4605
Right and Left Ventricular Volume Quantification in Children with repaired Tetralogy of Fallot Using 4D Flow MRI1Shanghai Children's Medical Center, Shanghai, China, 2GE Healthcare, Shanghai, China
Synopsis
4D flow CMR has been used to assess right and left ventricular function with increasing attention. We hypothesis that the results of right and left ventricular volume quantification using 4D flow has the same accuracy compared to that with 2D b-SSFP cine sequence in children with repaired Tetralogy of Fallot (r-TOF).
Introduction
Congenital heart disease is the most common birth defect in China, and Tetralogy of Fallot (TOF) is the most common cyanotic congenital heart disease. There was pulmonary valve regurgitation after operation of Tetralogy of Fallot, which would lead to the enlargement of right ventricle and the decrease of cardiac function. To our knowledge, right and left volume quantification with 4D flow of repaired Tetralogy of Fallot has rarely been reported. In this study, our aim was to compare the results of right and left ventricular volume between 2D b-SSFP cine and 4D flow. To assess the accuracy of 4D flow ventricular volume quantification in children with r-TOF.Methods
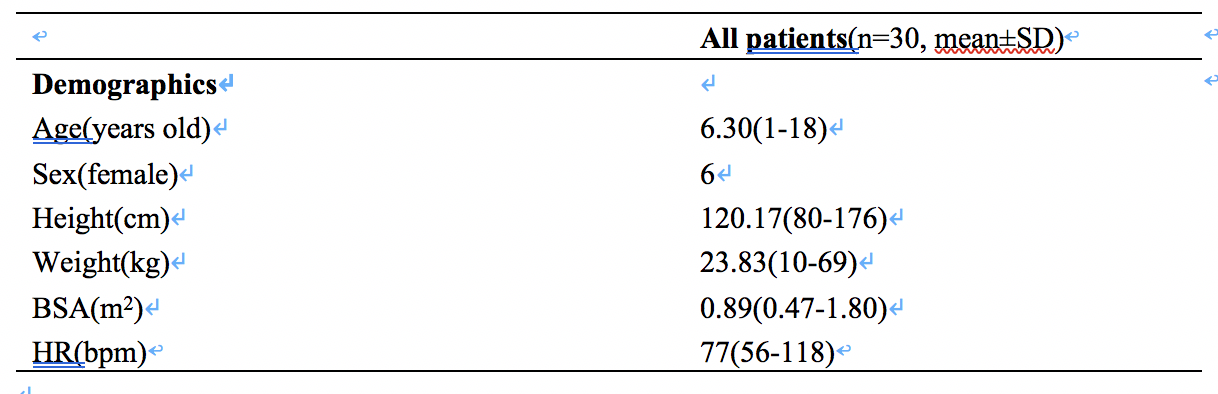
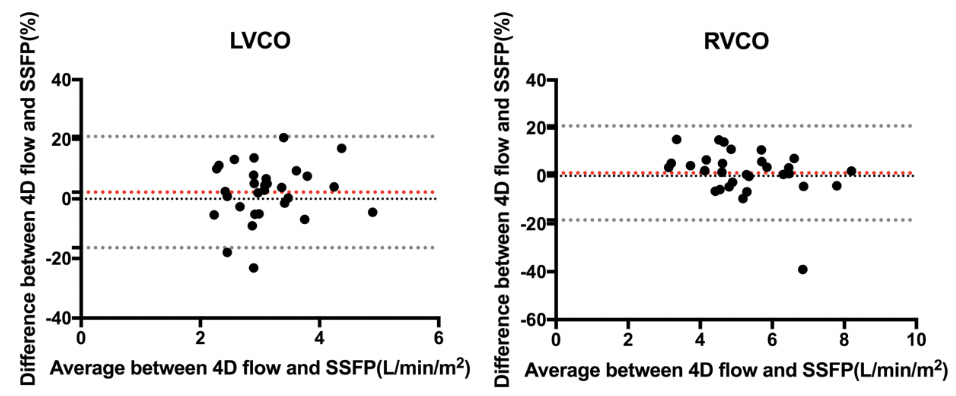
With the approval of Ethics Committee, we retrospectively identified contiguous repaired Tetralogy of Fallot children patients referred for cardiac MRI in our hospital. We included thirty pediatric patients (6 females, mean age 6.30 years) with r-TOF who underwent the 2D short-axis and the long-axis b-SSFP cine and the 4D Flow MRI from September 2018 to September 2019. 4D flow and 2D SSFP were acquired using 3.0 Tesla (Discovery MR 750, GE, USA) scanner with an eight-channel phased-array cardiac coil. The 4D flow data sets were uploaded to Arterys MICA’s online service(Arterys Inc, San Francisco, USA), which was accessed via the Internet. 2D SSFP volumetric parameters were measured by Circle Cardiovascular Imaging software (Cvi42, Calgary, Canada). The end-diastolic, end-systolic, stroke volumes, ejection fraction and cardiac output of left ventricle and right ventricle were measured by 4D flow and were compared with 2D SSFP cine. Statistical analysis was performed by SPSS 25.0 software (SPSS, Chicago, IL, USA), and a significance level of 0.05 was applied for all statistical test. Agreement of SSFP and 4D flow was assessed first using Bland-Altman analysis (mean difference between measurements with 95% confidence interval (CI)). To test the correlation of the results between 4D flow and 2D SSFP, Spearmen tests were used for nonparametric correlation test.Results
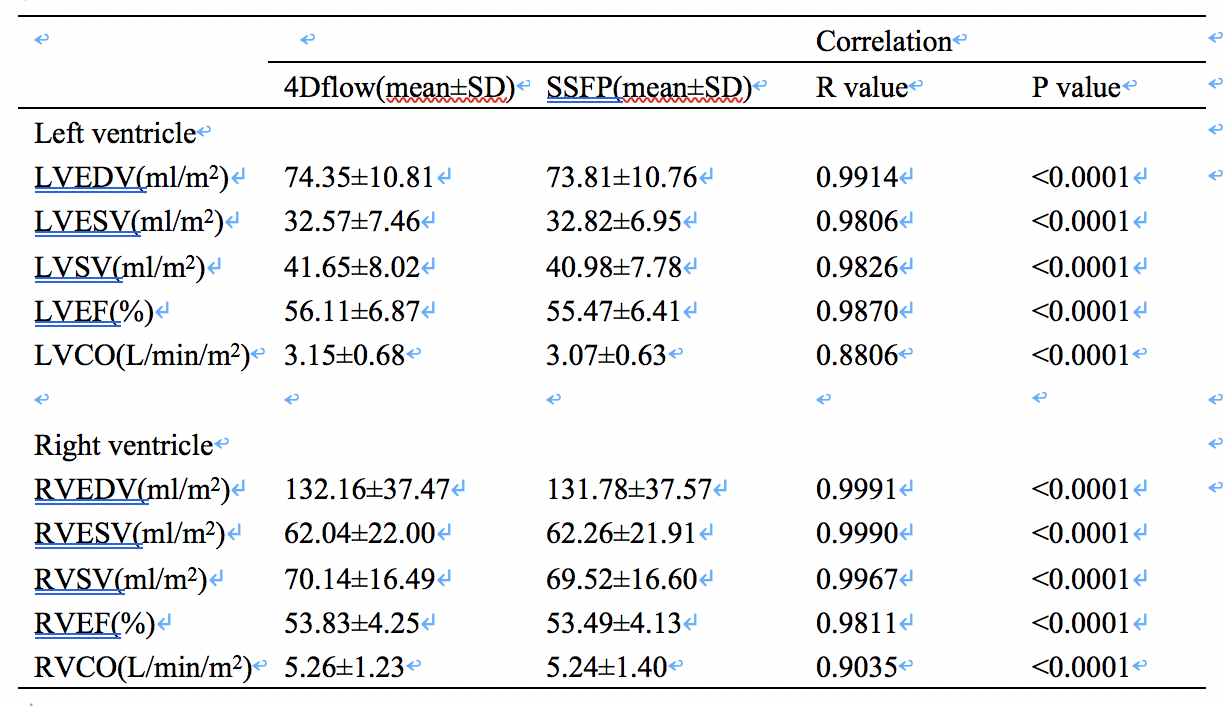
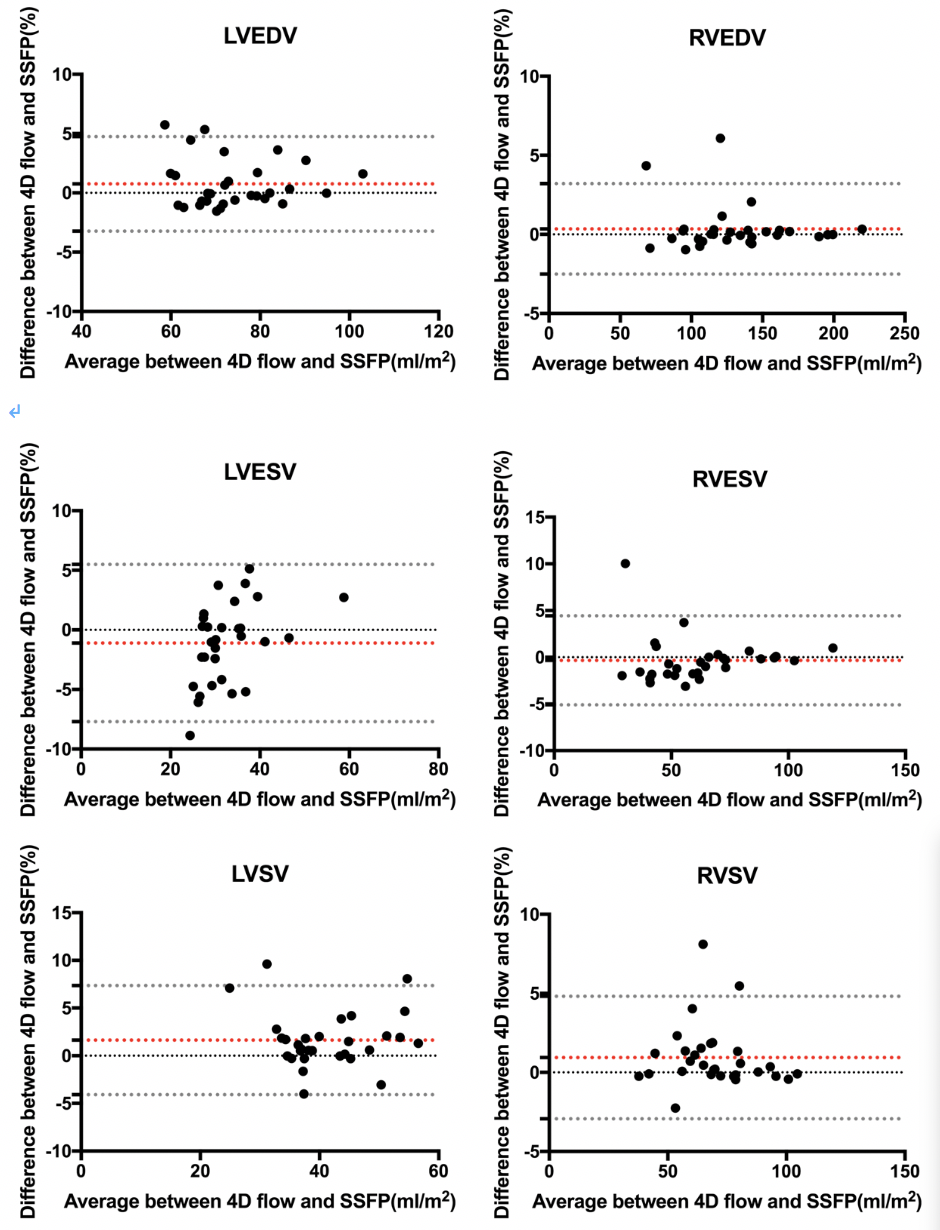
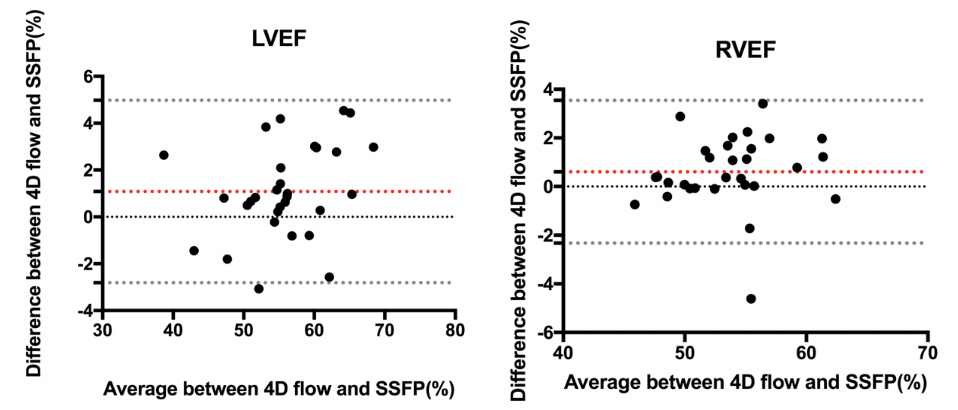
In our study, all 30 cases were repaired Tetralogy of Fallot. The mean end-diastolic, end-systolic, stroke volume, EF and cardiac output of right and left ventricle were shown in the table 2 for 2D SSFP and 4D flow. There was no difference in heart rate between 4D flow and SSFP acquisitions (77.03±13.30 vs. 76.47±12.45 bpm, p=0.881).Right and left ventricular Bland-Altman relative limits of agreement were between -7.705% to 7.354% for ventricular volumes, -2.812% to 4.977% for EF, and -21.64% to 26.41% for CO. There was no significant difference of cardiac output between 4D flow and SSFP for the LV(p=0.1153) or RV(p=0.8443).Significant biventricular correlation were shown between 4D flow and SSFP for both ventricular volumes(r=0.9806-0.9991,p<0.0001),ejection fraction(EF)(r=0.9811-0.9870, p<0.0001) and cardiac fraction (CO)(r=0.8806-0.9035, p<0.0001).Conclusions
Right and left ventricular end-diastolic, end-systolic and stroke volumes in congenital heart disease can be measured accurately by 4D flow CMR, which were compared with 2D b-SSFP cine. 4D flow CMR not only provide flow information of congenital heart disease also can assess cardiac function.Acknowledgements
NoneReferences
1. Cheng J Y, Hanneman K, Zhang T, Alley M T, Lai P, Tamir J I, Uecker M, Pauly J M, Lustig M, Vasanawala S S. Comprehensive motion-compensated highly accelerated 4D flow MRI with ferumoxytol enhancement for pediatric congenital heart disease: Mo-tion-Compensated Accelerated 4D Flow[J]. Journal of Magnetic Resonance Imaging, 2016, 43(6): 1355–1368.
2. Hsiao A, Lustig M, Alley M T, Murphy M, Chan F P, Herfkens R J, Vasanawala S S. Rapid Pediatric Cardiac Assessment of Flow and Ventricular Volume With Compressed Sensing Parallel Imaging Volumetric Cine Phase-Contrast MRI[J]. American Journal of Roentgenology, 2012, 198(3): W250–W259.
3. Bock J, Frydrychowicz A, Stalder A F, Bley T A, Burkhardt H, Hennig J, Markl M. 4D phase contrast MRI at 3 T: Effect of standard and blood-pool contrast agents on SNR, PC-MRA, and blood flow visualization[J]. Magnetic Resonance in Medicine, 2010, 63(2): 330–338.
4. Zhong L, Schrauben E M, Garcia J, Uribe S, Grieve S M, Elbaz M S M, Barker A J, Geiger J, Nordmeyer S, Marsden A, Carlsson M, Tan R, Garg P, Westenberg J J M, Markl M, Ebbers T. Intracardiac 4D Flow MRI in Congenital Heart Disease: Recommendations on Behalf of the ISMRM Flow & Motion Study Group[J]. Journal of Magnetic Resonance Imaging, 2019.
5. Dyverfeldt P, Bissell M, Barker A J, Bolger A F, Carlhäll C-J, Ebbers T, Francios C J, Frydrychowicz A, Geiger J, Giese D, Hope M D, Kilner P J, Kozerke S, Myerson S, Neubauer S, Wieben O, Markl M. 4D flow cardiovascular magnetic resonance consensus statement[J]. Journal of Cardiovascular Magnetic Resonance, 2015, 17(1). 6. Hanneman K, Kino A, Cheng J Y, Alley M T, Vasanawala S S. Assessment of the precision and reproducibility of ventricular volume, function, and mass measurements with ferumoxytol-enhanced 4D flow MRI: 4D Flow MRI Assessment of Ventricular Mass[J]. Journal of Magnetic Resonance Imaging, 2016, 44(2): 383–392.
Figures