4826
Deep Learning to Discriminate Nasopharyngeal Carcinoma and Benign Hyperplasia on MRI
Lun M. Wong1, Ann D. King1, and Qiyong Ai1
1Department of Imaging and Interventional Radiology, The Chinese University of Hong Kong, Shatin, Hong Kong
1Department of Imaging and Interventional Radiology, The Chinese University of Hong Kong, Shatin, Hong Kong
Synopsis
Benign hyperplasia is a common finding in the adenoid and walls of the nasopharynx and may hamper the detection of early-stage nasopharyngeal carcinoma (NPC) on MRI. In this study we aim to utilize deep learning to discriminate early-stage NPC from benign hyperplasia using T2-weighted-fat-suppressed MR images. We tested our method on a dataset of 413 cases, comprising 203 with early-stage NPC confined to the nasopharynx and 210 with benign hyperplasia. After training with validation (n=350 and n=13 respectively) followed by testing (n=50), the network achieved a promising result with a sensitivity of 100% and specificity of 83% for NPC detection.
Introduction
Nasopharyngeal carcinoma (NPC) is a disease prevalent in areas of the world such as South Asia China. Diagnosis of the disease at an early-stage is crucial to the survival of patients with NPC. In this regard, MRI is being used increasingly to detect small cancers that cannot be seen through the endoscope1, especially in those patients who have been screened for the disease using blood markers for the Epstein Barr Virus2,3.However, benign hyperplasia of the nasopharynx is common and causes enlargement of the adenoid and nasopharyngeal wall thickening which may overlap in appearance with that of early-stage NPC on the anatomical MRI sequences4 as shown in Fig. 1. Therefore, we have been researching new techniques that may aid discrimination, including the diffusion weighted imaging (DWI)5, but results showed some limitations. Furthermore, manual delineations are required which is laborious and time consuming. Therefore, an automatic solution which can discriminate benign and malignant nasopharyngeal lesions would be advantageous for NPC detection.
Artificial neural networks have the potential to perform this task. While artificial neural networks have unparalleled natural image classification capability the usage in medical imaging, especially for 3-dimensional (3D) volumes, is still being explored. The purpose of this study is to investigate whether convolutional neural networks (CNN) can be exploited to automatically detect early-stage NPC on MR imaging.
Method
This retrospective study was performed with local institutional board approval. Patients were ethnically Chinese who underwent T2-weighted-fat-suppressed MRI of the nasopharynx imaging in our institution between 2010 and 2019. Two groups of patients were included in the study: (1) those with newly biopsy-proven undifferentiated NPC whose primary tumours were staged as T1 with a minimal axial diameter ≥ 5mm and (2) those with benign hyperplasia with a minimal axial diameter ≥ 5mm without evidence of NPC on MRI and endoscopic examination. A total of 413 patients, 203 with NPC stage T1 and 210 with benign hyperplasia, were analysed.The image volume went through a pipeline of pre-processing filters, including alignment with the axis of symmetry using EROS6, intensity Nyul normalization7 and cropping to uniform size of 20x444x444px.
We adopted the Residual Attention Network (RAN)8 as our backbone and modified the convolutional kernels to suit the 3D inputs. Specifically, all the pooling layers were set to pool along 2D sagittal-coronal layers only, whereas all convolutional layers convolved with 3D kernels. Dropout layers were added to residual units to facilitate model robustness. The RAN consists of an attention branch that allows the network to learn a feature mask that reinforces useful deep features to mitigate the complex anatomy at the nasopharynx.
We randomly divided our dataset into training (n=350), validation (n=13) and testing (n=50) group. The network was allowed to train for 5500 epochs over the training data with an initial learning rate of 10-4, which decayed exponentially after each epoch, optimizing cross-entropy loss with stochastic gradient decent. The validation accuracy suggests the network converges at approximately 2000 epochs as shown in Fig. 2. The learnt model was then applied to the testing set. The sensitivity, specificity, positive predictive value (PPV) and negative predictive value (NPV) were evaluated.
Results
There were five false positive and no false negative results for NPC. The performance of the network showed a sensitivity of 100%, specificity of 83%, PPV of 81%, NPV of 100% and accuracy of 90%. The computed probabilities of NPC and benign hyperplasia in the 50 patients in the testing group are listed in Table 1.Discussion
Our results suggest CNN with the RAN architecture as described is a promising tool for NPC detection on T2-weighted-fat-suppressed MR and most cases were classified correctly with a high level of confidence, indicated by the large prediction probability differences. Furthermore, three of the five benign hyperplasia cases misclassified as NPC showed results with relatively low confidence intervals. This suggests the probability ratio could alert the radiologist to cases likely to be false positive for NPC and in the future these cases could be reduced by tuning the threshold probability ratio.Conclusion
CNN is a promising tool for MRI detection of early-stage nasopharyngeal carcinoma.Acknowledgements
References
- King AD, Vlantis AC, Bhatia KSS, et al. Primary nasopharyngeal carcinoma: diagnostic accuracy of MR imaging versus that of endoscopy and endoscopic biopsy. Radiology. 2011;258(2):531-537.
- Chan KCA, Woo JKS, King A, et al. Analysis of Plasma Epstein-Barr Virus DNA to Screen for Nasopharyngeal Cancer. N Engl J Med. 2017;377(6):513-522.
- King AD, Woo JKS, Ai QY, et al. Complementary roles of MRI and endoscopic examination in the early detection of nasopharyngeal carcinoma. Ann Oncol. 2019;30(6):977-982.
- King AD, Wong LYS, Law BKH, et al. MR Imaging Criteria for the Detection of Nasopharyngeal Carcinoma: Discrimination of Early-Stage Primary Tumors from Benign Hyperplasia. AJNR Am J Neuroradiol. 2018;39(3):515-523.
- Ai Q-Y, King AD, Chan JSM, et al. Distinguishing early-stage nasopharyngeal carcinoma from benign hyperplasia using intravoxel incoherent motion diffusion-weighted MRI. Eur Radiol. 2019;29(10):5627-5634.
- Chen X, Tian J, Zhang Y, Yang X. A Robust Orientation Estimation Algorithm for Low Quality Fingerprints. In: IWBRS 2005: Advances in Biometric Person Authentication. Heidelberg: Springer; 2005:95-102.
- Sun X, Shi L, Luo Y, et al. Histogram-based normalization technique on human brain magnetic resonance images from different acquisitions. Biomed Eng Online. 2015;14:73.
- Wang F, Jiang M, Qian C, et al. Residual attention network for image classification. In: Proceedings - 30th IEEE Conference on Computer Vision and Pattern Recognition, CVPR 2017. Vol 2017-Janua. ; 2017:6450-6458.
Figures
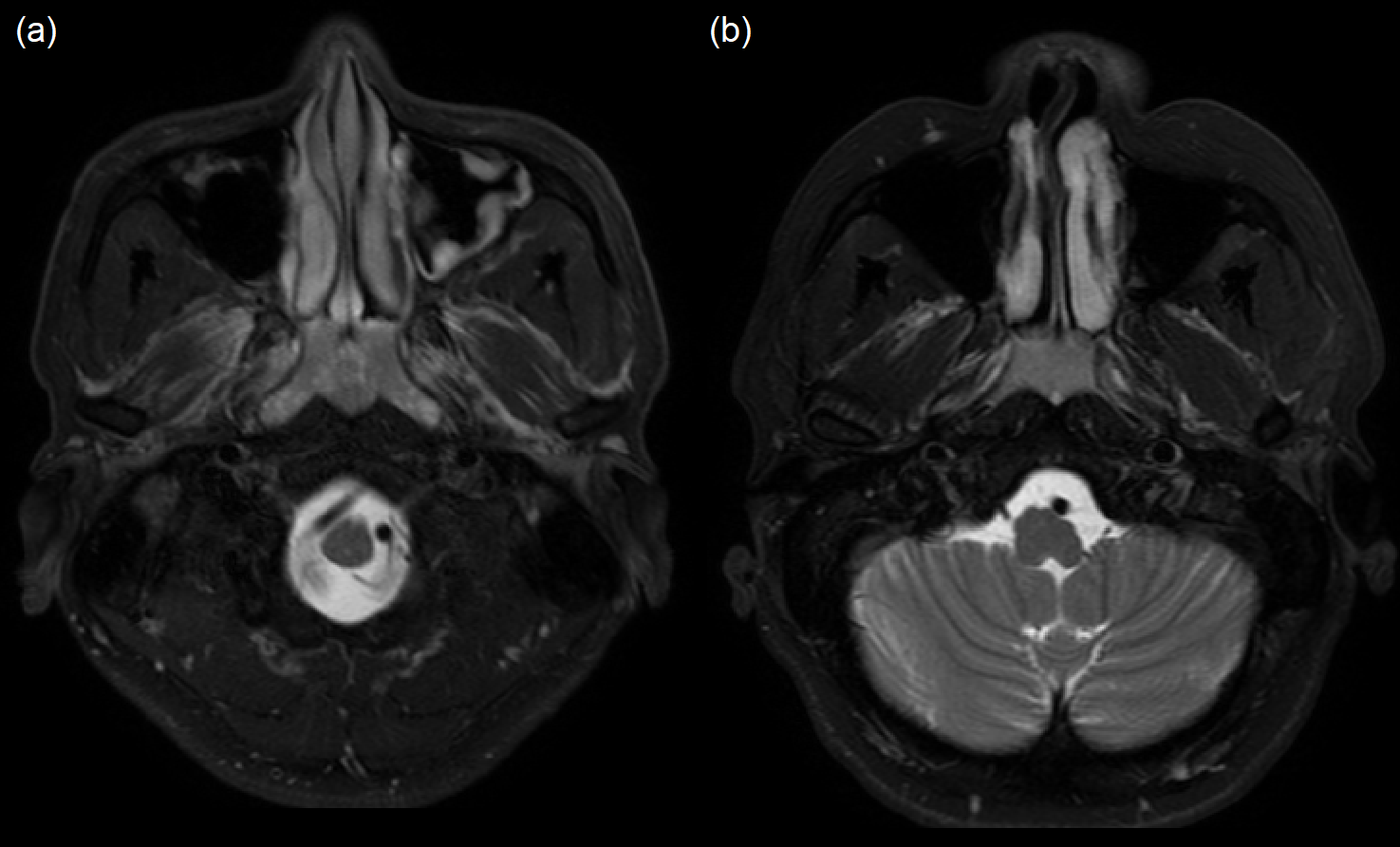
Figure 1. MR T2W fat-suppressed axial image of the nasopharynx in a patient
with (a) benign hyperplasia and (b) stage T1 NPC.
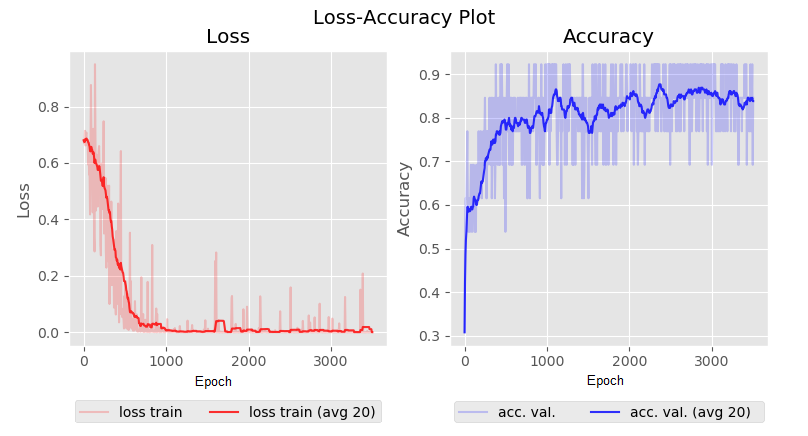
Figure 2. The loss-accuracy plot during training. Plot on the left in red shows
the cross-entropy loss against epoch during training. Plot on the right in blue
shows the validation accuracies against epoch during training. The plots
suggest the training process converges at around 2000 epochs.
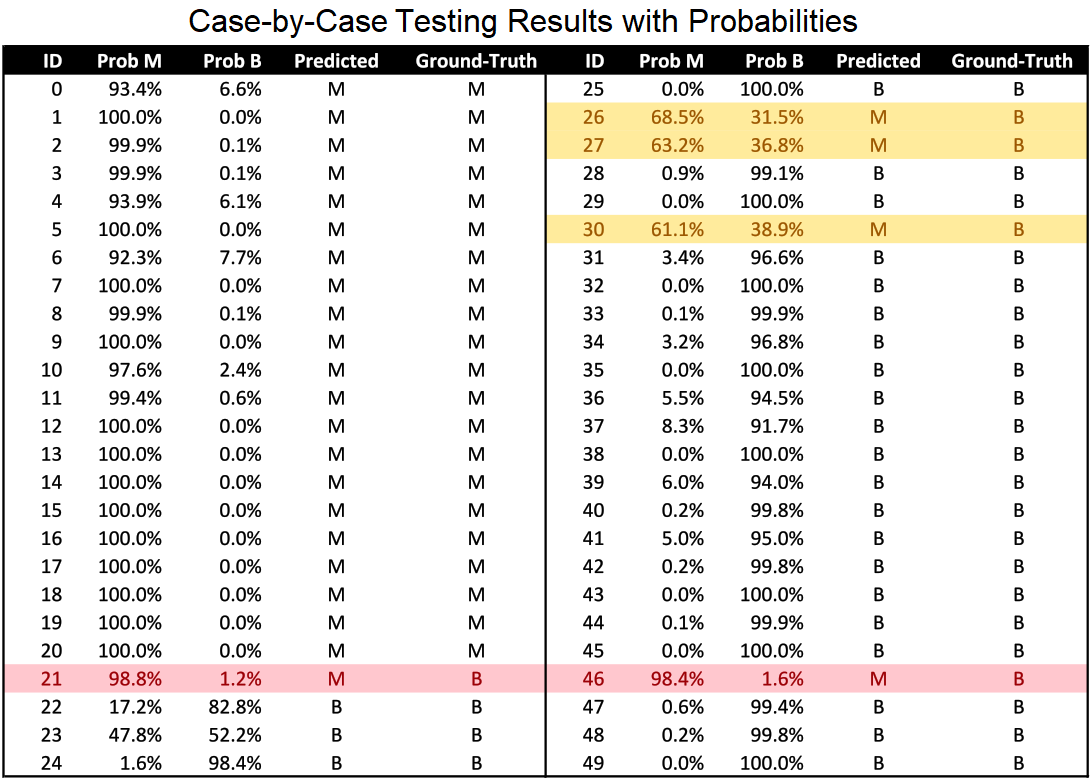
Table 1. Probabilities
of malignancy (M) and benign hyperplasia (B) in 50 test cases. The false
positive cases for malignancy are highlighted in yellow for three cases with a low
level of confidence and red for the two remaining cases.