4614
Differences in Functional Integration and Segregation in CHD Neonates: Interactions with Sex1Radiology, Children's Hospital of Pittsburgh of UPMC, Pittsburgh, PA, United States, 2Children's Hospital of Los Angeles, Los Angeles, CA, United States
Synopsis
Functional network topology was compared between neonates with congenital heart disease (CHD) and normal controls and sex-X-CHD interactions were investigated. Using a cost-independent analysis, CHD neonates displayed reduced segregation globally (modularity, transitivity) and nodally (clustering coefficient, participation coefficient) mainly in frontal and subcortical regions; no significant sex-X-CHD interactions were found. Using a cost-dependent analysis, CHD neonates displayed reduced integration and segregation globally (global efficiency, transitivity) and nodally (nodal efficiency, clustering coefficient) in frontal, temporal, and subcortical regions. Significant sex-X-CHD interactions (M>F) were found in similar regions. Results may support a neurophysiological basis for differential neurodevelopmental outcomes related to sex.
Introduction
Patients with congenital heart disease (CHD) are at increased risk for impaired neurocognitive function in a variety of domains1 and have shown brain dysmaturation beginning in infancy2. However, possible sex differences have not been explored in detail. We investigate differences in brain functional topology in a cohort of infants with CHD compared to normal controls as well as sex-X-CHD interaction effects.Materials and Methods
Resting-state BOLD data was successfully acquired from 218 infants (89 CHD, 129 Control) under normal sleep without sedation using a feed-and-bundle technique. All participants were full-term. CHD Cohort: 35F, 54M, Post-Conceptional Age (PCA) at Birth: 38.85 +/- 0.87 weeks; PCA at Scan: 43.75 +/- 5.15 weeks. Controls: 78F, 51M, PCA at Birth: 39.23 +/- 1.17 weeks: PCA at Scan: 45.15 +/- 4.88 weeks. Data was acquired at Children’s Hospital of Pittsburgh of UPMC (CHP) on a 3T Siemens Skyra scanner and a 3T GE Excite scanner, and at Children’s Hospital Los Angeles (CHLA) on a 3 T Philips Achieva scanner. CHD infants were heterogenous with regard to type of heart lesion with no frank visible injury.Previously published methods3 were used to minimize the risk of spurious correlations arising from participant motion involving slice-timing correction, motion correction (affine transform), spatial coregistration using a study-specific template, global norm = 1000, and volume censoring with intensity cost function (DVARS) < 25 and framewise displacement (FD) < 0.2 mm. A neonatal-specific parcellation atlas4 was used to generate time courses from 90 cortical regions; nuisance parameters (motion correction, drift) were regressed out and band-pass frequency filtering was used (0.009 Hz < f < 0.08 Hz) for each time course. Correlation matrices (90-X-90) were computed. A dataset was deemed acceptable and included in the analysis if there were at least 3 minutes of BOLD data remaining after censoring.
Graph analysis parameters were computed using Brain Connectivity Toolbox (BCT) and additional routines written in IDL. Graphs were thresholded according to fixed values of cost (0.05 to 0.45 with step size of 0.05; Cost-Independent analysis) and also according to fixed value of R determined by average value of cost (0.05 to 0.45 with step size of 0.05; Cost-Dependent analysis). Graph metrics computed include global metrics (efficiency, modularity, transitivity) and nodal metrics (clustering coefficient, nodal efficiency, participation coefficient). Mixed-effects GLM analyses (due to the different values of cost) with an unstructured correlation matrix were performed with CHD status the independent variable; sex, PCA at birth, PCA at scan, voxel size, multi-band parameter, and scanner covariates of no interest; and graph metric the dependent variable. FDR correction was used for nodal metrics to correct for multiple comparisons across nodes. The analyses were repeated investigating sex-by-CHD interactions.
Results
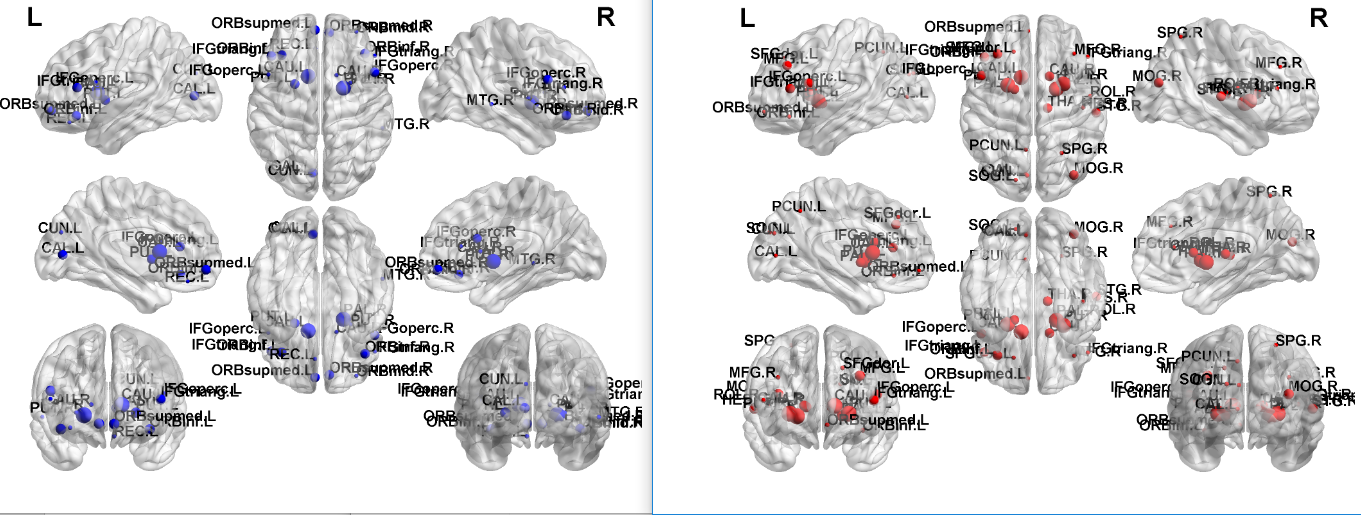
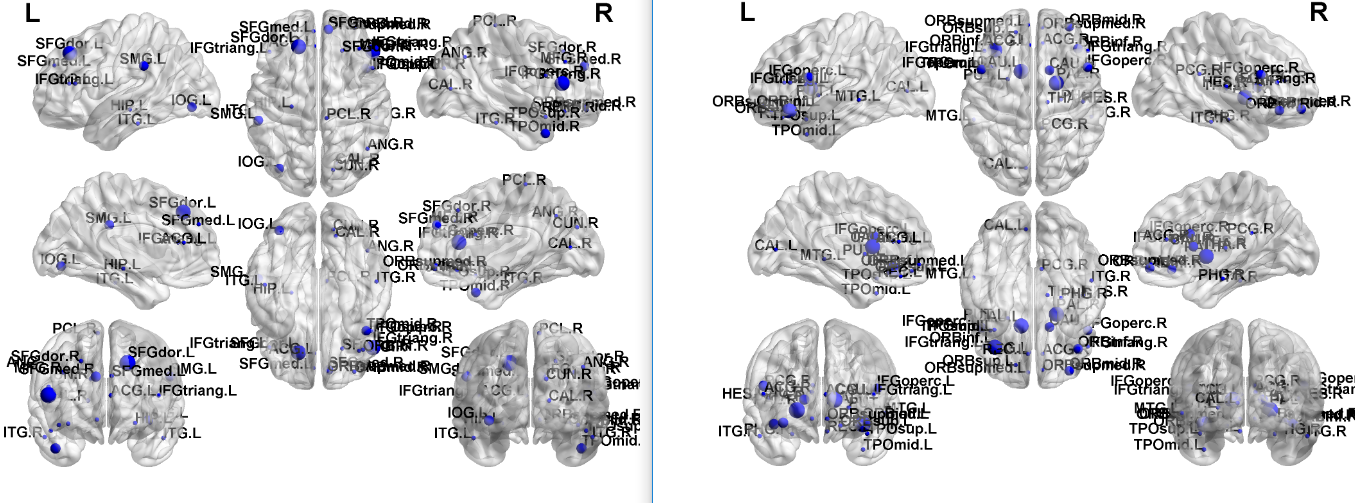
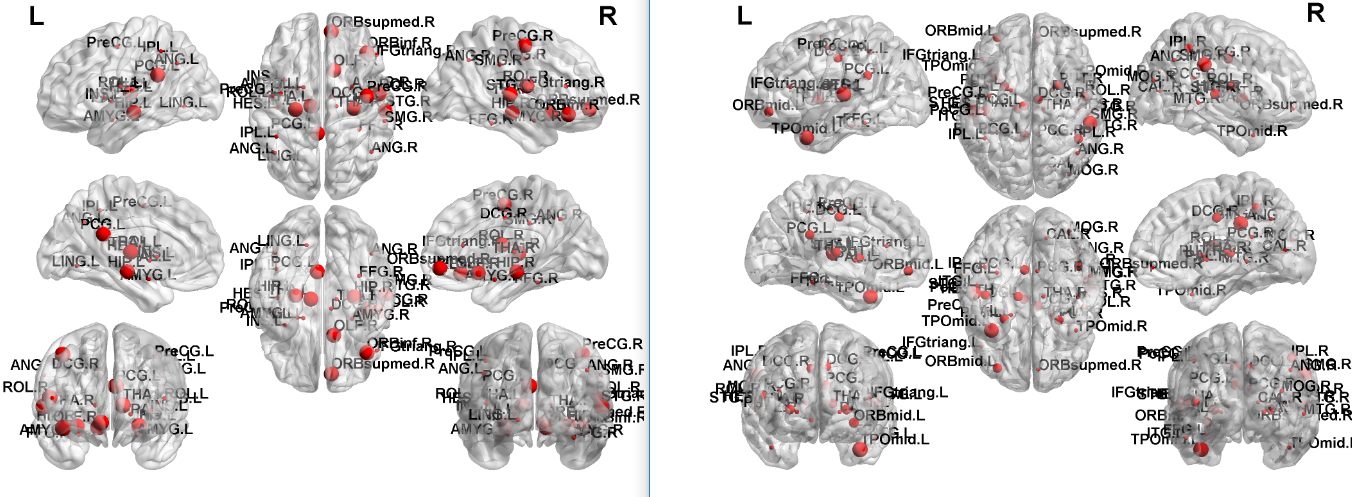
Cost-Independent: CHD infants display reduced modularity (p < 0.001) and transitivity (p < 0.05) as well as reduced clustering coefficient and increased participation coefficient (Figure 1) mainly in subcortical and frontal regions, indicating overall reduced segregation compared to normal controls. No significant sex-by-CHD interactions were found.Cost-Dependent: CHD infants display reduced global efficiency (p < 0.05) and transitivity (p < 0.05) as well as reduced nodal efficiency and reduced clustering coefficient (Figure 2) mainly in subcortical, frontal and temporal regions, indicating reduced integration and segregation compared to controls. Significant sex-by-CHD interactions (M > F) were seen for global efficiency (p < 0.05), nodal efficiency and clustering coefficient (Figure 3) again mainly in subcortical, frontal, and temporal regions.
Discussion
Results confirm brain dysmaturation in CHD infants impacts functional network topology, with reduced integration and segregation, particularly in subcortical and frontal regions, which may be related to the later risk of adverse neurocognitive outcome. However, results from the cost-dependent analysis indicate that this effect is reduced in boys compared to girls, which may indicate a differential risk between boys and girls regarding neurocognitive outcome. On the other hand, no significant sex-X-CHD interactions were found for the cost-independent analysis, indicating that some functional network topology differences are found equally in girls and boys.Metrics computed for the cost-dependent analysis are highly correlated with overall network cost and global efficiency and are thus a “coarser” indicator of network topology. The effects of overall cost are removed in the cost-independent analysis and are thus representative of topology at a finer or subtler level. Thus, boys may be able to compensate for the effects of CHD on the developing brain at a coarser but not at a finer level of functional topology. Further research associating brain functional topology in infancy with later neurocognitive outcome will be necessary to investigate this hypothesis further, as well as its possible association with genetic factors and/or impaired substrate delivery in utero.
Conclusion
CHD neonates show reduced functional integration and segregation compared to normal controls, both globally and nodally particularly in subcortical and frontal regions. Sex-by-CHD interactions (M > F) were found however for the cost-dependent analysis, indicating that part of this effect is reduced in boys compared to girls, which may differentially impact later neurocognitive development.Acknowledgements
No acknowledgement found.References
1. Marelli A, Miller SP, Marino BS, Jefferson AL, Newburger JW. The Brain in Congenital Heart Disease Across the Lifespan: The Cumulative Burden of Injury. Circulation 2016; 133(20): 1951-1962.
2. Leonetti C, Back SA Gallo V, Ishibashi N. Cortical Dysmaturation in Congenital Heart Disease. Trends Neurosci 2019; 42(3): 192-204.
3. Power JD, Mitra A, Laumann TO, Snyder AZ, Schlaggar BL, Petersen SE. Methods to detect, characterize, and remove motion artifact in resting state fmri. NeuroImage. 2014; 84: 320-341.
4. Shi F, Yap P-T, Wu G, Jia H, Gilmore JH, Lin W, Shen D. Infant Brain Atlases from Neonates to 1- and 2-Year Olds. PLoS ONE 2011; 6(4): e18746.
Figures