4606
Assessment of Right Ventricular Systolic Abnormalities in Pediatric Repaired TOF Patients with Preserved EF: CMR Feature Tracking Analysis1Shanghai Children's Medical Center, Shanghai Jiaotong University School of Medicine, Shanghai, China, 2National Heart Centre Singapore, Singapore, Singapore, 3GE Healthcare, Shanghai, China, 4Duke-NUS Medical School, National University of Singapore, Singapore, Singapore
Synopsis
Right ventricular (RV) ejection fraction (EF) <45% is insensitive for detecting systolic dysfunction due to pulmonary regurgitation after Tetralogy of Fallot repair (rTOF). In pediatric rTOF patients with RVEF≥45% and healthy controls, CMR feature tracking was used to assess RV systolic strains and displacement as well as systolic and diastolic myocardial velocities. We observed abnormal RV global longitudinal strain and myocardial velocities in rTOF despite normal RVEF. 78% and 75% of rTOF patients had tricuspid annular displacement systolic excursion <10.9 mm and peak systolic myocardial velocity <6.3cm/s (lower normal limits among controls), respectively, indicating high prevalence of systolic functional impairment.
Introduction
Right ventricular (RV) volume overload from residual pulmonary regurgitation in patients after repair of tetralogy of Fallot (rTOF) is associated with adverse outcome. RV systolic dysfunction assessment is necessary for optimal timing of intervention (pulmonary valve replacement). RV ejection fraction (EF) of <45% is an insensitive threshold to identify systolic functional impairment. We hypothesized that early systolic abnormalities precede RVEF deterioration in rTOF patients. Therefore, the aim of this study was to compare RV strains, myocardial displacement and velocities in rTOF with preserved RVEF ≥45% versus control using cardiac magnetic resonance (CMR) feature tracking 2,3.Materials and Methods
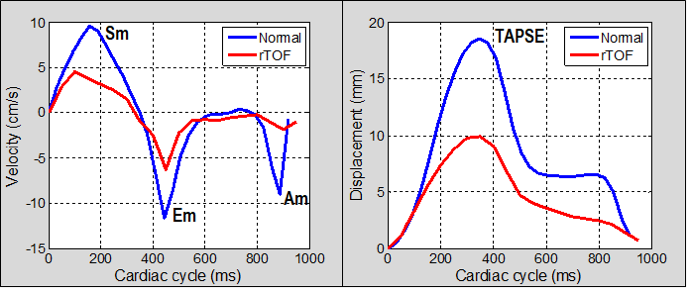
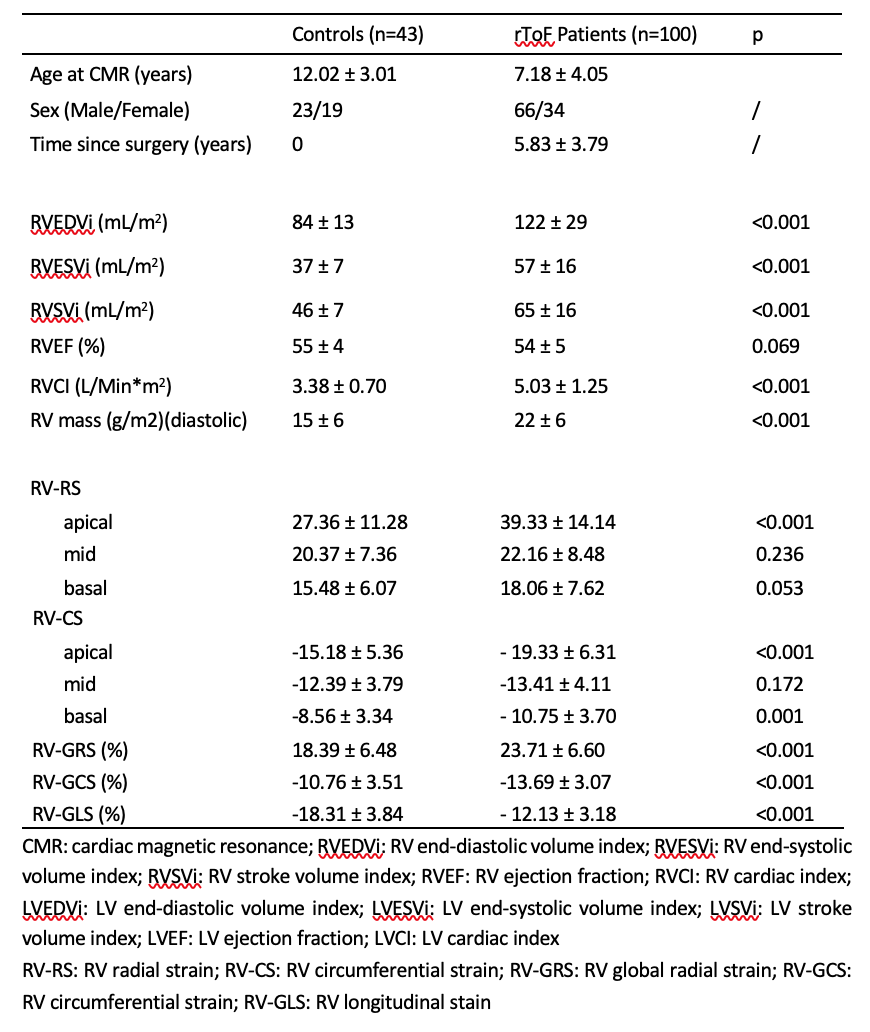
100 pediatric rTOF patients with preserved RVEF ≥45% and 43 healthy controls were recruited. All underwent steady-state free precession cine CMR on a 3.0T scanner (MR750, GE Healthcare, Waukesha). Volumetric analysis for bi-ventricular volumes, myocardial mass and ejection fraction and feature tracking for RV radial (RV-RS), circumferential (RV-CS) and longitudinal (RV-LS) strains were performed using CVI42 software (Circle Cardiovascular Imaging, Calgary). A software created on MATLAB (MathWorks Inc., MA) was used to track tricuspid annular (TA) motion semi-automatically in multiple RV long-axis planes to measure TA plane systolic excursion (TAPSE), peak systolic (Sm), early diastolic (Em) and late diastolic myocardial velocities (Am) 1-3 (Fig 1).Results
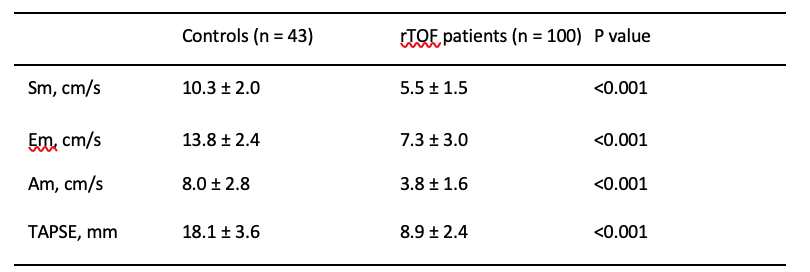
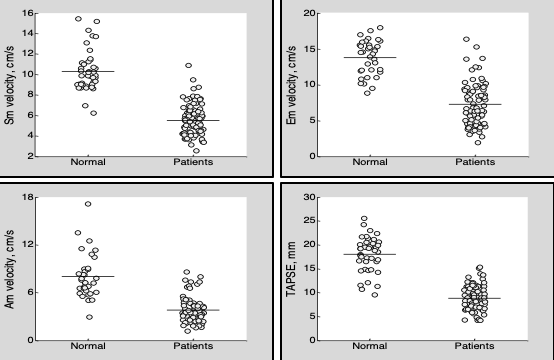
RV volumes, mass and cardiac index were significantly higher in rTOF versus controls (Fig 2). RV global radial (GRS) and circumferential strains (GCS) were significantly higher, and global longitudinal strain (GLS) lower, versus controls (Fig 2 and 3). All TA myocardial velocities (Sm: 5.5±1.5 vs 10.3±2.0 cm/s; Em: 7.3±3.0 vs 13.7±2.4 cm/s; Am: 3.8±1.6 vs 8.0±2.8 cm/s) and TAPSE (8.9±2.4 vs 18.1±3.6 mm) were significantly lower than controls (Figs 4 and 5). The lower limits (-2 standard deviations) of systolic parameters Sm and TAPSE among controls were 6.3 cm/s and 10.9 mm, respectively. Among rTOF patients, 75% had Sm < 6.3 cm/s and 78% had TAPSE < 10.9 mm.Conclusion
Among pediatric rTOF patients with preserved RVEF ≥45%, RV GLS was significantly decreased, whereas GRS and GCS exhibited directionally opposite changes, possibly as compensation for reduced RV GLS. Despite normal RVEF, there was high prevalence of systolic functional impairment that coexists with diastolic dysfunction in pediatric rTOF patients. CMR feature tracking may be used to detect subtle systolic and diastolic perturbations early after rTOF.Acknowledgements
No acknowledgement found.References
1. Leng S, et al. Am J Physiol Heart Circ Physiol 2015;309(11):H1923-H1935.
2. Leng S et al. Ann Biomed Eng 2016;44:3522-3538.
3. Leng S et al. Circulation Cardiovasc Imaging 2019;12:e008582.
Figures