4827
Combined SENSE and Compressed Sensing to Enhance Radiation Therapy MR Simulation1Medical Physics, Memorial Sloan Kettering Cancer Center, New York, NY, United States, 2Philips Healthcare, Best, Netherlands, 3Radiation Oncology, Memorial Sloan Kettering Cancer Center, New York, NY, United States
Synopsis
We evaluated a combination of SENSE acceleration and compressed sensing in the MR simulation workflow to reduce scan time and improve image quality and anatomical coverage. Imaging series were performed with SENSE-only and with a combined SENSE+compressed sensing (CS) software package. CS resulted in an average reduction of 28% in single-series scan time with negligible changes in image quality and the ability to contour structures for RT treatment planning. In addition, CS permitted pulse sequence modifications which reduced respiratory artifacts, improved visibility of the prostatic urethra, and eliminated the need for a Foley catheter in prostate cancer patients.
Introduction
It is well recognized that one of the drawbacks of MR Imaging is long scan times, and it is better for both patient comfort and health care economics to perform exams as quickly as possible. When MRI is employed for radiation therapy (RT) simulation, patients are positioned in immobilization devices, and, depending on the irradiation site, may need to be simulated under breath-hold, full bladder, and empty rectum conditions to ensure reproducible setup and/or maximize normal organ sparing. These factors further motivate efforts to reduce scan times. We are reporting on the use of a combination of SENSE [1] and compressed sensing [2] in a product called Compressed SENSE [3] in the MR simulation (MRSim) workflow to 1) reduce scan time, and/or 2) improve image quality and anatomical coverage.Methods
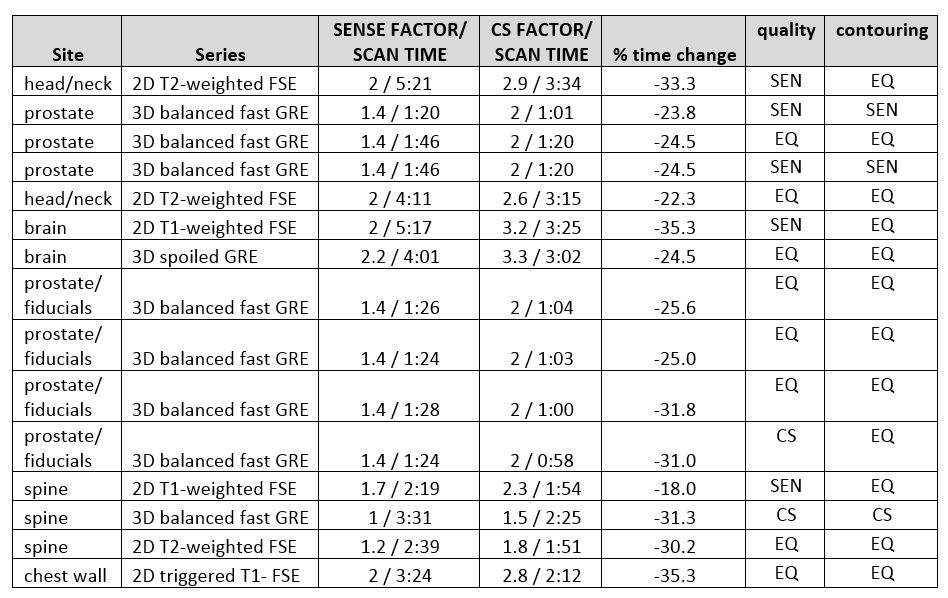
All scans were performed on a 3T Philips Ingenia (Philips, Best, The Netherlands) running software version 5.4 or 5.6 and equipped with a flat tabletop for MRSim. This scanner can accelerate imaging using SENSE [1] or the Compressed SENSE product (CS) which combines SENSE coil-based acceleration with sparse sampling and iterative reconstruction. The current study compared existing SENSE-accelerated MRSim series to identical series in which CS replaced SENSE. In 15 patients scanned between Sept. 1 and Nov. 1, 2019, one MR series per patient was selected to be acquired twice: once with SENSE and once with CS to permit direct comparison. All geometric parameters were kept constant. Table 1 contains the anatomical sites, series descriptions, and acceleration factors. The acceleration factor used for CS was based on the vendor’s recommendations for 2D or 3D imaging. The regularization parameter which generated the least blurring was used. For each SENSE-CS pair, image quality and the ability to contour lesions were assessed by a radiation oncologist with 9 years of experience in MR in RT. Image quality encompassed perceived SNR, sharpness, and presence/absence of artifacts. The series used for imaging gold fiducial markers in the prostate were further assessed by contouring the markers and comparing the contoured volumes using an unpaired student’s t test. Additional series employing CS are discussed in Results to illustrate alternative image quality improvement strategies.Results
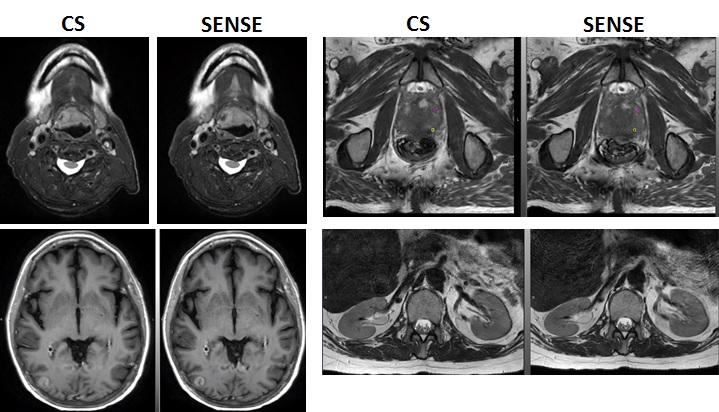
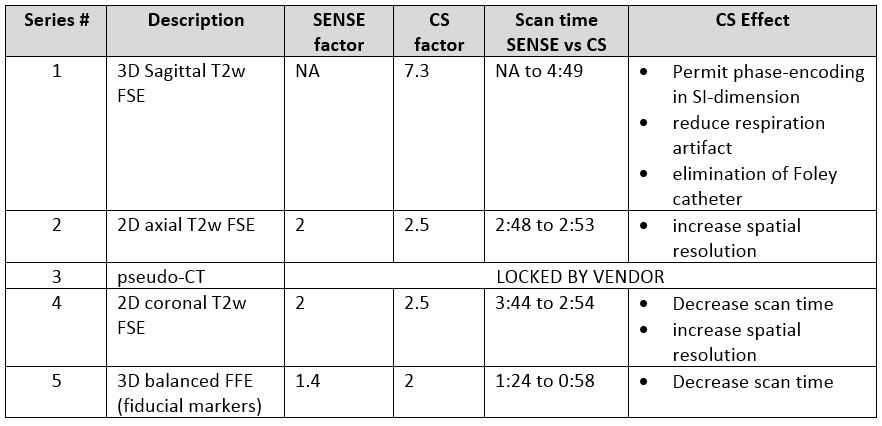
Example images for head and neck, prostate, brain, and spine are shown in Figure 1. Table 1 contains a comparison of scan times for 15 SENSE and CS-accelerated series. The average CS scan time reduction for both 2D and 3D sequences was 28%. When evaluating image quality, the radiation oncologist found equivalent image quality in 8 cases, SENSE superior in 5, and CS superior in 2. For contouring, 12 cases were rated equivalent, SENSE was superior in 2, and CS was superior in 1. The volumes of prostate fiducial markers contoured in seven series did not differ significantly when acquired with CS vs. SENSE (P > 0.5). Not included in the table is a lower extremity MR simulation in which we applied CS in seven 2D FSE series including axial upper/lower T1w and T2w, coronal T1w and T2w and sagittal T2w. Compared to a previous lower extremity simulation which employed SENSE only, total scan time was reduced from 33 to 24 minutes using CS (27%).Prostate simulations comprise the vast majority of our patient cohort (~80 cases/month) and have therefore provided the most opportunity for optimization with CS. The five series comprising the prostate MRSim (Table 2) demonstrate the variety of applications of CS. In series 2, 4, and 5, the acceleration provided by CS was traded for reduced scan time and/or increased in-plane spatial resolution. Series 1, a 3D scan which is used to contour the prostatic urethra, would normally be prescribed with phase encoding in RL and AP dimensions to limit scan time. However, phase encoding in the AP dimension results in respiratory artifacts which can obscure the urethra. Swapping phase-encoding to the superior-inferior dimension and oversampling to avoid aliasing resulted in a scan time of over 9 minutes with SENSE, which was unacceptable in patients. However, with a CS factor of 7.3, we were able to obtain the image in 4 min 43 s. Moreover, this permitted us to eliminate the use of the Foley catheter for urethra visualization, reducing the overall workflow time.
Discussion
The combination of SENSE-based acceleration with sparse sampling and iterative reconstruction (compressed sensing) permitted us to reduce MRSim series times by an average of 28%. In the majority of cases, image quality and ability to contour were equivalent in CS and SENSE series. In the seven cases where image quality was non-equivalent, SENSE was superior in 5, suggesting a slight advantage in SNR. There was negligible difference in the ability to contour with CS vs SENSE. While the potential benefit of CS is greater in 3D series where there are two phase-encoding dimensions, we were able to substantially improve scan times in 2D series as well. In prostate simulation, CS permitted improved image quality in the same scan time and, importantly, allowed us to eliminate the Foley catheter from our workflow.Conclusion
Combined SENSE and compressed sensing results in reduced scan times while maintaining high image quality for MR Simulation.Acknowledgements
The authors would like to thank the MRI technologists and therapists in the Department of Radiation Oncology for their skilled assistance.References
[1] Pruessmann KP, Weiger M, Scheidegger MB, Boesiger P. SENSE: sensitivity encoding for fast MRI. Magn Reson Med 1999;42(5):952-962.
[2] Lustig M, Donoho D, Pauly JM. Sparse MRI: The application of compressed sensing for rapid MR imaging. Magn Reson Med 2007;58(6):1182-1195.
[3] Gierts-Ossevoort, L., et. al. Compressed SENSE: Speed Done Right. Every Time. Whitepaper. Philips Healthcare, Best, The Netherlands. 2018.
Figures