4610
Non-invasive cardiac magnetic resonance blood oxygenation mapping in complex congenital heart disease1Northwestern University Feinberg School of Medicine, Chicago, IL, United States, 2Lurie Children's Hospital of Chicago, Chicago, IL, United States, 3Ohio State University, Columbus, OH, United States
Synopsis
Cardiac magnetic resonance (CMR) can be utilized for non-invasive estimation of blood oxygen (O2) saturation in complex pediatric heart disease (i.e., single ventricle physiology) with good correlation to current gold standard catheter-derived measurements. Oximetry maps derived from T2 CMR data can enhance visualization of regional O2 saturations and may guide optimization of image acquisition and analysis.
Introduction
Non-invasive estimation of blood oxygen (O2) saturation by cardiac magnetic resonance (CMR) has clinical application in complex congenital heart disease – particularly single ventricle physiology. These lesions require palliative surgeries and life-long follow-up for residual defects leading to complications such as unexplained cyanosis. A T2-mapping based, non-linear, multi-parameter method has been described to non-invasively determine O2 saturation in the heart and great vessels in specific regions of interest.1 This study builds on our prior validation of “oximetry maps” in adults and children with predominantly structurally normal hearts to attempt visualization of O2 saturations within the heart and surrounding vasculature and determine optimal regions for evaluation in complex pediatric structural heart disease.Methods
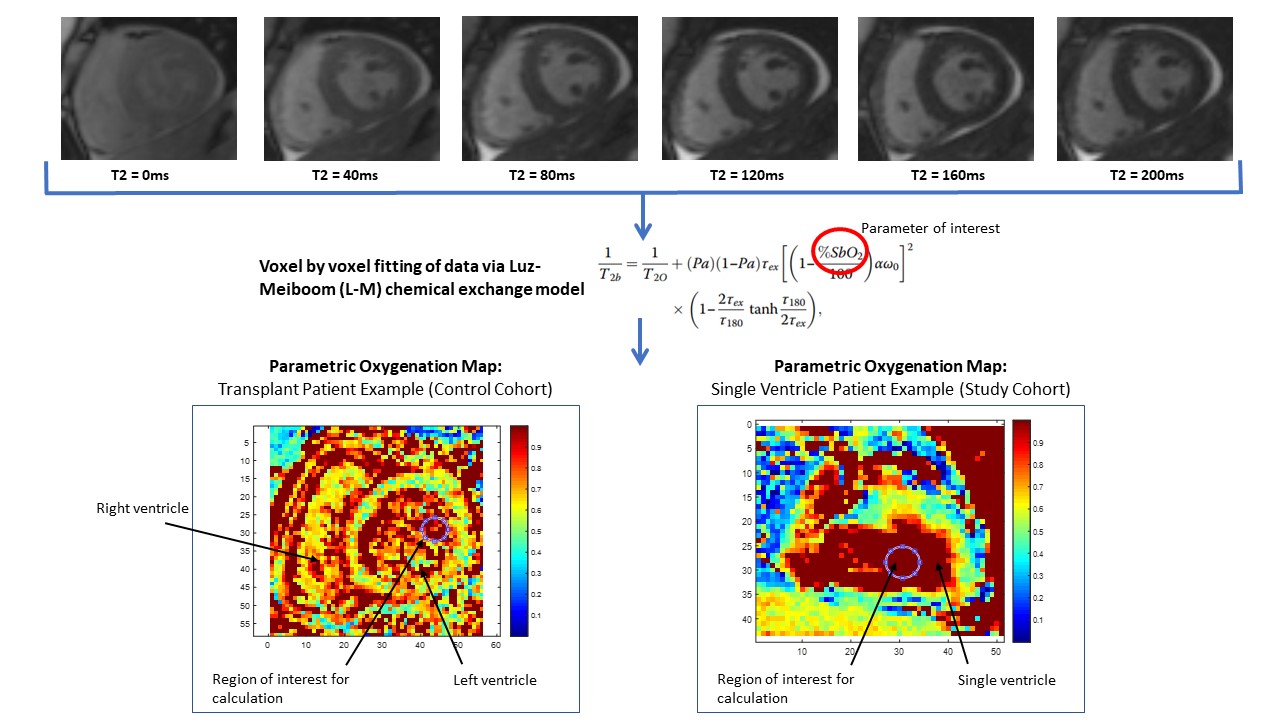
8 patients (mean age: 17.1 ± 8.7 years, 3 female) with single ventricle physiology undergoing clinically indicated cardiac catheterization and CMR were recruited in a single tertiary care children’s hospital and compared against a control cohort of patients with structurally normal transplanted hearts (n=7 patients, mean age: 15.6 ± 6.5 years, 3 female). For each patient, a series of T2-prepared single-shot steady-state free-precession (SSFP) images were acquired in free-breathing, across T2-preparation (T2p) times ranging from 0 to 200 ms (Figure 1). The corresponding inter-echo spacing (τ) ranged from 0 to 25 ms. Images were acquired in multiple planes depending on the patient’s diagnosis. Data analysis included calculation of color coded maps representing estimated O2 saturations based on voxel-wise fitting of the T2 data to the Luz-Meiboom model (S, T, τ, and α). Regional O2 saturation based on oximetry maps were compared to corresponding invasive catheterization results.Results
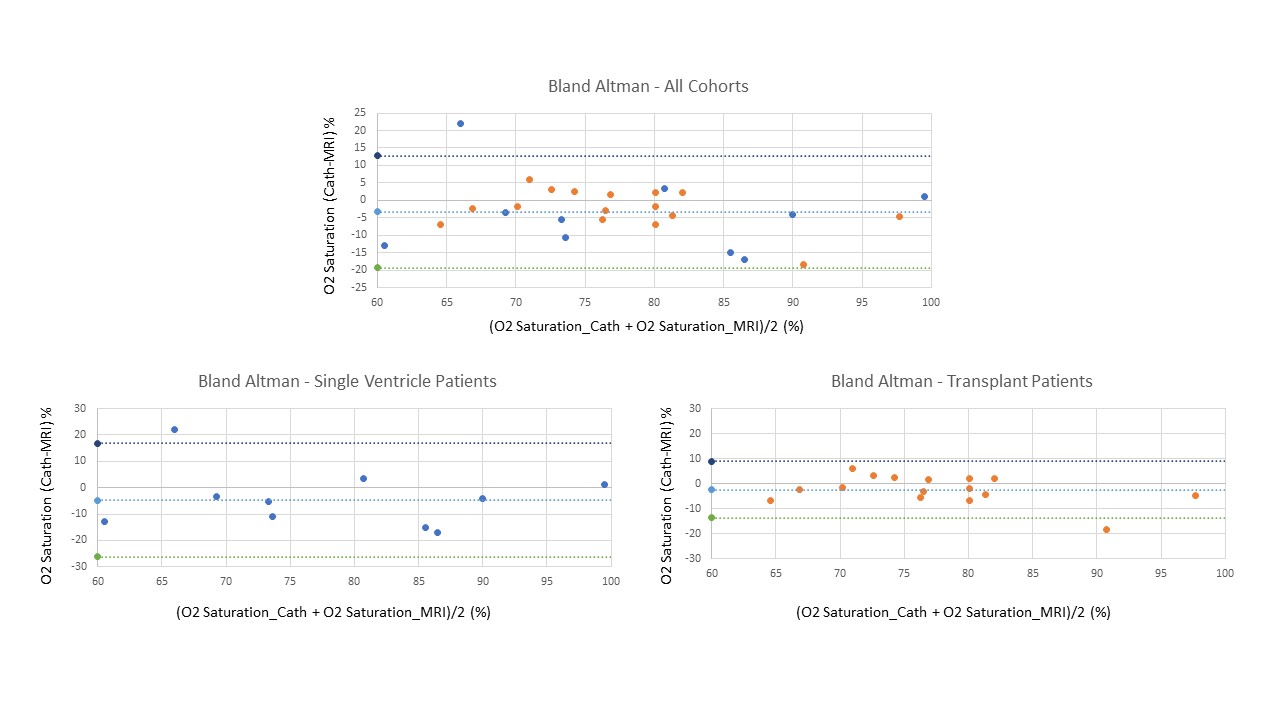
Oximetry maps allowed for visualization of O2 saturations to identify regions with uniform blood pools and appreciate regions of heterogenous local O2 saturations (Figure 2). Correlation between saturations measured via oximetry maps and catheterization were favorable overall (r=0.73, p<0.001) as well as specifically in single ventricle patients (r=0.70, p=0.02) and structurally normal transplant patients (r=0.81, p<0.001). Bland Altman plots in Figure 3 comparing MRI-derived estimates against catheter measurements demonstrated reasonable agreement of CMR map derived regional O2 saturations compared to catheterization overall (mean difference= -3.3, limits of agreement= -19.4,12.7), in single ventricle patients (mean difference=-4.8, limits of agreement=-26.3,16.8) and in structurally normal transplant patients (mean difference=-2.4, limits of agreement -13.7, 8.96).Discussion
CMR estimates demonstrated acceptable correlation with the clinical gold standard of cardiac catheterization in pediatric patients with complex congenital heart disease but with less favorable limits of agreement compared to patients with structurally normal hearts. Typically during catheterization, point blood gas samples from select cardiac chambers and vessels are obtained and extrapolated to estimate O2 saturations in the remaining heart and vasculature based on presumed hemodynamics while ignoring streaming effects. “Streaming effects,” are non-uniform local differences in blood flow that occur in anatomically complex palliative cardiac repairs and can result in heterogeneous local O2 saturations.2,3 Comparison of regional blood pool analysis to cardiac catheterization does not take into account streaming effects in human hearts altered by palliation surgeries and may explain why oximetry maps visually depicted heterogenous local saturations in these patients.Conclusion
Oximetry maps aim to further develop the ability for CMR to estimate intracardiac and vascular blood O2 saturations in complex congenital heart disease. Ongoing patient recruitment is warranted to further optimize image acquisition and analysis and potentially enhance visualization of streaming effects of oxygenated and deoxygenated blood.Acknowledgements
NoneReferences
1. Varghese J, Potter LC, LaFountain R, et al. CMR-based blood oximetry via multi-parametric estimation using multiple T2 measurements. J Cardiovasc Magn Reson. 2017;19:88.
2. Jarvis K, Schnell S, Barker AJ, et al. Evaluation of blood flow distribution asymmetry and vascular geometry in patients with Fontan circulation using 4-D flow MRI. Pediatr Radiol. 2016;46(11):1507-19.
3. Klimes K, Abdul-Khaliq H, Ovroutski S, et al. Pulmonary and caval blood flow patterns in patients with intracardiac and extracardiac Fontan: a magnetic resonance study. Clin Res Cardiol. 2007;96(3):160-7.
Figures