Endometrial Cancer & Other Uterine Malignancies
1Diagnostic Imaging Department, Cancer Institute Hospital of Japanese Foundation for Cancer Research, Tokyo, Japan
Synopsis
Diagnosing local extension of the endometrial carcinoma with MR is crucial as myometrial and cervical stromal invasion are important prognostic factors. However, the utility of T2-weighted, contrast-enhanced, and diffusion-weighted images is controversial. In this lecture, oncologically essential facts and tips of the MR in diagnosing endometrial carcinoma will be presented. Leiomyosarcoma is the most common malignant mesenchymal tumor of the uterus; however, it is still difficult to differentiate it from uterine fibroids. We will provide MR findings of leiomyosarcoma comparing to those of histological variants of uterine fibroid and cutting edge technology in differentiating these two disease entities.
Endometrial Carcinoma
Tumors affecting uterine corpus is divided into the epithelial, mixed epithelial and mesenchymal and mesenchymal origin. Endometrial carcinoma is the most common malignancy among them, and about 60000 female has affected annually in the U.S. The staging system established by FIGO is widely used that is originally determined after surgery. However, pre-operative diagnosis affects the treatment option, and imaging diagnosis is as important as those in other gynecological malignancies. In general, the local extension of the endometrial carcinoma is diagnosed with MR, and CT or FDG-PET-CT is widely used for distant metastasis. There is so much evidence MR can provide accurate myometrial invasion, which is closely related to the lymph nodes metastasis and outcomes, including dynamic contrast enhancement (DCE) and diffusion-weighted images (DWI). However, diagnostic radiologists should know the biological behavior of the diseases, factors affect patients' outcomes and treatment options before diagnosing with MR. In this lecture, the oncologic background of the endometrial carcinoma and pearls and pitfalls while staging this disease with MR will be provided:- Oncologic background
- Type I and Type II endometrial carcinoma
- Risk stratification of the diseases
- Controversial surgical procedure
- When can we omit lymph node dissection?
- When do we need a radical hysterectomy?
- When can we select fertility-preserving treatment?
- Pears and pitfalls in diagnosing endometrial carcinoma with MR
- Predicting the histological diagnosis of the endometrial lesion on MR
- Staging endometrial carcinoma
- Myometrial invasion-T2-weighted images (T2WI), DCE, DWI
- Cervical invasion
- Adnexal extension
- Intraperitoneal dissemination
Uterine sarcoma
Another important topic of uterine malignancies is differentiating uterine sarcomas and fibroids. Fibroids, leiomyomas, in other words, can show variable faces on MR due to degeneration and histological variants that mimic uterine sarcomas. Carcinosarcoma, classified into mixed epithelial and mesenchymal tumors, is now considered as evolving from a carcinoma. So the disease will be discussed in the part of endometrial carcinoma. We will discuss the following topics concerning with MR diagnosis of the uterine sarcomas with typical MR findings.- Histological variants and degeneration of the uterine leiomyomas
- Recent advances in differentiating uterine sarcomas from fibroids
- Classical T1-, T2-weighted images, and contrast-enhanced T1WI including DCE
- DWI
- Texture analysis and radiomics
Acknowledgements
No acknowledgement found.References
- Zaino R et al: Tumours of uterine corpus, (in): Kurman RJ, Carcangiu ML, Herrington S et al. ed eds; WHO classification of Tumours of Female Reproductive Organs. p121-154, IARC Press, Lyon, 2014
- Zaino RJ: FIGO staging of endometrial adenocarcinoma: a critical review and proposal. Int J Gynecol Pathol 28: 1-9, 2009
- Morice P et al: Endometrial cancer. Lancet 387: 1094-1108, 2016
- Vargas R et al: Tumor size, depth of invasion, and histologic grade as prognostic factors of lymph node involvement in endometrial cancer: a SEER analysis. Gynecol Oncol 133: 216-220, 2014
- Nougaret S et al: Endometrial Cancer MRI staging: Updated Guidelines of the European Society of Urogenital Radiology. European Radiology 2018
- Andreano A et al: MR diffusion imaging for preoperative staging of myometrial invasion in patients with endometrial cancer: a systematic review and meta-analysis. Eur Radiol 24: 1327-1338, 2014
- Lin G et al: Endometrial cancer with cervical stromal invasion: diagnostic accuracy of diffusion-weighted and dynamic contrast enhanced MR imaging at 3T. Eur Radiol 27: 1867-1876, 2017
- Bell SW et al: Problematic uterine smooth muscle neoplasms. A clinicopathologic study of 213 cases. Am J Surg Pathol 18: 535-558, 1994
- Tanaka YO et al: Smooth muscle tumors of uncertain malignant potential and leiomyosarcomas of the uterus: MR findings. J Magn Reson Imaging 20: 998-1007., 2004
- Lakhman Y et al: Differentiation of Uterine Leiomyosarcoma from Atypical Leiomyoma: Diagnostic Accuracy of Qualitative MR Imaging Features and Feasibility of Texture Analysis. Eur Radiol 27: 2903-2915, 2017
Figures

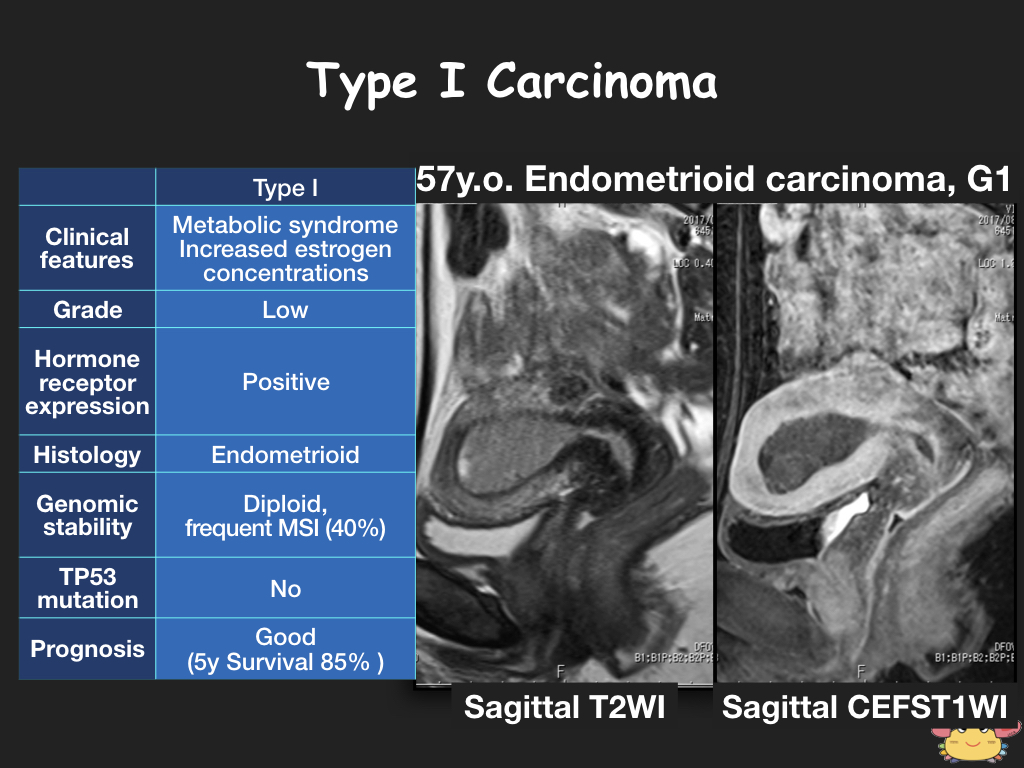
Type I endometrial carcinoma
Bokhman et al. divided endometrial carcinoma into type I and II. Type I carcinoma is usually indolent and tends to show exophytic extension MR.
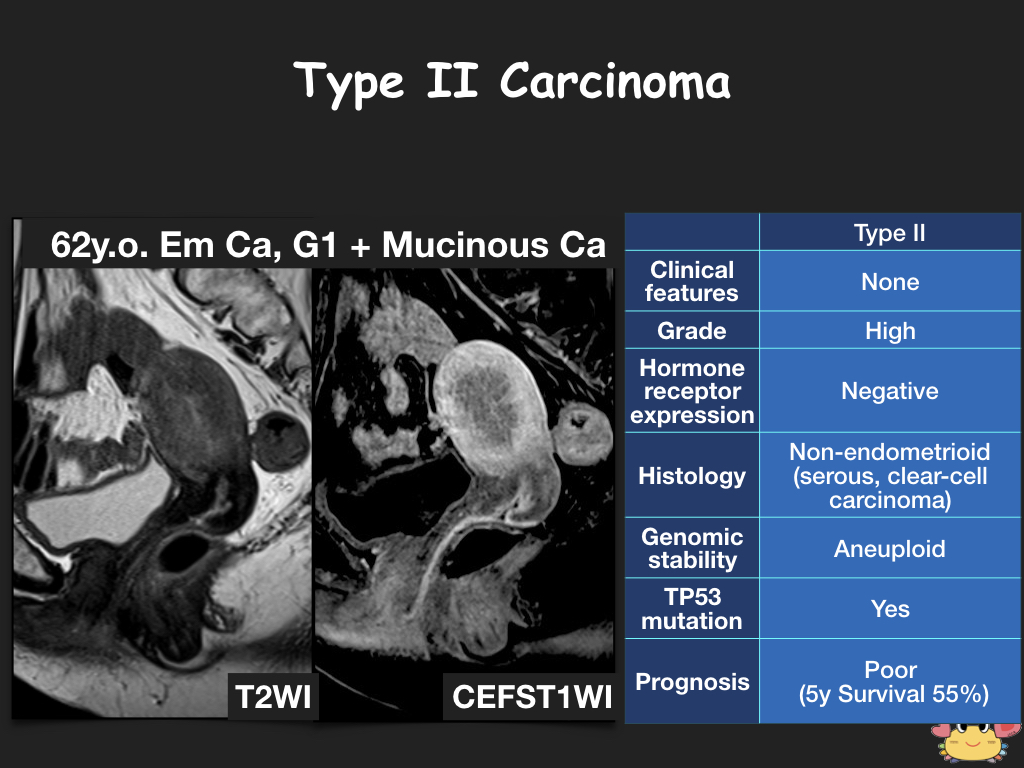
Type II endometrial carcinoma
Bokhman et al. divided endometrial carcinoma into type I and II. Type II carcinoma is usually aggressive and tends to show endophytic extension MR.
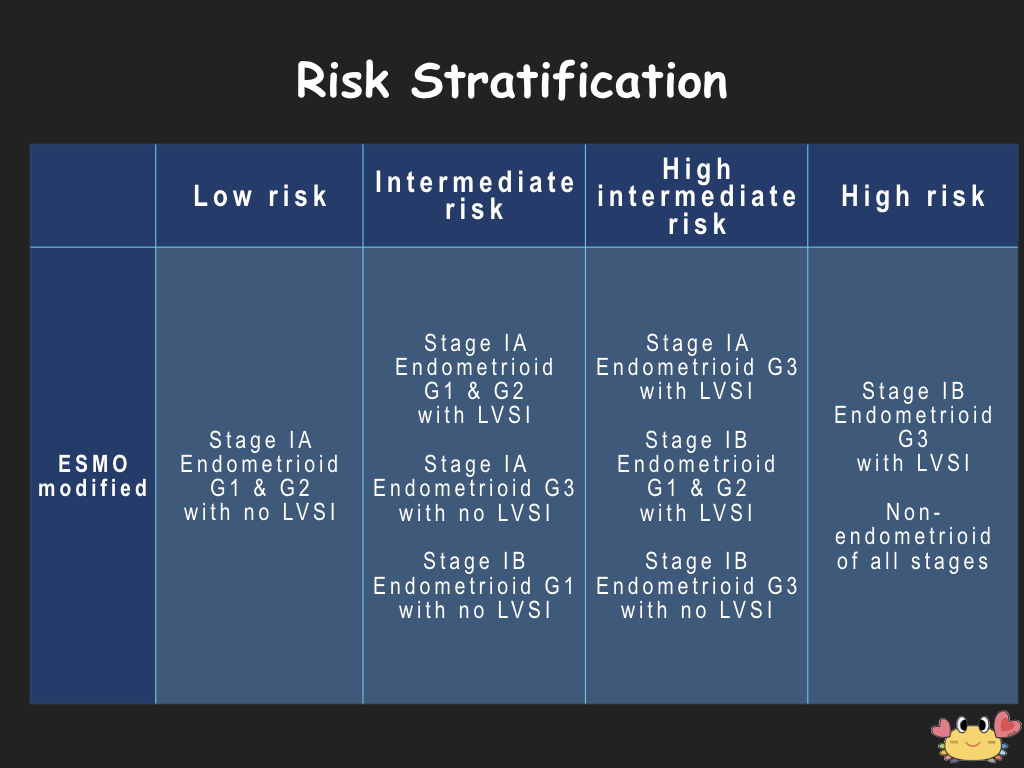
Risk stratification established by ESMO (European Society for Medical Oncology)
There are several risk stratification established by societies, and ESMO's is the most accepted one. All of them value the myometrial invasion, which can be diagnosed with MR.
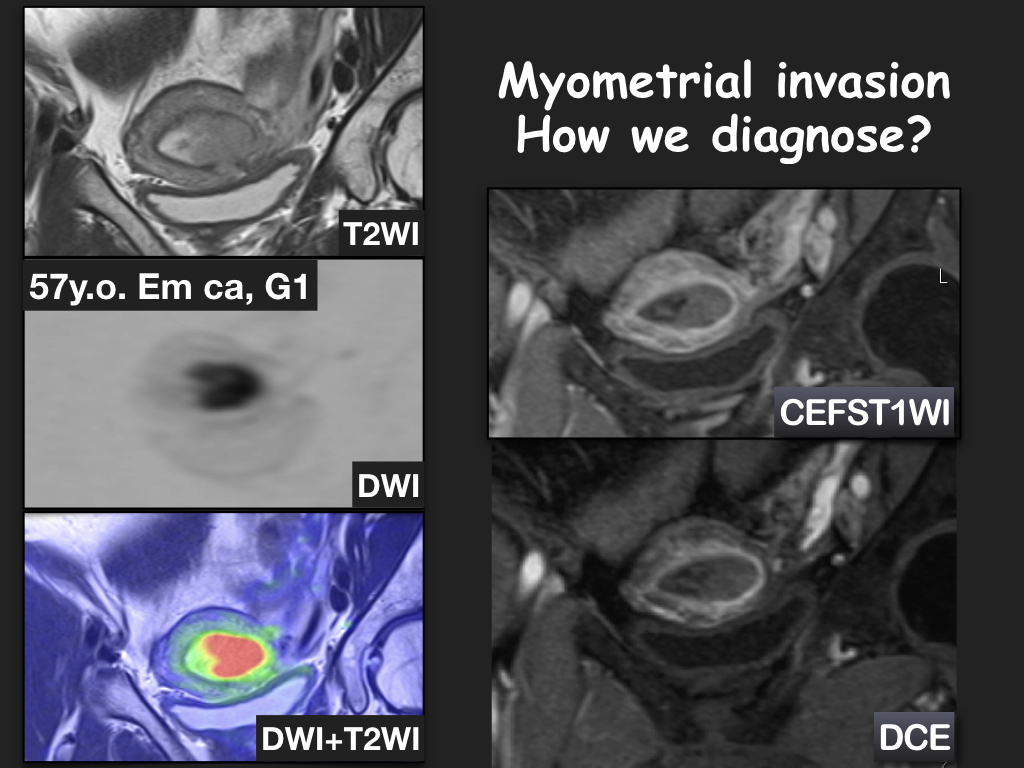
How to diagnose myometrial invasion of the endometrial carcinoma on MR
There are many sequences in diagnosing myometrial invasion with MR. Each method has advantages and disadvantages.