Cerebrovascular Disease have previously been referred for a single-photon-emission-computed-tomography scanning with/ maybe without Diamox (a vasodilator). If the patient has perfusion defects on the first SPECT scanning with Diamox, the patient must undergo a new SPECT scanning without Diamox to determine whether the flow defects are due to reduced flow reserve. It is time-consuming examinations in which the patient receives gamma radiation from administered radioactive drug. To prevent patients going through two long examinations and to get a more detailed examination of the cerebrovascular defects, we have set-up a clinical MRI protocol.
Background and aim:
Cerebrovascular Disease (CVD) refers to all states where the blood circulation to a particular part of the brain is temporarily or permanently stopped. Any change in the blood flow can lead to two types of problems: ischemia and hemorrhage. The four most common reasons are: cerebral thrombosis, cerebral embolism, cerebral or intracerebral hemorrhage or subarachnoid bleeding. To investigate the cerebral blood flow (CBF), patients with CVD have previously been referred for a single photon emission computed tomography (SPECT) scanning with and maybe without acetalzolamide (Diamox). Diamox is a vasodilator, so if the patient has perfusion defects on the first SPECT scanning with Diamox, the patient must undergo a new SPECT scanning without Diamox to determine whether the flow defects are due to reduced flow reserve. It is time-consuming examinations in which the patient also receives gamma radiation from an administered radioactive drug. In order to prevent patients going through two long examinations and to get a more detailed examination of the cerebrovascular defects, we have set up a clinical MRI protocol.Methods and Results:
The MRI examination is performed on a 3 T upgraded Philips scanner (Achieva magnet, Ingenia software and with a d-Stream system), equipped with a 32-element receive head coil and MultiTransmit parallel RF transmission. Protocol: The protocol includes anatomical images of the brain, (sagittal and axial T2 TSE, axial FLAIR and a 3D T1TFE), Magnetic Resonance angiography (MRA), Diffusion weighted imaging (DWI), total flow to the brain measured by the phase contrast method, regional perfusion with Arterial Spin Labeling (ASL) before and after administration of Diamox.Example of a patient with cerebrovascular defects referred for an MRI scanning:
Referring information: Previously MRI has shown new ischemic infarct in the temporal / partial area of the brain, in the right hemisphere and also areas with cerebral changes after older infarcts. Ultra sound (UL) shows occlusion of the right internal carotid and severe stenosis in the right external carotid, left internal and external carotid. The patient is referred for a new MRI examination for assessment of the hemodynamic condition. Results: Total flow to the brain increases by 45% after administration of Diamox (Fig.1). CBF measurements (ASL) show severely decreased perfusion in the right temporal/partial area before and after Diamox, which corresponds to the right cerebral artery supply area (Fig. 2) and to the infarcts seen on the FLAIR sequence (not shown). DWI (Fig.3) shows reduced diffusion compatible with relatively new infarction in a smaller area located more medial from the area with the defect blood brain barrier. Right internal carotid is missing on the MRA, due to occlusion (Fig. 3). The other areas of the brain show normal increase of CBF after Diamox. Conclusion: Irreversible perfusion reduction in the right temporal/partial area corresponding to the right cerebral arterial media supply area with no effect of Diamox.Conclusion:
With our new MRI protocol, the clinicians get valuable and adequate information about the blood circulation in patients with cerebrovascular diseases. An MRI scanning will also benefit patients since they only need a 2 hours MRI scanning without radioactive injections, instead of a SPECT scan with radioactive injections, where they may need to meet up for scanning two days.Acknowledgements
No acknowledgement found.References
No reference found.Figures
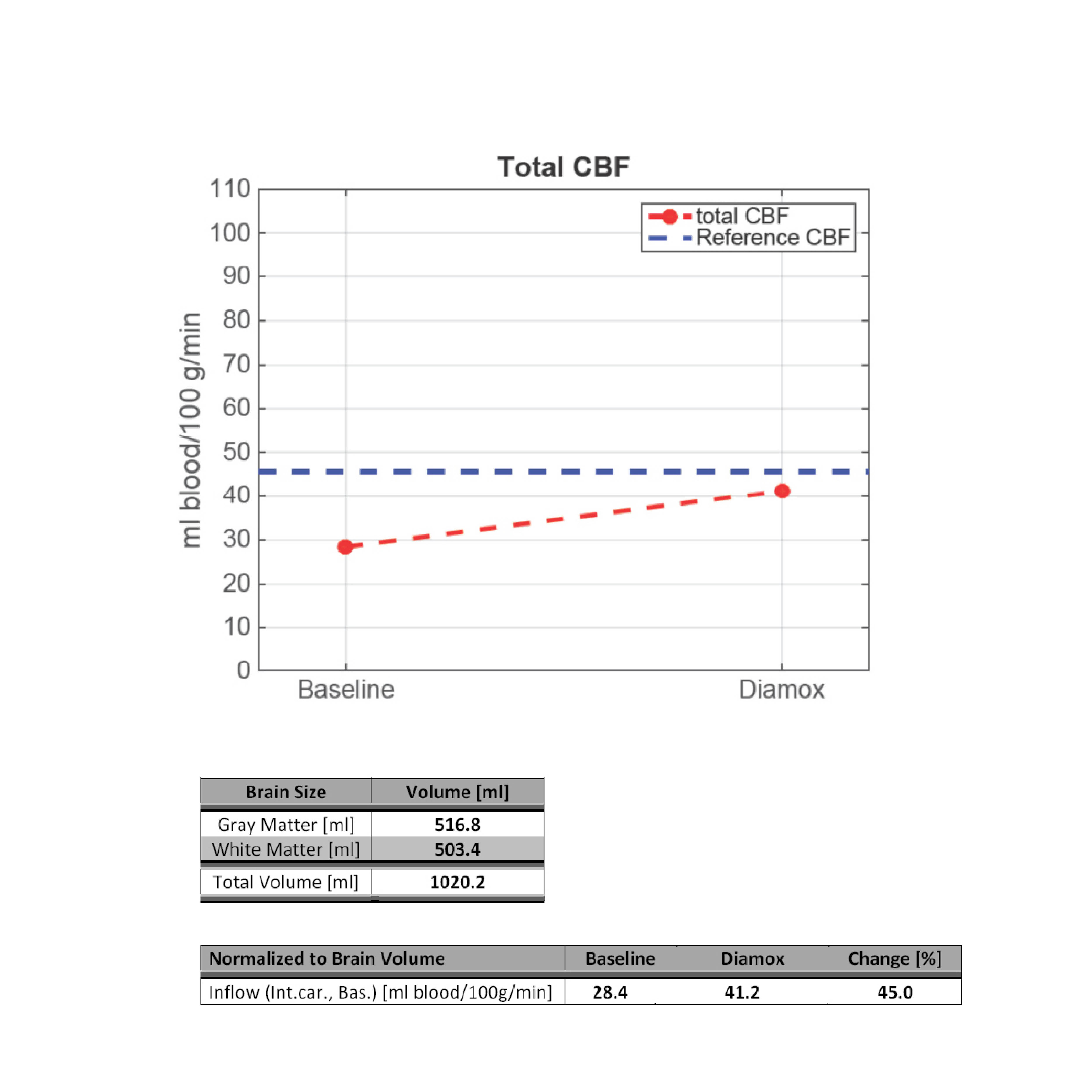
Figure1. Total flow to the brain before and
after Diamox
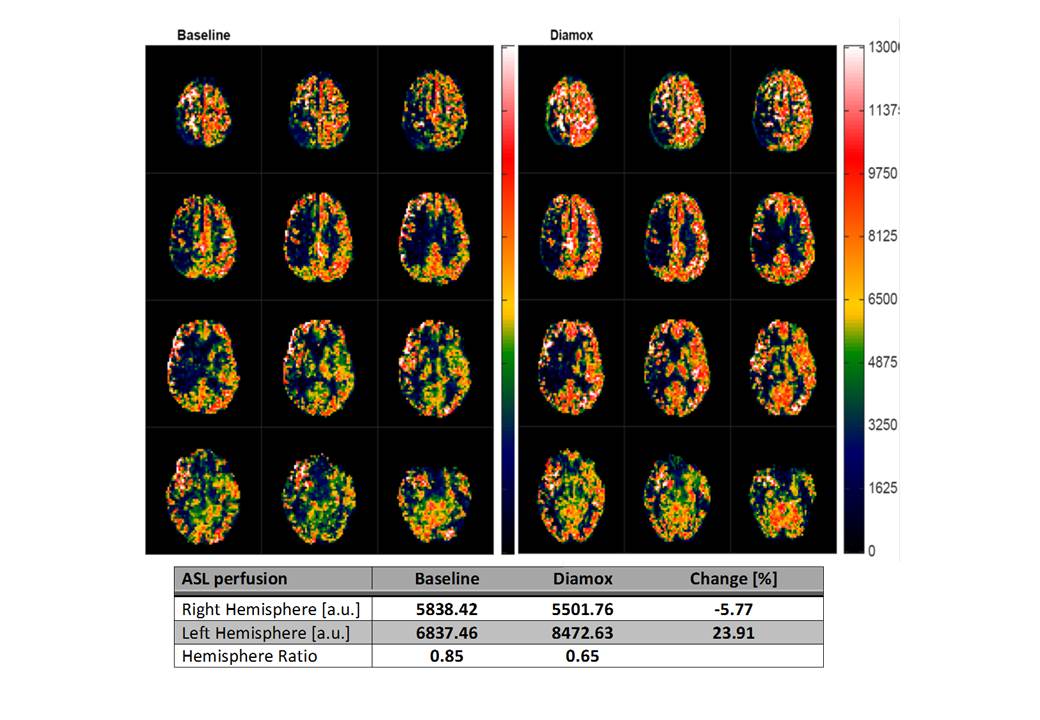
Figure2. ASL before and after Diamox
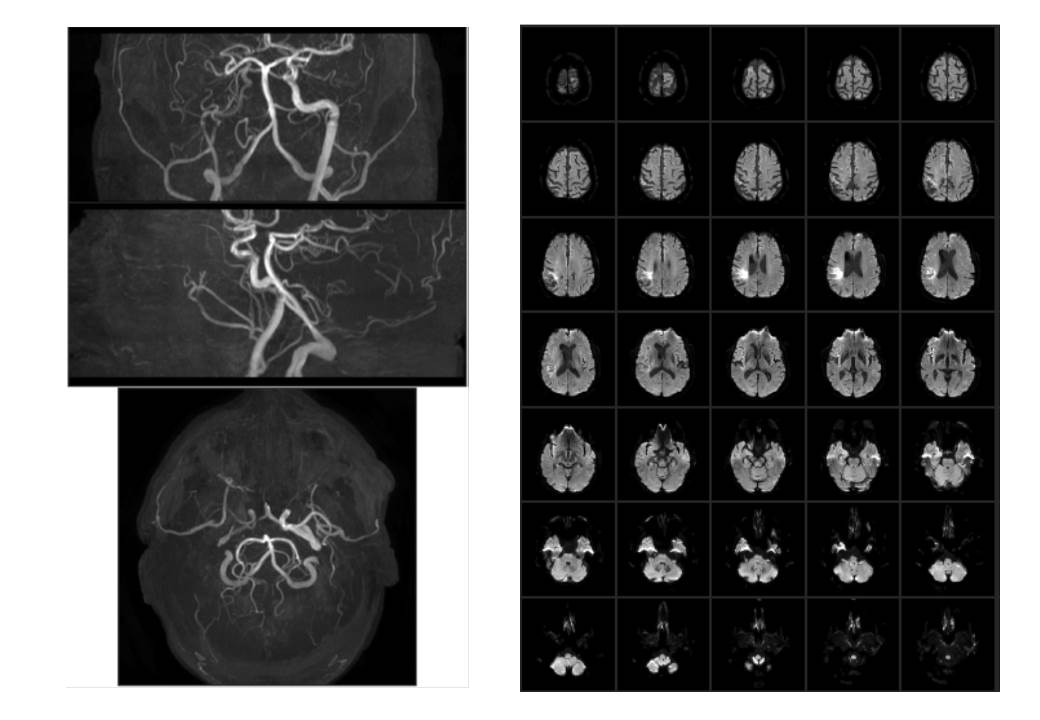
Figure3.MRA and DWI