S12
Advances in Neonatal Brain MRI: 1.5T to 3T1Singapore General Hospital, Singapore, Singapore
Synopsis
Advances of neonatal brain imaging from 1.5T to 3T is beneficial as the additional signal gained from a greater magnetic field strength can be translated into higher spatial resolution and shorter acquisition time. This improves the depiction of intracranial structures and abnormality, hence better clinical outcome can be achieved. Nevertheless, the pitfalls with greater magnetic field strength need to be addressed to reap the benefit of higher magnetic field strength.
Background
Moving neonatal brain imaging from 1.5T to 3T is beneficial as the additional signal intensity offered by higher field strength can be translated to higher spatial resolution and shorter acquisition time. This is crucial in neonatal imaging as it reduces the dependence of sedative drugs to reduce motion artifacts. By convention, neonatal brain imaging is routinely performed using lower field strength in our institution as the biological effects of greater magnetic field strength on a developing brain is unknown(1).Neonatal imaging in 3T is adopted in our institution upon the release of guidelines by the Food Drug Administration (FDA)(2). This is timely as the demand for neonatal brain imaging has increased exponentially in numbers and complexity. We would like to showcase the optimization of our standard neonatal brain imaging protocol, the pitfalls and the remedy in 3T. The presentation will be supplement with images acquired with 1.5T and 3T scanner.
Teaching Point
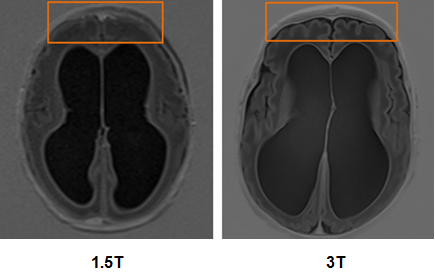
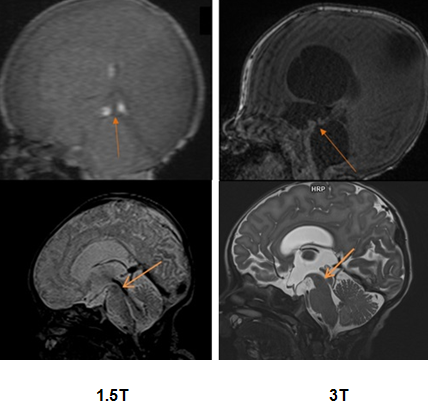
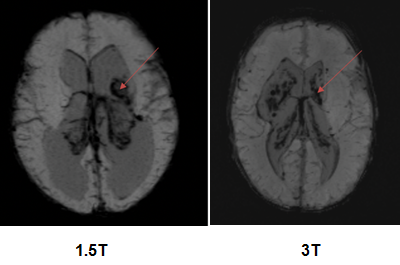
1. Higher spatial resolution in 3T improves the visualisation of the neonatal brain, especially in the differentiation of grey white matter and the depiction of minute cerebral aqueduct (Figure 1 and Figure 2).2. Increased susceptibility artifact associated with shorter T2* in 3T is useful where brain region with haemorrhage will be easier to identify due to intensified hypointensity. This is apparent in susceptibility-weighted imaging (SWI), a technique that is sensitive in detecting susceptibility differences between blood products and adjacent tissue(3).
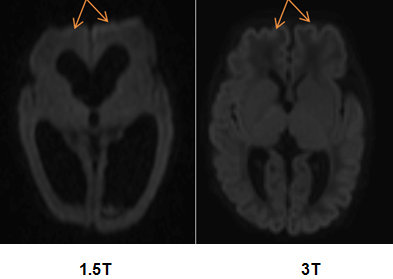
3. The inherent distortion of single-shot diffusion-weighted imaging (DWI) in 3T is remedied by utilizing a readout-segmented eco-planar imaging (RESOLVE-EPI) sequence (Figure 4). The acquisition time of RESOLVE-EPI in 3T is much shorter than that in 1.5T due to the additional SNR.
Conclusion
Neonatal brain imaging in 3T should be the standard moving forward, given the improvement in visualization of intracranial anatomical details and grey and white matter differentiation. An increase in susceptibility artifact is beneficial in SWI whereas distortion artifact in single-shot EPI can be overcome by using RESOLVE-EPI. Nevertheless, further optimisation in imaging sequences is still needed. Imaging of the neonatal brain in 3T set the tone for more advance scan sequences such as functional imaging, diffusion tractography, and spectroscopy.Acknowledgements
No acknowledgement found.References
1. Schenck JF. Safety of Strong, Static Magnetic Fields. In: Ordidge RJ, Kanal E, Shellock FG, editors. New York: John Wiley & Sons, Inc.; 2000. p. 2-19.
2. FDA. Center for Devices and Radiological Health Criteria for Significant Risk Investigations of Magnetic Resonance Diagnostic Devices - Guidance for Industry and Food and Drug Administration Staff. 2014.
3. Deistung A, Mentzel H-J, Rauscher A, Witoszynskyj S, Kaiser WA, Reichenbach JR. Demonstration of paramagnetic and diamagnetic cerebral lesions by using susceptibility weighted phase imaging (SWI). Zeitschrift fuer Medizinische Physik. 2006;16(4):261-7.
Figures