4870
IVIM & Diffusion Kurtosis MR Imaging on Interim Response Assessment of Hodgkin Lymphoma
Archana Vadiraj Malagi1, Devasenathipathy Kandasamy2, Kedar Khare3, Deepam Pushpam4, Rakesh Kumar5, Sameer Bakhshi4, and Amit Mehndiratta1,6
1Centre for Biomedical Engineering, Indian Institute of Technology Delhi, New Delhi, India, 2Department of Radiodiagnosis, All India Institute of Medical Sciences Delhi, New Delhi, India, 3Indian Institute of Technology Delhi, New Delhi, India, 4Department of Medical Oncology, Dr. B.R. Ambedkar Institute-Rotary Cancer Hospital (IRCH), All India Institute of Medical Sciences Delhi, New Delhi, India, 5Department of Nuclear Medicine, All India Institute of Medical Sciences Delhi, New Delhi, India, 6Department of Biomedical Engineering, All India Institute of Medical Sciences Delhi, New Delhi, India
1Centre for Biomedical Engineering, Indian Institute of Technology Delhi, New Delhi, India, 2Department of Radiodiagnosis, All India Institute of Medical Sciences Delhi, New Delhi, India, 3Indian Institute of Technology Delhi, New Delhi, India, 4Department of Medical Oncology, Dr. B.R. Ambedkar Institute-Rotary Cancer Hospital (IRCH), All India Institute of Medical Sciences Delhi, New Delhi, India, 5Department of Nuclear Medicine, All India Institute of Medical Sciences Delhi, New Delhi, India, 6Department of Biomedical Engineering, All India Institute of Medical Sciences Delhi, New Delhi, India
Synopsis
PET/CT plays an important role in assessment of treatment response in Hodgkin lymphoma (HL). This study goal was to evaluate the role of IVIM and DKI parameters role in interim assessment of HL. ADC, D(BE+TV), Dk and f showed reduction in interim which was in accordance with changes of SUVmax and SUVmean whereas D* and k showed increase against treatment response. In future, IVIM and DKI can have the potential in accurate assessment of interim monitoring in HL.
Introduction
Accurate chemotherapy monitoring of cancer provides clinically useful information for treatment response and its prognostication. In Hodgkin lymphoma (HL), 18-fluorodeoxyglucose (FDG) Positron Emission Tomography (PET) with CT (PET/CT) is most commonly used for diagnosing, staging and interim monitoring using quantitative parameter such as standard uptake value (SUV)1. However, PET/CT uses ionizing radiation, and radiotracers is sometimes contraindicated in few patients because of associated complications. Non-invasive monitoring can be achieved using Intravoxel incoherent motion (IVIM) and Diffusion kurtosis imaging (DKI) which provides microstructure and macrovascular information of tumor without any contrast injection2,3. Objective of this study was to investigate the role of IVIM and DKI in interim response assessment of HL in comparison with clinical standard, PET imaging.Methods
Patients and Interim assessment: Three patients with Hodgkin lymphoma (n=3; age: 42.33±13.58 years; M:F=1:2) were recruited and underwent biopsy procedure after the ethical approval of Institutional Ethics Board and written informed consent. All patients were treated with standard ABVD (Adriamycin, Bleomycin-sulfate, Vinblastine-sulfate, and Dacarbazine) regime. Interim assessments were done after four cycles of chemotherapies i.e. within 8 weeks.18F-FDG PET/CT acquisition and analysis: PET/CT examinations were performed with a PET/CT scanner (Biograph Mct; Siemens Healthcare,Henkestr,Erlangen,Germany) and Discovery 710 (General electric company, Fairfield, Connecticut, USA). Dosage of 6–11 MBq/kg (0.16–0.18 mCi/kg; minimum, 3 mCi) FDG intravenously injected. After the 45–60-minute uptake period, the patients were taken for the PET/CT study. SUVmax (maximum Standard Uptake Value) and SUVmean were calculated using equation below:
$$SUV=\frac{r}{a'/w}$$
where, r=radioactivity activity concentration (kBq/ml), a′=decay-corrected amount of injected radiolabeled FDG (kBq), and w=weight of the patient (g).
MR acquisition and Analysis: All patients were scanned in 1.5T MRI (Ingenia; Philips Healthcare, Best, the Netherlands) at AIIMS, New Delhi, India, with a STIR (Thoracic:TR=1.503s and TE=0.09s;Abdomen: TR=1.503s and TE=0.06s), including IVIM-DKI with 9b-values= 0,35,50,100,175,300,500,1500,2000 s/mm2 using phased-array surface coil (Thoracic: TR=12.44s, TE=0.081s; Abdomen: TR=12.44s, TE=0.081s) for thoracic and abdominal area.
All parameters were estimated using Non-linear least square optimization based IVIM-DKI model with in-house toolbox using MATLAB. ADC was calculated voxelwise using monoexponential model.
IVIM parameters such as D, D*, and f were evaluated using two methods i) BE model2 and ii) BE with Total variation penalty function (TV)4,5. BE model is defined below2:
$$S⁄S_0=fexp(-bD^* )+(1-f)exp(-bD)$$
where S and S0 are diffusion signals with and without diffusion gradient b in s/mm2. In BE+TV model, image gradient was calculated with parameter values updated iteratively (TV parameters, alpha and beta set to 0.005 and 0.99)5.
DKI parameters such as Dk and k were analyzed using DKI model3:
$$S⁄S_0=exp(-bD_k+b^2D_k^2 K/6)$$
ROI localization: Image DWI at b=2000 s/mm2 (hyperintense), ADC map (hypointense) and PET-SUV maps (hyperintense) were used to localize tumor as shown in Figure1.
Results
Diffusion, Kurtosis and Perfusion-related parameters in Baseline and Interim monitoring of HL: Figure2, circled area shows tumor region appeared hypointense in ADC, Dk D (BE), D (BE+TV) and k map at baseline for a representative patient. After treatment, intensity in tumor region reduced and corresponding changes can be seen in D (BE+TV), Dk, k map distinctly.Figure3 shows D* parameter obtained from BE and BE+TV model, appeared hypointense at baseline as compared to interim assessment whereas f showed opposite trend. D* (BE) at both times showed noisy maps.
Quantitative assessment of IVIM and DKI parameters with PET parameters: Figure4 shows ADC, Dk, D (BE+TV), f (BE) and f (BE+TV) mean values reduced at interim measurement as compared to baseline, same changes were also seen in PET parameters such as SUVmax and SUVmean. Whereas, D* (BE) and D* (BE+TV) with k showed increased mean values at interim assessment. D (BE) showed no changes w.r.t treatment response.
Discussion and Conclusions
IVIM analysis consists of diffusion and perfusion parameter explaining the structural and dynamic information of tissue in the tumor region whereas DKI parameters provides information on tissue heterogeneity. To obtain spatial homogeneity in parameter maps, total variation penalty function was included into BE model to remove any spurious values in maps4,5.Previous literature has shown D, D* and f parameters to be good biomarker for treatment response6-8. In this study, quantitative and qualitative assessment of IVIM and DKI parameters were performed in comparison with PET parameters for patients with HL. Diffusion related parameters such as ADC, Dk, D (BE+TV) showed decreasing trend in chemotherapy interim assessment which is in accordance with PET indicating a positive treatment response9. Kurtosis showed opposite trend with increase during response interim assessment, indicating increase in tissue heterogeneity. Perfusion-related parameters such as f showed reduction and opposite trend was observed with D* for response assessment which is in accordance with literature6-8. However, due to small sample size, no statistical analysis could be performed. Still with a limited dataset this preliminary study showed good evidence to support further exploration of IVIM & DKI in chemotherapy response assessment for Hodgkin Lymphoma and to evaluate if it can be used in place of PET imaging.
Acknowledgements
This study was supported by IIT Delhi and AIIMS Delhi. AVM was supported by research fellowship fund from Ministry of Human Resource Development, Government of India.References
- Kanoun S, Rossi C, Casasnovas O. [18F] FDG-PET/CT in Hodgkin Lymphoma: Current Usefulness and Perspectives. Cancers. 2018;10(5):145.
- Le Bihan D, Breton E, Lallemand D et al. Separation of diffusion and perfusion in intravoxel incoherent motion MR imaging. Radiology. 1988;168(2):497-505.
- Jensen JH, Helpern JA et al. MRI quantification of non‐Gaussian water diffusion by kurtosis analysis. NMR in Biomedicine 2010;23(7):698-710.
- Rudin L I, Osher S & Fatemi E. Nonlinear total variation based noise removal algorithms. Phys. D nonlinear Phenom.1992;60:259–268.
- Kayal E B et al. Quantitative Analysis of Intravoxel Incoherent Motion (IVIM) Diffusion MRI using Total Variation and Huber Penalty Function. Med. Phys. 2017;44:5849–5858.
- Xiao Y, Pan J, Chen Y et al. Intravoxel incoherent motion-magnetic resonance imaging as an early predictor of treatment response to neoadjuvant chemotherapy in locoregionally advanced nasopharyngeal carcinoma. Medicine. 2015;94(24).
- Granata V, Fusco R, Catalano O et al. Early assessment of colorectal cancer patients with liver metastases treated with antiangiogenic drugs: the role of intravoxel incoherent motion in diffusion-weighted imaging. PLoS One. 2015;13:10(11):e0142876..
- Xiao Y, Pan J, Chen Y et al. Intravoxel incoherent motion-magnetic resonance imaging as an early predictor of treatment response to neoadjuvant chemotherapy in locoregionally advanced nasopharyngeal carcinoma. Medicine. 2015;94(24).
- Wu R, Suo ST, Wu LM et al. Assessment of chemotherapy response in non-Hodgkin lymphoma involving the neck utilizing diffusion kurtosis imaging: a preliminary study. Diagnostic and Interventional Radiology. 2017;23(3):245.
Figures
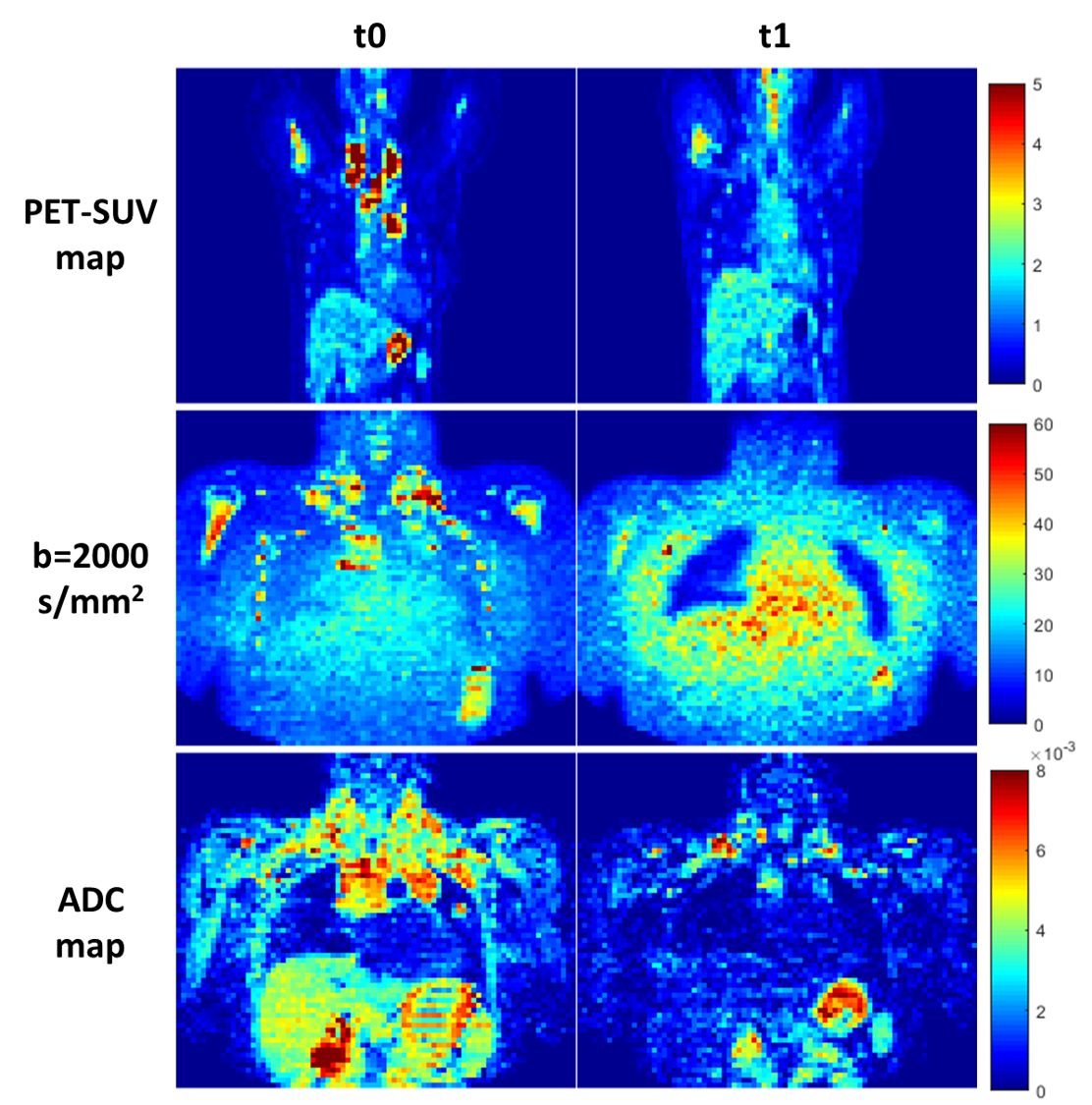
Figure1: ROI
localization of tumor (black circle) using PET-SUV map, IVIM-DKI at b=2000 s/mm2
and ADC map of one representative patient having HL at baseline(t0) and interim
(t1).
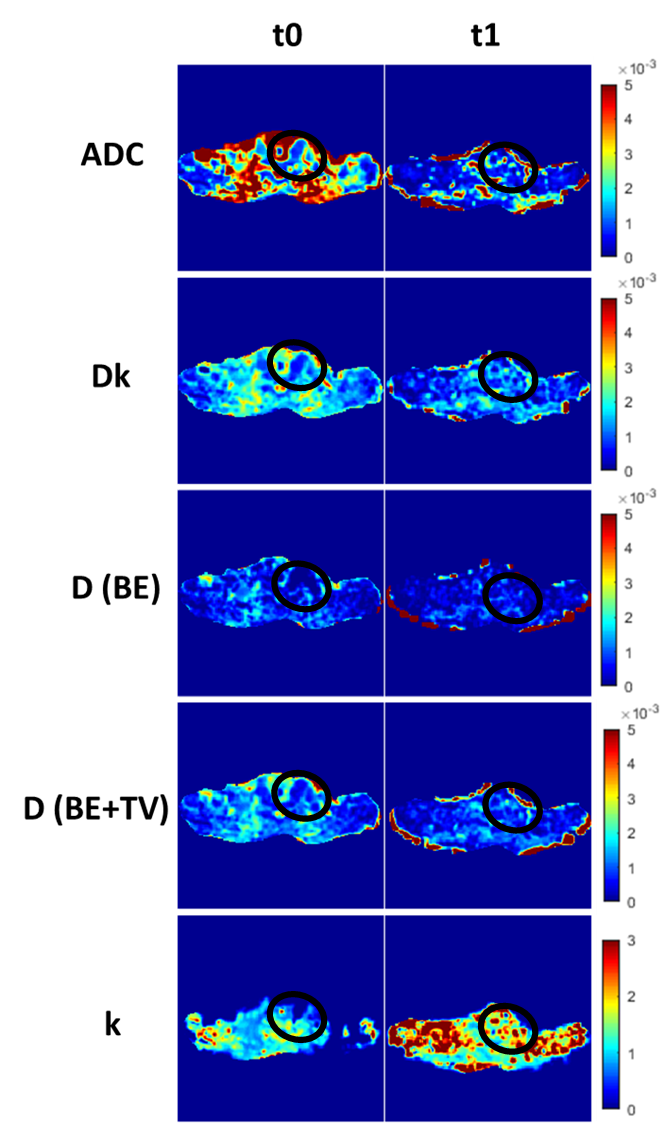
Figure2: Comparison of ADC, IVIM
parameters (D (BE) and D(BE+TV)) and DKI parameters (Dk and k) against Baseline
(t0) and Interim (t1) of one representative patient having HL.
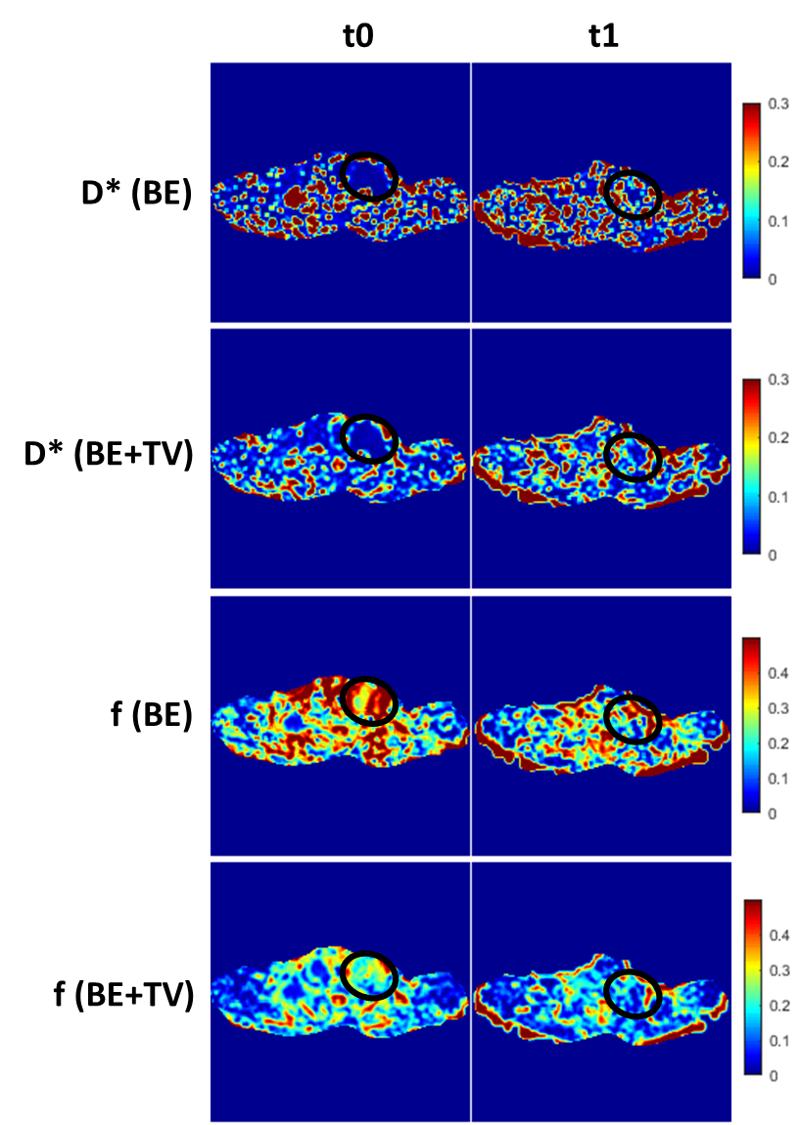
Figure3: Comparison of Perfusion related parameters such as
D* (BE), D* (BE+TV)), f (BE), and f (BE+TV) against Baseline (t0) and Interim (t1) of one representative
patient having HL.
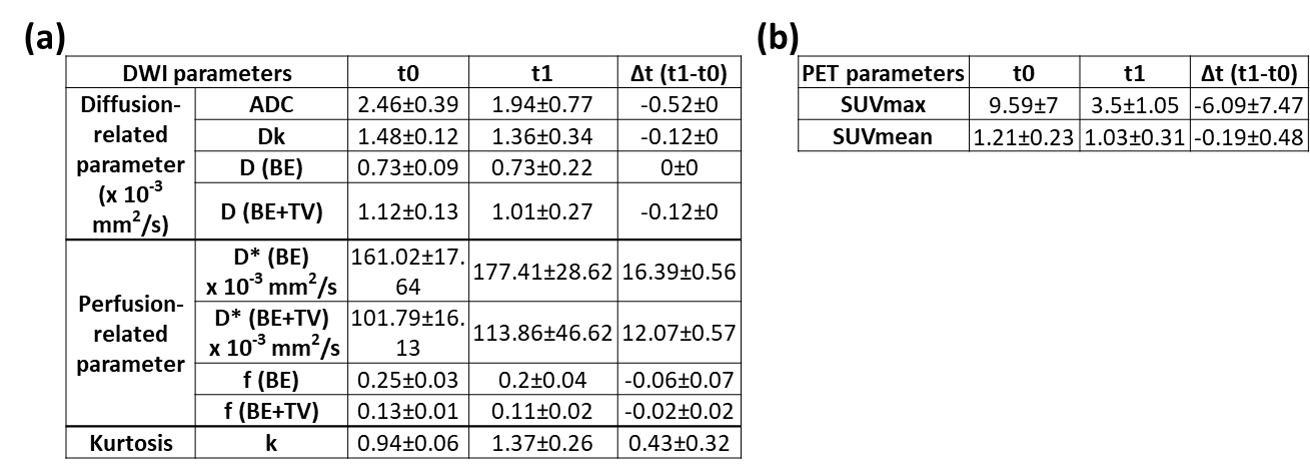
Figure4: Quantitative comparison of
(a) IVIM and DKI parameters, (b) PET parameters at baseline and interim
monitoring of HL