4608
Wide-spread Reduced Cerebral Blood Flow in Patients with Right Ventricle Compared to Left Ventricle Single Ventricle Heart Disease1Anesthesiology, University of California at Los Angeles, Los Angeles, CA, United States, 2Radiology, University of California at Los Angeles, Los Angeles, CA, United States, 3Bioengineering, University of California at Los Angeles, Los Angeles, CA, United States, 4Brain Research Institute, University of California at Los Angeles, Los Angeles, CA, United States, 5Neurology, University of Southern California, Los Angeles, CA, United States, 6Division of Pediatric Cardiology, University of California at Los Angeles, Los Angeles, CA, United States, 7Division of Pediatric Cardiology, Children's Hospital of Los Angeles, Los Angeles, CA, United States, 8UCLA School of Nursing, University of California at Los Angeles, Los Angeles, CA, United States, 9Radiology, University of Southern California, Los Angeles, CA, United States
Synopsis
Single ventricle heart disease (SVHD) presents with either a dominant single right ventricle (RV) or left ventricle (LV). Individuals with RV dominant SVHD show worse outcomes, including worse cognition and quality of life, which may result from decreased cardiac output due to differences in ventricular size, shape, and function or other structural related sequela, contributing to regional cerebral blood flow (CBF) changes. We examined CBF changes between RV and LV over controls, and found more wide-spread changes in RV over LV. These findings indicate that worse outcomes in RV SVHD may result from compromised CBF over LV SVHD.
Introduction
Single ventricle heart disease (SVHD) patients may be characterized as either a dominant single right ventricle (RV) or left ventricle (LV).1-3 Individuals with RV dominant SVHD show worse outcomes, including lower cognition, increased morbidity and mortality, need for transplantation, and reduced quality of life compared to adolescents with LV SVHD. Differences in size, shape, and systolic and diastolic function between morphologic types may cause decreased cardiac output, particularly in RV SVHD. However, whether such variations in cardiac output or morphologic types could lead to alterations in regional brain cerebral blood flow (CBF), contributing to tissue changes and functional deficits, are unclear. Regional brain CBF can be assessed by magnetic resonance imaging (MRI) based arterial spin labeling (ASL) imaging procedures. ASL imaging is a non-invasive approach, without use of radiation or contrast agents, for assessment of regional brain perfusion changes. ASL-based CBF values have been validated with positron emission tomography, and shown to be reproducible, making it favorable for CBF evaluation, and thus, is useful in regional CBF assessment in SVHD. However, this technique has not been used in the evaluation of CBF and brain changes in SVHD based on ventricle type. Our aim was to examine regional CBF changes between RV and LV SVHD compared to control subjects using the ASL procedures.Materials and Methods
Fourteen adolescents with RV SVHD (age 16.1±1.5 years; BMI, 21.7±3.6 kg/m2; 7 male), 6 LV SVHD (age, 16.3±1.0 years; BMI, 24.7±7.3 kg/m2; 4 male), and 25 healthy controls (age, 15.9±1.4 years; BMI, 23.3±5.1 kg/m2; 13 male) were studied. SVHD subjects, who have undergone surgical palliation with Fontan completion, were recruited via flyers or referrals from pediatric cardiology clinics, and private practice cardiology groups. Control subjects were healthy, without any history of chronic medical or psychiatric conditions or head injury, and were recruited from the community. All procedures were approved by the Institutional Review Boards and each subject provided written informed consent prior to the study. Brain MRI studies were performed using a 3.0-Tesla MRI scanner (Magnetom Prisma, Siemens, Erlangen, Germany). 3D pseudo-continuous ASL [pCASL] (TR = 4,000 ms, TE = 36.7 ms, FA = 120°, bandwidth = 2365 Hz/pixel, matrix size = 96´96, FOV = 240´240 mm, slice thickness = 2.5 mm) data were collected. Using labeled and non-labeled ASL brain volumes, perfusion images were computed and whole-brain CBF maps were generated. These maps were normalized to a common space, smoothed, and voxel-by-voxel CBF changes were assessed between RV SVHD and controls and LV SVHD and controls (SPM12 software; ANCOVA; covariates, age and sex; p<0.005]. Control sites to calculate effect sizes. Brain clusters with significant differences between groups were overlaid onto background images for structural identification.Results
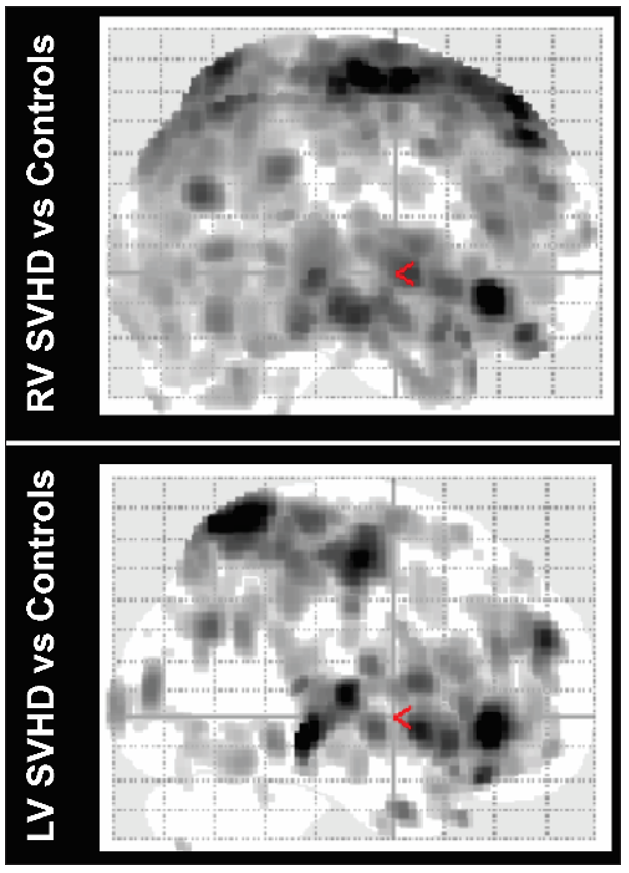
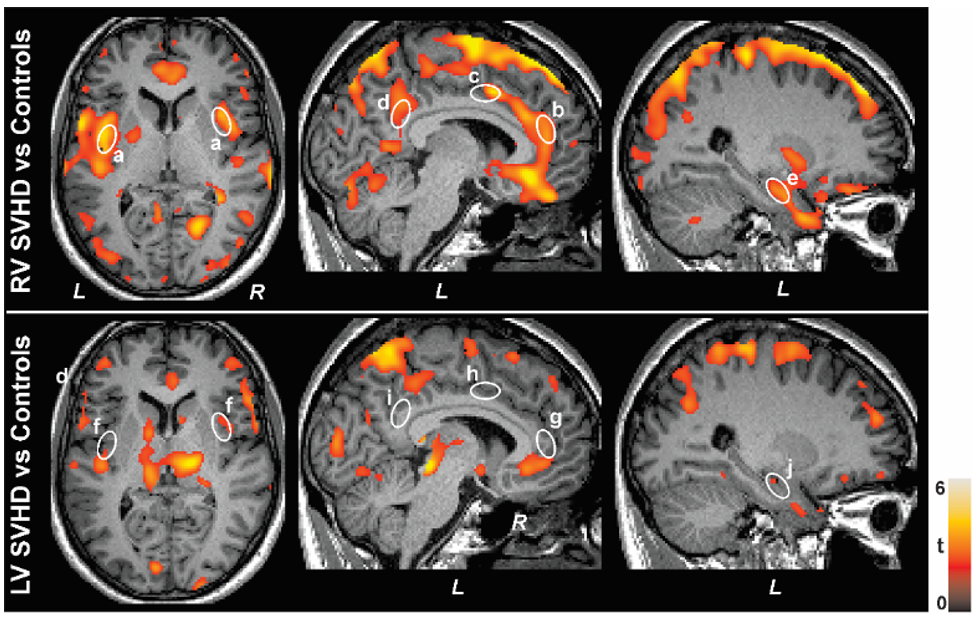
Regional brain CBF was largely reduced in RV over LV SVHD (Fig. 1). Whole-brain voxel-based analyses showed multiple brain sites with more widespread reduced CBF values in RV over LV SVHD compared to controls (Fig. 2, p<0.005), including the prefrontal cortices, caudate, insula (a, f), anterior (b, g), mid (c, h), and posterior (d, i) cingulate, and hippocampus (e, j).Discussion
SVHD adolescents with a dominant RV showed more widespread reduced CBF than single LV in cognitive and mood regulatory sites, which may result from variable cardiac output between ventricle types or other structural related sequela contributing to variable hemodynamics. The findings indicate that the therapeutic approach should be cognizant of the differences in CBF based on ventricle type and investigate interventions to optimize CBF in RV SVHD.Conclusions
The findings indicate that variable regional CBF changes occur between RV and LV SVHD adolescents after staged surgical palliation in multiple cognitive and mood control areas, which can be assessed with non-invasive ASL procedures.Acknowledgements
This work was supported by National Institutes of Health R01-NR016463.References
1. Pike NA, Roy B, Gupta R, Singh S, Woo MA, Halnon NJ, Lewis AB, Kumar R: Brain abnormalities in cognition, anxiety, and depression regulatory regions in adolescents with single ventricle heart disease. J Neurosci Res 2018, 96(6):1104-1118.
2. Singh S, Kumar R, Roy B, Woo MA, Lewis A, Halnon N, Pike N: Regional brain gray matter changes in adolescents with single ventricle heart disease. Neurosci Lett 2018, 665:156-162.
3. Singh S, Roy B, Pike N, Daniel E, Ehlert L, Lewis AB, Halnon N, Woo MA, Kumar R: Altered brain diffusion tensor imaging indices in adolescents with the Fontan palliation. Neuroradiology 2019, 61(7):811-824.
Figures