Using Novel Fat Water Separation Sequence to Quantify Intramyocardial Fat-Fraction
1Translational Research Institute, Woolloongabba, Australia, 2Queensland University of Technology, Brisbane, Australia, 3Princess Alexandra Hospital, Woolloongabba, Australia
Synopsis
VARPRO is a novel fat water separation sequence that shows promise for myocardial lipid characterisation. Two questions were addressed in this study: 1. Does VARPRO provide the same myocardial fat-fraction result compared to established magnetic resonance spectroscopy (MRS)? 2. Is the myocardial fat-fraction obtained by VARPRO reproducible? The results suggest the two methods are strongly associated but agreed poorly. The VARPRO estimation is proportionally biased, however, the bias can be easily accounted for using a linear equation. The temporal reproducibility of VARPRO is satisfactory. VARPRO could be a potential, alternative modality to MRS in myocardial lipid quantification.
Introduction
Myocardial steatosis increases the risk of developing heart failure, even in the absence of ischaemia (1-3). Monitoring the myocardial fat-fraction could improve the understanding of cardiac metabolism, and provide a potential risk assessment for patients. Proton magnetic resonance spectroscopy (MRS) is the only non-invasive technique that provides an evaluation of the intramyocardial lipid content (4). Yet, the application of MRS is limited clinically due to technical and practical constraints (3, 4). A novel pulse sequence to provide robust water/fat separation has now been developed based on multi-echo Dixon acquisitions with iterative variable projection estimation (VARPRO, Work-in-progress#724C, Siemens). The images are reconstructed using graph-cut algorithm (5, 6). VARPRO produces water, fat, and T2*maps simultaneously in a single breath-hold. It shows promise as a simple and efficient alternative to MRS for myocardial lipid characterisation. The objectives of this study were: 1, to compare the accuracy of myocardial lipid evaluation using VARPRO and established MRS; 2, to evaluate the reproducibility of using VARPRO to characterise myocardial fat-fraction.Methods
Research subjectsInstitutional ethics approval and written informed consent were obtained. Two cohorts of participants were recruited to evaluate the accuracy and reproducibility respectively. Cohort 1 comprised thirty healthy volunteers (n=30; F=9; mean age=37.5±10.5 years; mean BMI=24.9±3.2 kg/m2); cohort 2 comprised sixteen participants with type 2 diabetes (n=16; F=6; mean age=57.6±10.6 years; mean BMI=36.2±3.5 kg/m2; mean HbA1c= 66.2±12.3 mmol/mol).
Study protocol
Cohort 1 underwent MRI examination on a 60cm 3.0T MRI system (Prisma, Siemens AG, Erlangen, Germany) using two 30-channel flex array. VARPRO was acquired in the left ventricle (LV) short-axis planes in the basal, mid, and apical positions. Respiratory and ECG-gated proton point resolved spectroscopy (PRESS) was acquired with and without water suppression. The voxel was placed on the interventricular septum at end-diastole. Cohort 2 were examined twice on a 70cm 3.0T MRI system (Skyra, Siemens AG, Erlangen, Germany), using a 30-channel flex anterior array combined with the spinal array. VARPRO was acquired after eight hours of fasting. At the time of rescanning, cohort 2 had mean BMI and HbA1c of 36.7±4.0kg/m2 and 62.5±14.2mmol/mol respectively. The mean inter-scan interval was 7.4 months.
Data collection
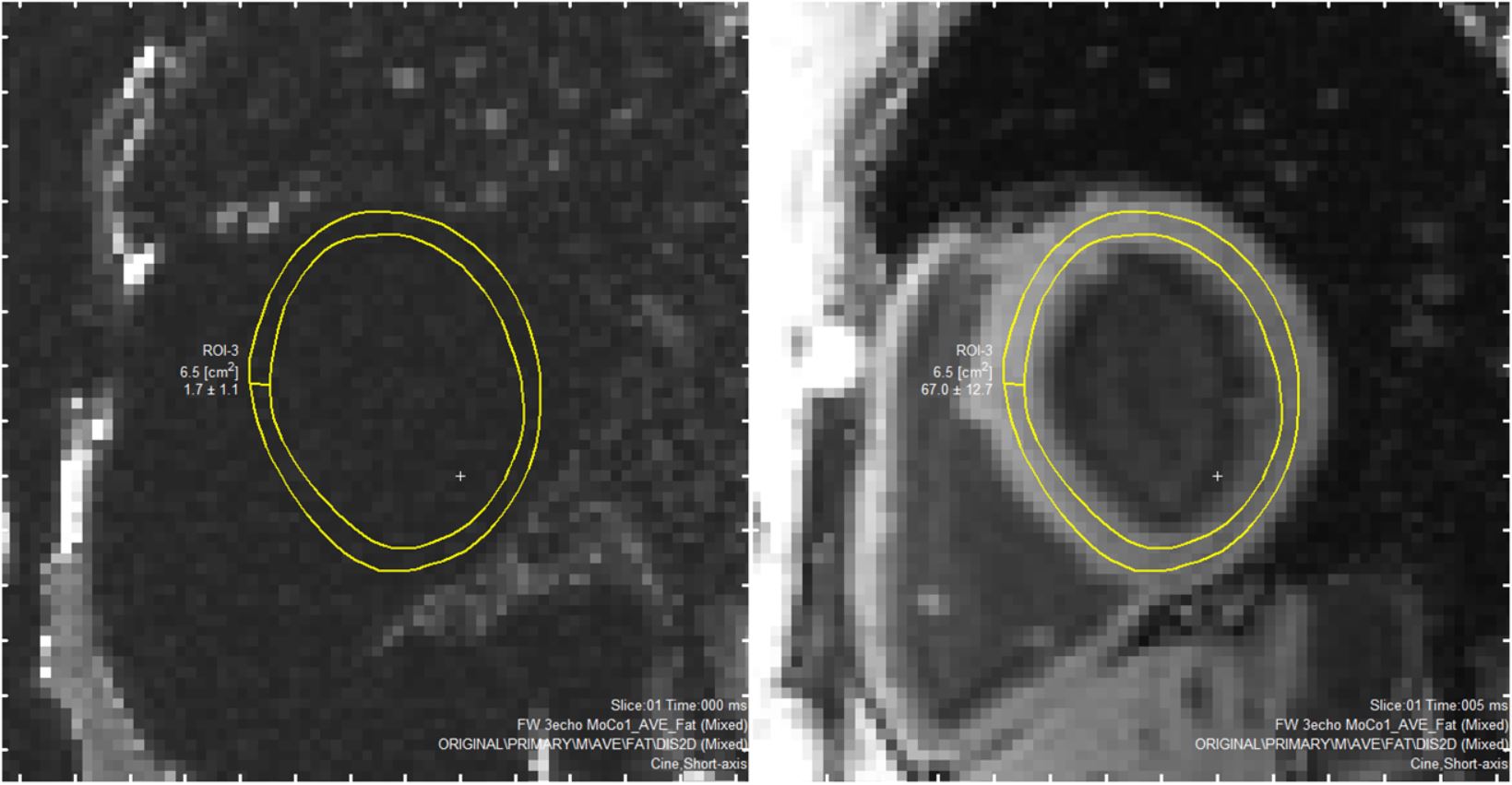
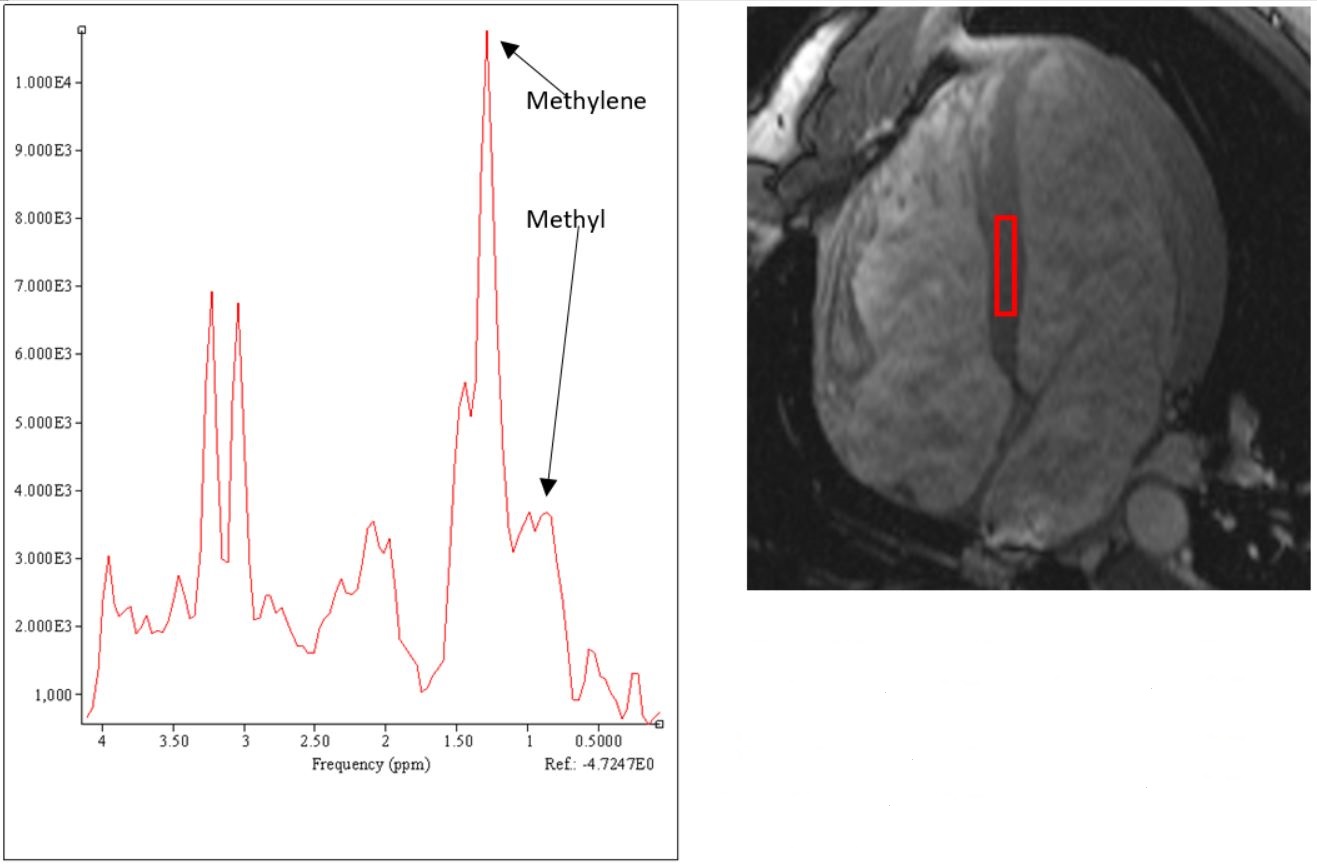
Segment (v2.2 R6190, Medviso, Lund, Sweden) was used for image analysis. Images with apparent artefacts were rejected. The regions of interest (ROIs) were placed within manually segmented myocardia with a further 20% erosion in both endo- and epicardial directions (Figure 1). Basal and mid-cavity fat-fractions were averaged to achieve VARPRO fat-fraction. Myocardial spectra were analysed using Java-based magnetic resonance user interface (jMRUI, V6.0, Leuven, Belgium). Advanced method for accurate, robust and efficient spectral (AMARES) fitting of MRS data was used to quantify the amplitude of water and lipid signals. Intramyocardial lipid was recorded as the sum of methyl and methylene resonances at 0.9 and 1.3 ppm (Figure 2).
Statistical analysis
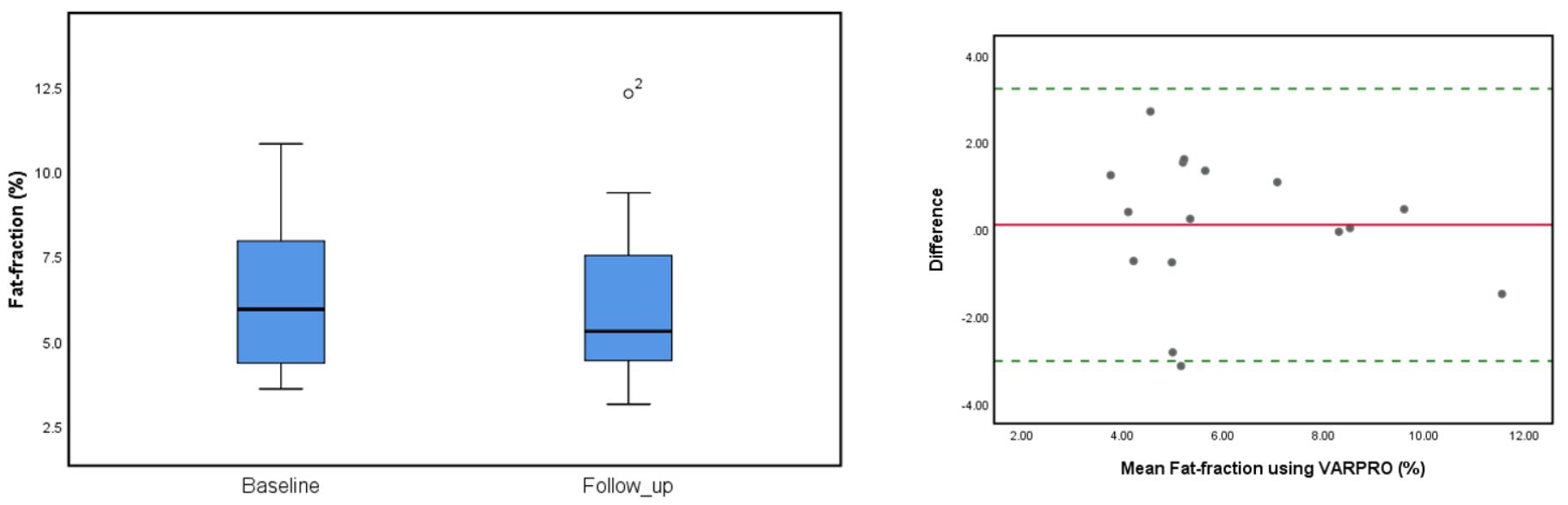
Paired t-test and Pearson correlation tests were used to assess the relationship between the fat-fractions obtained by the two methods. A sub-group of cohort 1 (n=20) were randomly selected to develop a linear adjustment equation, and this was validated in the remaining 10 participants. The agreement between adjusted VARPRO and MRS fat-fraction was tested using Bland and Altman method (7) which was also used to assess temporal reproducibility in the repeated VARPRO measurements on cohort 2.
Results
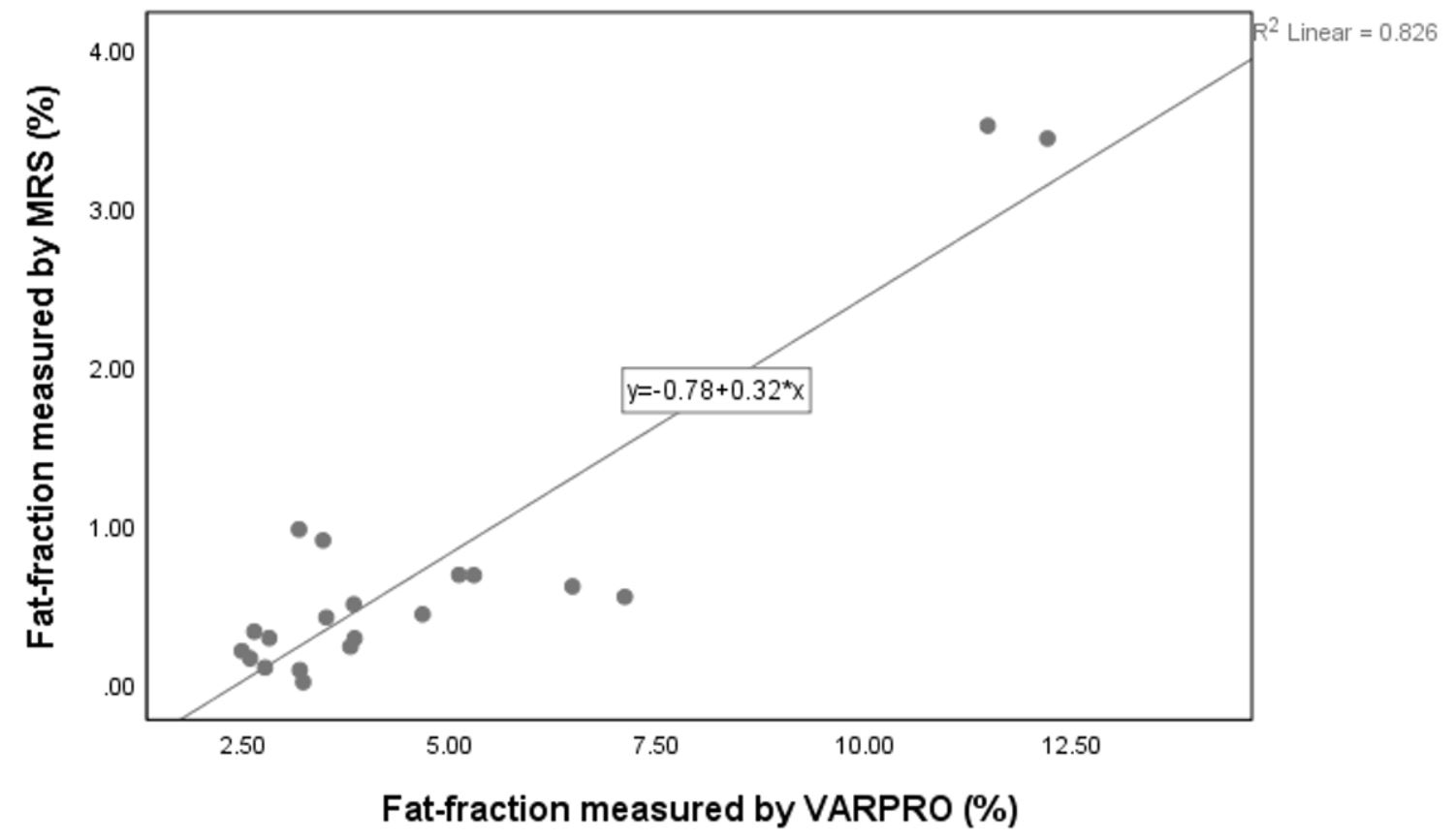
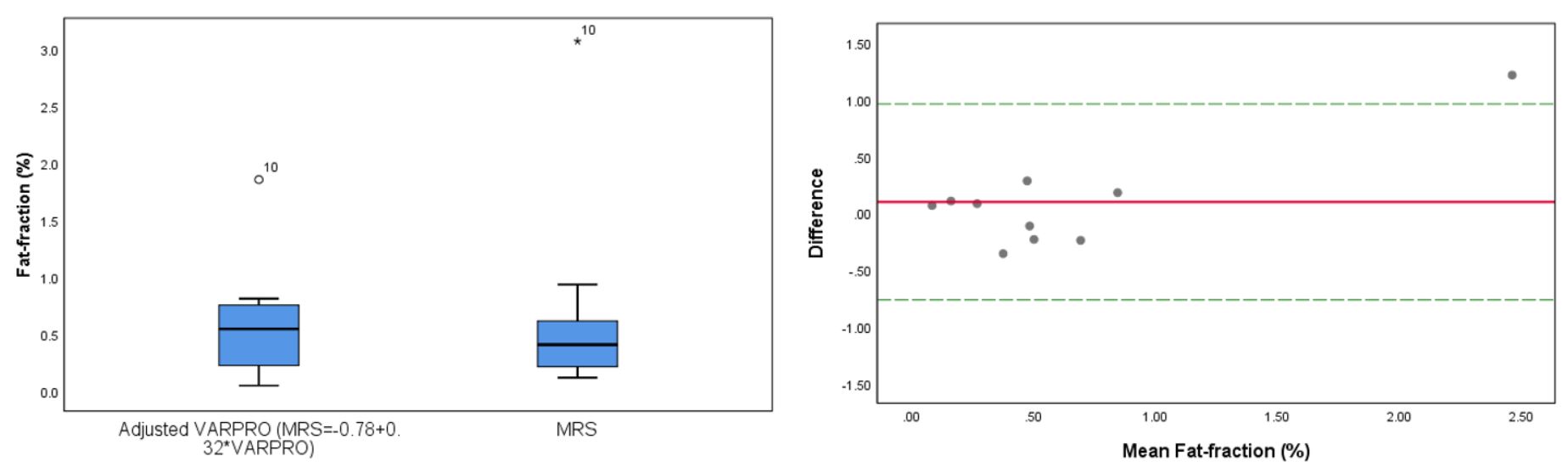
There was a strong linear association (r=0.897, P<0.001) between myocardial lipid concentration obtained by VARPRO and MRS. However, the numerical values of the two methods are significantly different (p<0.001), suggesting poor agreement; therefore, VARPRO values were adjusted according to the linear regression equation obtained from a derivation set ( $$$MRS=-0.78+0.32*VARPRO$$$ ) (Figure 3). Adjusted VARPRO was compared to MRS in a validation set, with good concordance (11% mean variation) (Figure 4). Our results also showed VARPRO exhibits good temporal reproducibility with the coefficient of repeatability of 3.18 (Figure 5).Discussion
Using VARPRO to quantify fat-fraction is achieved by directly measuring mean signal intensity on water-only and fat-only images. Thus, the accuracy is susceptible to thermal noise and other image artefacts, which could explain why lipid concentrations determined by VARPRO are consistently higher than those measured using MRS. However, this bias is non-differential, and can easily be adjusted using linear models. Moreover, the high reproducibility of VARPRO makes it an ideal method for longitudinal studies. Finally, VARPRO does not require lengthy scan times or special technical expertise. This makes the investigation of metabolic heart disease less burdensome clinically. The research has some limitations. Firstly, the overall sample size is small. Secondly, as the accuracy-test was conducted on healthy volunteers, the full spectrum of myocardial steatosis have not been studied. Thirdly, the test re-test variability was sampled, on average, 7.4 months apart. Although there was no significant changes in BMI or HbA1c, interval change might still be a confounder.Conclusions
VARPRO is a potential, alternative modality to MRS in myocardial lipid quantification. It is less susceptible to technical disadvantages. Patient tolerance is markedly better compared to MRS. VARPRO can be easily incorporated into the routine clinical protocol, making a non-invasive assessment of cardiac metabolism possible. Further studies on larger and diverse groups of participants could help evaluate the performance of VARPRO, covering the full spectrum (moderate to severe) of cardiac steatosis.Acknowledgements
No acknowledgement found.References
1. Ng AC, Delgado V, Djaberi R, Schuijf JD, Boogers MJ, Auger D, et al. Multimodality imaging in diabetic heart disease. Curr Probl Cardiol. 2011;36(1):9-47.
2. Graner M, Pentikainen MO, Nyman K, Siren R, Lundbom J, Hakkarainen A. Cardiac steatosis in patients with dilated cardiomyopathy. Heart. 2014;100.
3. Faller KM, Lygate CA, Neubauer S, Schneider JE. 1 H-MR spectroscopy for analysis of cardiac lipid and creatine metabolism. Heart failure reviews. 2013;18(5):657-68.
4. Weiss K, Martini N, Boesiger P, Kozerke S. Cardiac proton spectroscopy using large coil arrays. NMR in Biomedicine. 2013;26(3):276-84.
5. Hernando D, Kellman P, Haldar J, Liang ZP. Robust water/fat separation in the presence of large field inhomogeneities using a graph cut algorithm. Magnetic Resonance in Medicine: An Official Journal of the International Society for Magnetic Resonance in Medicine. 2010;63(1):79-90.
6. Hernando D, Haldar J, Sutton B, Ma J, Kellman P, Liang ZP. Joint estimation of water/fat images and field inhomogeneity map. Magnetic Resonance in Medicine: An Official Journal of the International Society for Magnetic Resonance in Medicine. 2008;59(3):571-80.
7. Bland JM, Altman DG. Statistical methods for assessing agreement between two methods of clinical measurement. Lancet. 1986;1.
Figures