4840
Intrinsically Registered Fat Saturated and Unsaturated T2W Images Using a Keyhole Method1The Christie NHS Foundation Trust, Manchester, United Kingdom, 2Division of Cancer Sciences, The University of Manchester, Manchester, United Kingdom
Synopsis
Fat saturated and unsaturated T2W images of the same anatomy are required for MRI lung radiotherapy treatment planning. A prospective 'keyhole' pulse sequence that produces both image contrasts at full resolution via acquisition of a subset of FS k-space substituted into the non FS k-space was simulated. Simulated FS images with 50% of FS k-space substituted in a cross hair pattern were found to be only slightly inferior to acquired FS images by four clinicians based on scoring for delineation suitability. The prospective pulse sequence would save MR protocol time and improve the patient experience.
Introduction
Lung cancer treatment with the Elekta Unity MR-Linac is in preparation [1,2]. T2 weighting (T2W) is the preferred contrast for MR lung tumour delineation on radiotherapy MR planning scans, however the similar contrast of fat and tumour make identifying mediastinal invasion and some lymph nodes difficult on T2W images, necessitating a second fat-suppressed (FS) image [3]. This adds significant time to the imaging protocol, prolongs patient discomfort during the planning MR in radiotherapy treatment position and necessitates registration of the two datasets in post-processing. We envisage a new technique that acquires the complete non-FS k-space and a subset of FS k-space within one pulse sequence, then reconstructs both images at full resolution using a keyhole k-space approach [4], offering significant time saving during the scan, in post-processing and reduced time in the MR scanner for the patient.Methods
A multi-slice T2W TSE pulse sequence (TR/TE = 5200/102ms, 30x3.5mm slices with matrix 320x320, 1.25x1.25mm pixels) was obtained both with and without spectral fat saturation FS in lung cancer patients as part of Clinical Trial ref NCT03048760 on a 1.5T Aera (Siemens, Erlangen). Re-sampling of the non-FS image data was undertaken to ensure the imaging slices were at the same spatial locations as the FS images. K-space data for each sequence was obtained and a keyhole k-space matrix was created in post-processing using MATLAB (v 2016b, Mathworks, Natick, USA). To create the keyhole, lines of FS k-space were substituted into the complete non-FS k-space sequence in a cross hair pattern, selected because the majority of high pixel values in k-space lie close to the principal axes.The chosen method is susceptible to ringing artefacts generated at the boundary of the substituted k-space lines. This effect was minimised by calculating the mean signal in the middle five lines of k-space in the common frequency encode direction of the FS and non-FS datasets and scaling the non-FS dataset down by the ratio of the means. The resulting keyhole k-space was inverse Fourier transformed into a final synthesized FS image.
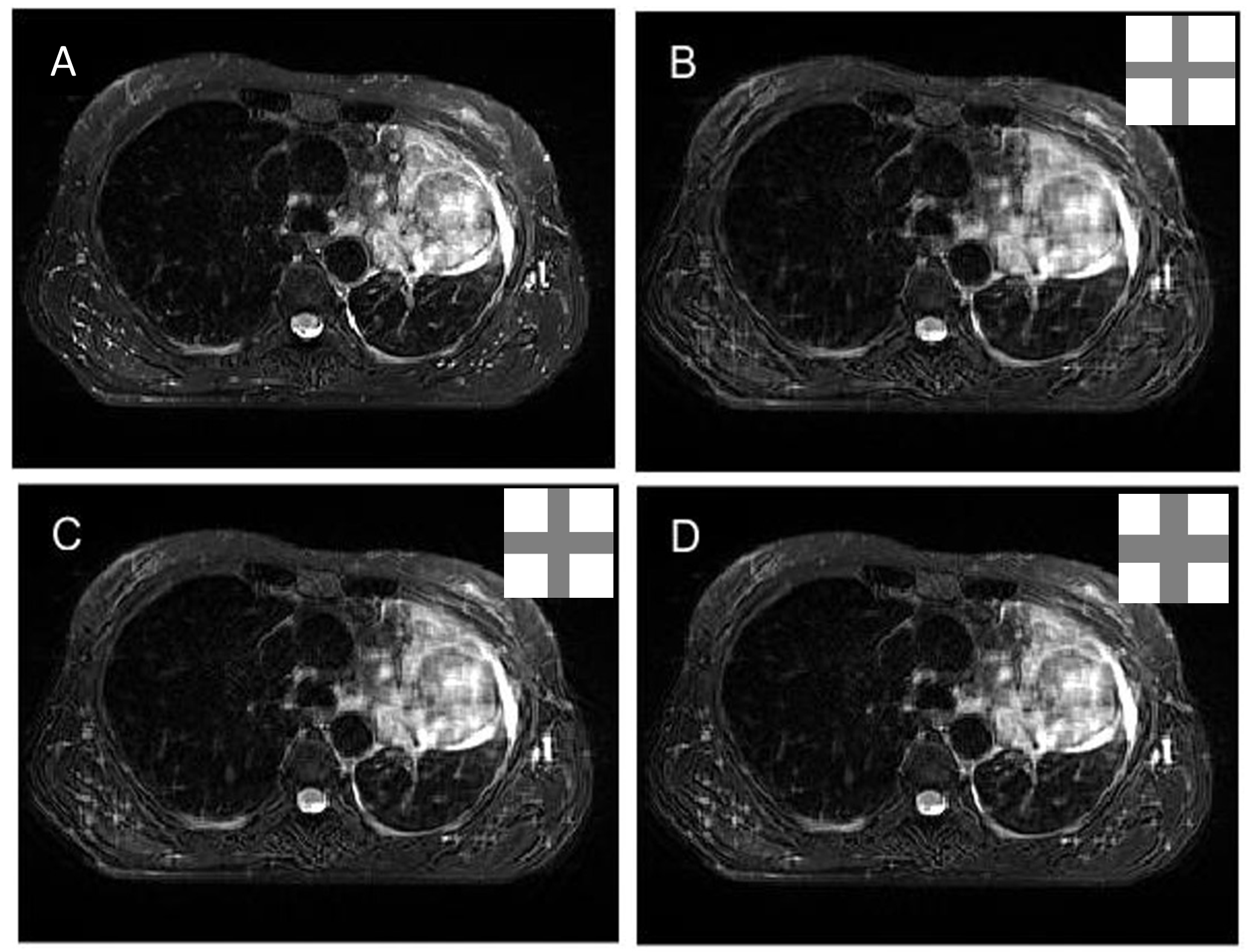
Synthesized FS images with 30, 40 and 50% k-space line replacement were prepared for two slices through the visible tumour for eight patients. 30% replacement meant 15% of k-space lines were replaced in the x-direction and the same number were replaced in the y-direction, with the overlapping centre of k-space averaged as in a radial acquisition (see figure 1 B-D, insets).
To assess the suitability of the synthesized images for delineation 3 lung oncologists and 1 research radiographer were asked to score them on a scale of 0-100, where the traditionally acquired FS image was assigned a reference score of 80. The images for scoring were presented on a 2x2 grid with the reference image in the top left and the 30, 40 and 50% k-space line replacement images assigned randomly to the other squares, see figure 1.
Results
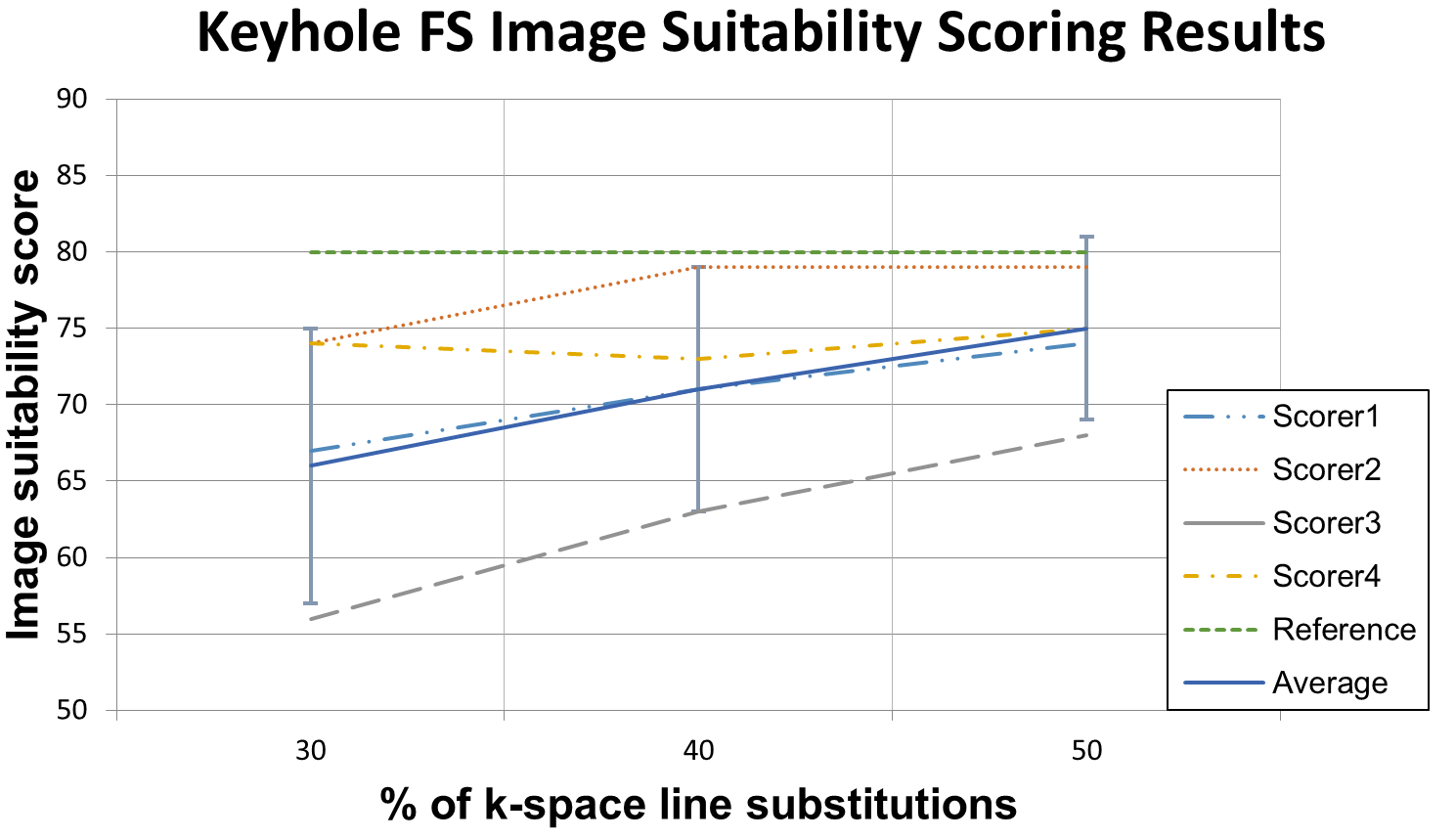
Figure 2 shows the results from the four scorers and averages obtained thereafter.The mean (standard deviation) for the images synthesized with 30, 40 and 50% k-space substitution was 66(9), 71(8) and 75(6) out of 100, where the reference image was assigned a score of 80.
Discussion
The results give confidence that the proposed keyhole FS method can produce FS images of sufficient quality for radiotherapy treatment planning purposes. Images synthesized via 50% FS k-space line replacement into a full non FS k-space were found to be only slightly inferior to FS images acquired in the traditional way. The inter-scorer variation, as reflected in the standard deviation of the average scores across the four scorers, was large and potentially demonstrated that oncologists look for different things from their FS T2W planning MR images.To prospectively acquire images using the described technique a specially designed pulse sequence would be required to capture the full non-FS image and a subset of FS k-space with two orthogonal phase encode directions. Such a prospective pulse sequence will be tested in further work. Beyond the simple time saving afforded by acquiring fewer lines of FS k-space, the acquisition of an interleaved multi-contrast keyhole pulse sequence would offer intrinsic spatial registration between the two reconstructed images, and thus add further benefit to the MR treatment planning pathway.
Conclusion
This work demonstrated the possibility for intrinsically registered fat saturated an unsaturated T2W lung MRI images to be acquired in one keyhole pulse sequence for the purposes of radiotherapy treatment planning. The proposed method would save time in the patient workflow and thereby increase patient comfort and compliance. The method may have wider clinical benefit in other anatomies for radiotherapy MR treatment planning and in radiology where FS and non FS images are required of the same anatomy.Acknowledgements
No acknowledgement found.References
1. Bainbridge, H. et al., 2017. Magnetic resonance imaging in precision radiation therapy for lung cancer. Translational Lung Cancer Research, 6(6), pp. 689-707.
2. Dubec, M. et al., 2017. MRI for Lung Cancer Radiotherapy Treatment Planning and Treatment. Journal of Thoracic Oncology, 12(11, S2), p. S2334.
3. Cobben, D. C. P. et al., 2016. Emerging Role of MRI for Radiation Treatment Planning in Lung Cancer. Technology in Cancer Research in Treatment, 15(6), pp. NP47-60.
4. Flask et al., 2003. Keyhole Dixon Method for Faster, Perceptually Equivalent Fat Suppression. Journal of Magnetic Resonance Imaging, 18 pp. 103-112.
Figures