4767
3D Isotropic Resolution Distortion-free Diffusion-Prepared Magnitude-Stabilized bSSFP Imaging at 1.5 Tesla1Radiological Sciences, University of California, Los Angeles, Los Angeles, CA, United States, 2MR R&D Collaborations, Siemens Healthineers, Los Angeles, CA, United States
Synopsis
Strong spatial distortion of the DW-ssEPI sequence prevents its utilization in radiotherapy planning and treatment adaptation. In this work, a 3D diffusion-prepared magnitude-stabilized bSSFP sequence was developed and validated at 1.5T. A phase navigator was acquired during the catalyzation stage of the bSSFP readout to estimate the spatial variation of the signal phase, and a locally low-rank constrained reconstruction was developed to resolve the phase variation. The sequence was validated on a diffusion phantom and healthy volunteers. It provided submillimeter geometric fidelity and acceptable ADC accuracy, which makes it a promising candidate for treatment planning and adaptation of the brain.
Introduction
MRI is increasingly used in radiotherapy workflow1. Diffusion-weighted imaging (DWI) has been shown to have exceptional value for tumor delineation and response assessment2. A major obstacle that prevents applying DWI for treatment planning and online adaptive radiotherapy is the strong spatial distortion in the conventional diffusion-weighted single-shot echo-planar imaging (DW-ssEPI) sequence, which is problematic for geometrically accurate radiotherapy target delineation. Therefore, the goal of this work is to develop a 3D diffusion sequence to achieve 1.5mm isotropic resolution distortion-free diffusion imaging for treatment planning and radiotherapy treatment adaptation of the brain.Methods
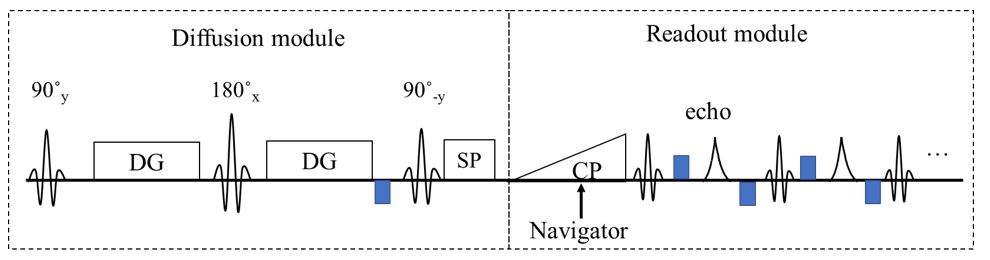
Sequence: A previously proposed diffusion-prepared magnitude-stabilized bSSFP (DP-MS-bSSFP, abbreviated as DP-MS) sequence3 was extended to 3D. The sequence diagram of one example imaging shot is shown in Figure 1. In multi-shot diffusion imaging, the use of strong diffusion gradients magnifies motion and system imperfections and creates strong Eddy currents, which then leads to different signal phase accrual for different k-space segments. A 2D navigator was acquired during the built-in linear catalyzation pulses to estimate and correct the MR signal phase inconsistency between different shots. It assumes that the through-slab phase variation is negligible, and has been shown to be valid for slab thickness less than 30mm in the brain4,5.Reconstruction: The multi-shot 3D diffusion data was then phase corrected slice-by-slice6. A 1D Fourier transform was first applied along the kz direction. Then for each slice, the k-space data from each individual imaging shot was used to reconstruct one image. Under ideal scenario where no physiological motion occurs between shots, the reconstructed image series from multiple shots should be identical, and hence the rank of the Casorati matrix would be 1. Therefore, we propose a locally low-rank constrained reconstruction:
$$min_x\sum_{j=1}^{n_c}\sum_{i=1}^L||D_iFS_jP_{ij}x_i-y_{ij} ||_2^2+\gamma \sum_{b\in\Omega} ||C_bx||_\ast$$
where $$$y_{ij}$$$ is the acquired k-space data from the $$$i^{th}$$$ shot and $$$j^{th}$$$ coil, $$$x_i$$$ is the coil-combined image reconstructed from the $$$i^{th}$$$ shot, $$$x$$$ is the matrix concatenating all images from different shots, $$$F$$$ is the Fourier transform, $$$D_i$$$ is the under-sampling operator for $$$i^{th}$$$ shot, $$$P_{ij}$$$ is the phase compensation matrix derived from the Gaussian-windowed phase of the built-in ramp-up navigator, $$$S_j$$$ is the $$$j^{th}$$$ coil sensitivity map. $$$\Omega$$$ is a set of small image blocks partitioned from $$$x$$$, $$$C_b$$$ is the operator that takes image block from the set $$$\Omega$$$ and forms its Casorati matrix, $$$||\cdot||_{\ast}$$$ is the nuclear norm, and $$$\gamma $$$ is the regularization parameter.
Phantom study: A diffusion phantom was scanned on a 1.5T scanner (Avanto, Siemens Healthineers) to evaluate the geometric fidelity and ADC accuracy. Scan parameters for the DW-ssEPI sequence and the DP-MS sequence were: TR=6100/2000ms, TE=86/120ms, field of view=240x240mm2 , resolution=1.5mm3, bandwidth= 1562/780 Hz/px, average= 12/1, 32 slices (25% oversampling in DP-MS), scan time=2min46s/9min36s, respectively. b-value of 0 and 800 s/mm2 were acquired. In DP-MS, each kz plane was covered with four shots. The turbo spin-echo sequence was acquired as the geometric reference. A total of 8 landmarks were selected on each slice of images to calculate the target registration error (TRE) with the TSE reference, a surrogate of the geometry accuracy. ADC values from DP-MS were compared with ADCs from DW-ssEPI.
In-vivo study: Four healthy volunteers were recruited to evaluate the in-vivo performance. A total of 48 slices in three slabs were acquired to evaluate and compare the geometric fidelity and ADC. Eight to ten landmarks were picked in each slice to calculate the TRE. A region of interest (ROI) was drawn on the white matter for all slices. Additional ROIs were drawn on the cerebrum and CSF region for slices that contain the cerebrum and the ventricle. The Bland-Altman analysis was performed to evaluate the ADC agreement between DW-ssEPI and DP-MS.
Results
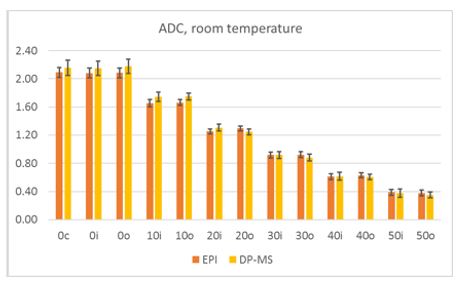
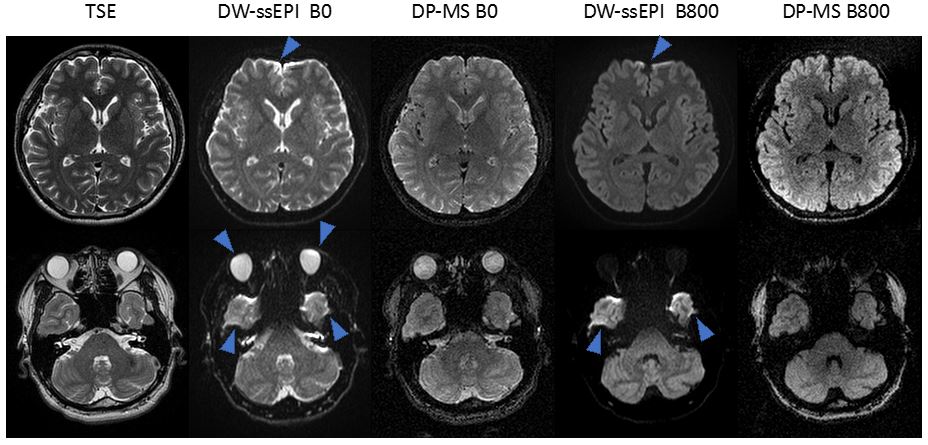
As shown Figure 2, DW-ssEPI image had strong distortion and susceptibility related artifacts, whereas no obvious artifact was observed in DP-MS image. Compared with TSE images, the maximum landmark displacement was 8.34mm for DW-ssEPI, and 3.13mm for DP-MS. TREs from DP-MS (0.70±0.50 mm) were significantly lower than TREs from DW-ssEPI (2.09±1.75mm).Figure 3 shows the phantom ADC results. There was a good agreement of ADC values measured from the two diffusion sequences. The percent difference was less than 7%.
An in-vivo comparison is shown in Figure 4. Distortion and signal pile-up were apparent on DW-ssEPI images, particularly at the base of the brain. DP-MS provided high-quality diffusion images with no observable distortion. The mean TRE of DW-ssEPI was over 2mm for all four volunteers, and the maximum displacement was almost 10mm. The mean TRE was less than 0.8mm for DP-MS.
The Bland-Altman plots of the mean diffusivity for selected ROIs on the white matter, cerebellum, and CSF were shown in Figure 5. Overall, there were good agreements of ADC between the two diffusion approaches, and the systematic biases were low (0.01x10-3mm2/s, 0.02x10-3mm2/s, and -0.02x10-3mm2/s for white matter, cerebellum, and CSF, respectively).
Discussion and conclusion
In this work, a 3D diffusion-prepared magnitude-stabilized bSSFP sequence was developed and validated for high-quality distortion-free diffusion imaging. It provided submillimeter geometric fidelity and acceptable ADC accuracy on phantom and volunteer brain scan, which makes it a promising candidate for treatment planning and adaptive radiotherapy.Acknowledgements
No acknowledgement found.References
1. Benedict SH, Yenice KM, Followill D, et al. Stereotactic body radiation therapy: The report of AAPM Task Group 101. Med Phys. 2010;37(8):4078-4101. doi:10.1118/1.3438081
2. Leibfarth S, Winter RM, Lyng H, Zips D, Thorwarth D. Potentials and challenges of diffusion-weighted magnetic resonance imaging in radiotherapy. Clin Transl Radiat Oncol. 2018;13:29-37. doi:10.1016/j.ctro.2018.09.002
3. Gao Y, Han F, Zhou Z, et al. Multishot diffusion-prepared magnitude-stabilized balanced steady-state free precession sequence for distortion-free diffusion imaging. Magn Reson Med. 2019;81(4):2374-2384. doi:10.1002/mrm.27565
4. Engström M, Skare S. Diffusion-weighted 3D multislab echo planar imaging for high signal-to-noise ratio efficiency and isotropic image resolution. Magn Reson Med. 2013;70(6):1507-1514. doi:10.1002/mrm.24594
5. Chang H-C, Hui ES, Chiu P-W, Liu X, Chen N-K. Phase correction for three-dimensional (3D) diffusion-weighted interleaved EPI using 3D multiplexed sensitivity encoding and reconstruction (3D-MUSER). Magn Reson Med. 2018;79(5):2702-2712. doi:10.1002/mrm.26944
6. Chang H-C, Sundman M, Petit L, et al. Human brain diffusion tensor imaging at submillimeter isotropic resolution on a 3Tesla clinical MRI scanner. NeuroImage. 2015;118:667-675. doi:10.1016/j.neuroimage.2015.06.016
Figures