4623
Quiet Diffusion-weighted Imaging in Pediatric Patients with Moyamoya Disease1Department of Diagnostic Imaging and Nuclear Medicine, Kyoto University Graduate School of Medicine, Kyoto, Japan, 2Human Brain Research Center, Kyoto University Graduate School of Medicine, Kyoto, Japan
Synopsis
Diffusion-weighted imaging (DWI) is an essential MR sequence for evaluating pediatric patients with moyamoya disease (MMD). Acoustic noise associated with DWI may lead to motion artifact. Compared with conventional DWI (cDWI), quiet DWI (qDWI) is considered less noisy and able to keep children more relaxed and stable. We evaluated the advantages of qDWI compared with cDWI in pediatric MMD patients. Compared with cDWI, qDWI induced fewer artifacts in sedated pediatric MMD patients, whereas in unsedated patients, the frequencies of qDWI- and cDWI-induced artifacts were similar. qDWI and cDWI had the same performance for detecting restricted diffusion.
Introduction
Moyamoya disease (MMD) is a cerebrovascular disorder characterized by steno-occlusion of the carotid arteries. Conventional DWI (cDWI) is acquired with single-shot echo-planar imaging (EPI). The EPI sequence relies on fast switching of gradient amplitudes, generating a level of acoustic noise that is the highest among the routine brain MR imaging sequences. Because the noise is uncomfortable, children find it difficult to remain still during image acquisition, and young children in particular need sedation to eliminate motion artifact in the images. However, sedation using anesthesia elicits safety concerns. Quiet DWI (qDWI) with acoustic noise reduction has recently been introduced to clinical practice, and is achievable using readout-segmented EPI scanning in combination with partial-Fourier acquisition in the phase-encoding direction.1, 2 The acoustic noise is lessened by reducing the forces generated in the gradient coils.3, 4 Compared with cDWI, qDWI is considered a gentler sequence for pediatric patients. The aim of this study was to evaluate the advantages of qDWI compared with cDWI for pediatric MMD patients.Methods
This retrospective study was approved by our Institutional Review Board, and written informed consent was waived.Patients
We evaluated 106 MR scans of 56 MMD patients who underwent MR examinations between September 2017 and August 2018: 38 scans of 15 sedated patients (6 boys, 9 girls; mean age, 5.2 years; range, 1–9 years) and 68 scans of 42 unsedated patients (19 boys, 23 girls; mean age, 10.7 years; range, 7–16 years). In all patients (except one girl), the MR examination was performed either with or without sedation.
Image acquisition
MR imaging was obtained using 3T units (MAGNETOM Prisma and MAGNETOM Skyra; Siemens Healthineers, Erlangen, Germany). The acquisition parameters for qDWI were as follows: repetition time, 5440 ms for MAGNETOM Prisma and 7370 ms for MAGNETOM Skyra; echo time, 61 ms for MAGNETOM Prisma and 67 ms for MAGNETOM Skyra; slice thickness, 3 mm; matrix, 160 × 160; field of view, 220 × 220 mm; phase partial Fourier, 7/8; number of slices, 35; bandwidth 780 Hz/pixel; averages, 1; acquisition time, 1 m 56 s for MAGNETOM Prisma and 2 m 36 s for MAGNETOM Skyra; parallel acquisition technique, 2; readout segments, 3. The acquisition parameters for cDWI were as follows: repetition time, 4900 ms; echo time, 75 ms; slice thickness, 3 mm; acquisition matrix, 160 × 160; field of view, 220 × 220 mm; phase partial Fourier, 7/8; number of slices, 35; bandwidth 1360 Hz/pixel; averages, 5; acquisition time, 2 m 4 s; parallel acquisition technique, 3. qDWI and cDWI were acquired with b = 0 and b = 1000. Fifty-three scans were performed in the order of qDWI followed by cDWI, and the remaining 53 scans were obtained in reverse order.
Image analysis
Two neuroradiologists with 13 and 10 years of experience, who were blinded to the sequence type, reviewed the images independently. Artifacts were defined as abnormal image findings that displayed blurring and ghosting other than susceptibility or probable stroke lesions. Artifacts were evaluated separately in the sedated and unsedated patients. Restricted diffusion in the brain was also evaluated. Any disagreements between the neuroradiologists were resolved by a third neuroradiologist with 22 years of experience.
Statistical analysis
A chi-square test was used to compare the frequency of artifacts and restricted diffusion between qDWI and cDWI. A P value of <.05 was considered statistically significant.
Results
Artifacts in sedated patientsNo artifacts were observed on qDWI, but were evident in four cases in which blurring and ghosting were observed on cDWI (P = .04). One patient awoke from sedation during cDWI acquisition, and no cDWI was obtained.
Artifacts in unsedated patients
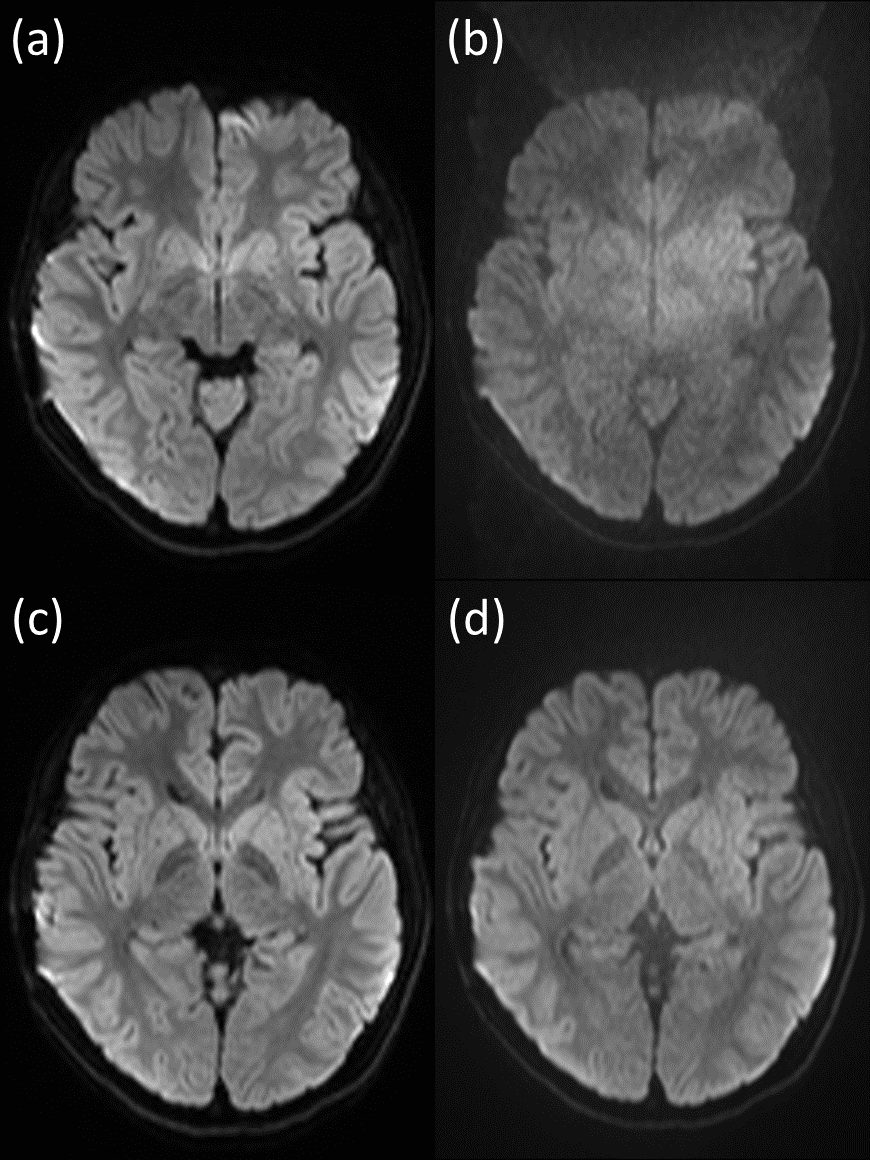
Three patients had artifacts on qDWI, whereas two patients had artifacts on cDWI. There was no significant difference between the two sequences in terms of artifacts (P = .65). Figure 1 shows qDWI and cDWI of a representative patient.
Restricted diffusion in sedated and in unsedated patients
cDWI revealed three instances of restricted diffusion, all of which were also found on qDWI (no significant difference, P = .99).
Discussion
The blurring and ghosting artifacts observed on cDWI were caused by head motion. These artifacts were observed on only a few of the images. qDWI is equipped with motion correction because readout-segmented EPI is a multi-shot sequence and is sensitive to motion.5 However, it is difficult to eliminate motion artifact. In qDWI, no averaging was applied, whereas cDWI was acquired with five averages. However, because the abilities of the two sequences to detect lesions with restricted diffusion were the same, and the artifact rates were similar, we consider that qDWI can be substituted for cDWI. The reduction of acoustic noise by 4.1–5.5 dB in qDWI corresponds to a reduction of 38%–47% in sound pressure compared with cDWI, according to our internal survey.Conclusion
Compared with cDWI, qDWI induced fewer artifacts in sedated pediatric MMD patients, whereas in unsedated patients, the frequencies of qDWI- and cDWI-induced artifacts were similar. qDWI and cDWI had the same performance for detecting restricted diffusion.Acknowledgements
We are grateful to Yuta Urushibata from Siemens Healthcare K.K. for the helpful discussion.References
1. Rösch J, Ott M, Heismann B, et al. Quiet diffusion-weighted head scanning: Initial clinical evaluation in ischemic stroke patients at 1.5T. J Magn Reson Imaging 2016;44:1238-1243
2. Heismann B, Ott M, Grodzki D. Sequence-based acoustic noise reduction of clinical MRI scans. Magn Reson Med 2015;73:1104-1109
3. Ott M, Blaimer M, Grodzki DM, et al. Acoustic-noise-optimized diffusion-weighted imaging. MAGMA 2015;28:511-521
4. Pierre EY, Grodzki D, Aandal G, et al. Parallel imaging-based reduction of acoustic noise for clinical magnetic resonance imaging. Invest Radiol 2014;49:620-626
5. Holdsworth SJ, Skare S, Newbould
RD, et al. Robust GRAPPA-accelerated diffusion-weighted readout-segmented
(RS)-EPI. Magn Reson Med
2009;62:1629-1640
Figures