4576
Fetal cardiac magnetic resonance imaging (FCMR); MR sequences, cardiac & non-cardiovascular findings with prenatal and postnatal correlation
Dianna M. E. Bardo1, Christopher Lindblade2, Fidaa Wishah1, Patricia Cornejo1, Jennifer Vaughn1, Mittun Patel1, and Luis Goncalves1
1Radiology, Phoenix Children's Hospital, Phoenix, AZ, United States, 2Cardiology, Phoenix Children's Hospital, Phoenix, AZ, United States
1Radiology, Phoenix Children's Hospital, Phoenix, AZ, United States, 2Cardiology, Phoenix Children's Hospital, Phoenix, AZ, United States
Synopsis
Fetal MRI is a not uncommon imaging procedure, most often performed to diagnose neurologic abnormalities. Increasingly fetal cardiac MRI is performed to confirm CHD findings found on fetal echocardiography and associated non-cardiovascular anomalies, especially in mid-to-late gestation fetuses.
This educational exhibit will provide guidance for image acquisition and show an extensive multi-modality case based library of fetal cardiac images, highlighting MRI findings, with correlation to postnatal imaging.
Purpose
The purpose of this educational exhibit is to show FCMR images of congenital heart disease (CHD) and anatomical findings associated with CHD. We will describe currently available FCMR image acquisition techniques and use a case-based approach to show a variety of CHD diagnosis and non-cardiovascular associations on fetal MRI, along with correlation to fetal echocardiography, prenatal ultrasound, and postnatal imaging. Teaching points to highlight the added value of FCMR in diagnosis and prognosis will be added.Materials and Methods
50 fetuses, 21 4/7-38 weeks gestation with known, suspected and unknown diagnoses of CHD underwent FCMR either for confirmation of cardiac findings and/or for diagnosis of associated fetal anomalies, including neurological, renal, pulmonary or musculoskeletal systems.FCMR was performed using a pseudo ECG-gating technique to generate an artificial ECG trace to enable steady state free precession images of the heart in coronal, sagittal and axial planes. We will describe other techniques currently available, Doppler US and integrated ECG methods.
FCMR findings will be shown along with correlative fetal echo and postnatal echo, cardiac MR and cardiac CTA images.
Results
65 CHD diagnoses made with FCMR included hypoplastic left heart syndrome (10), ventricular septal defect (9), anomalous pulmonary veins (7), transposition of the great arteries (4), tetralogy of Fallot (3), and double outlet right ventricle (2). Fetal MR revealed additional important anatomical findings in fetuses with CHD including abnormalities of the pulmonary parenchyma, bronchi, abdominal visceral situs, intracranial abnormalities (brain malformations, stroke, ventriculomegaly) and skeletal dysplasia.Conclusion
FCMR is an important diagnostic tool used to confirm or clarify the diagnosis of CHD which is most often initially made with echo. Fetal MR is known to be a highly sensitive and specific method for identification of non-cardiac imaging findings associated with CHD. Early knowledge of severity of and complexity of CHD and accompanying anomalies enables guidance for delivery planning and immediate postnatal care and opportunities for possible genetic counseling for parents.Acknowledgements
References
Figures
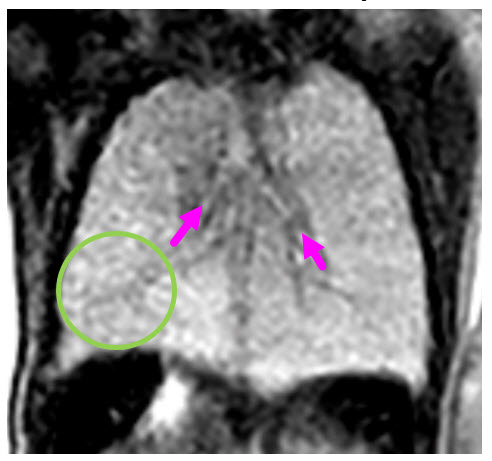
At 29
gestational weeks coronal fetal T2 weighted view of the chest shows large lung
volume with coarse, ‘nutmeg’ appearance which is indicative of lymphangiectasia (green circle) and bilateral morphologically R main bronchi (pink arrows). Lymphangiectasia is secondary to
obstructed pulmonary venous flow and abnormal formation of pulmonary lymphatic
drainage which infers a very poor prognosis.
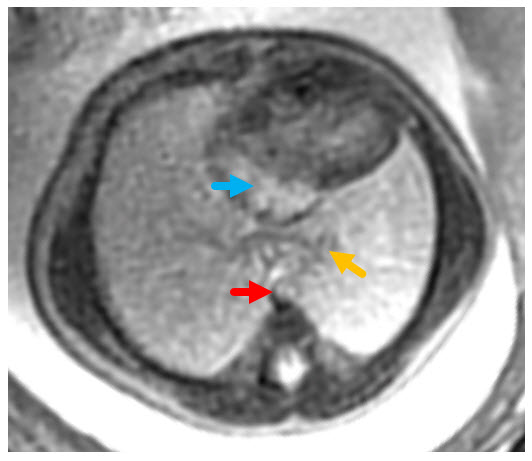
Pseudo ECG-gated BFFE axial 4 chamber
view of the heart shows a single atrium (light blue arrow), pulmonary veins (yellow-orange arrow) which do not connect to the atrium and
wide spacing between the posterior atrial wall and the aorta (red arrow).
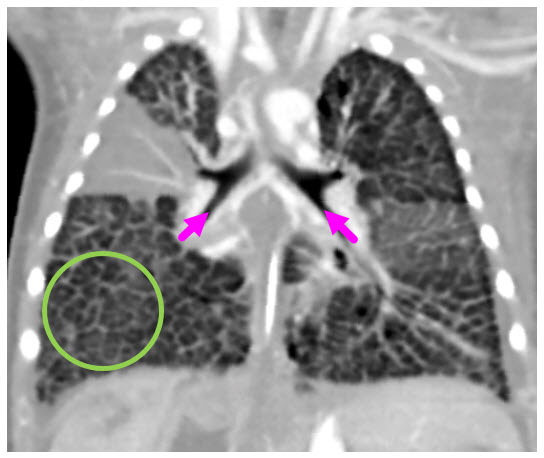
Postnatal
coronal ECG-triggered, contrast enhanced CT image of the chest shows large lung
volume with interstitial thickening due to lymphangiectasia (green circle) and bilateral morphologically R main bronchi (pink arrows).
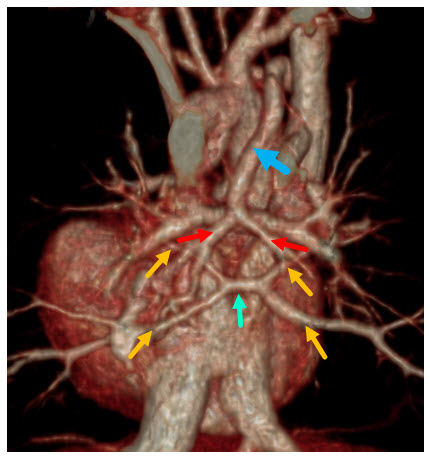
A 3D reconstructed CT image viewed from
posterior shows multiple pulmonary venous drainage pathways: 4 very small
caliber pulmonary vein branches (yellow orange arrows) and their confluence (light green arrow) which does not drain to the left atrium
and 2 pulmonary vein branches (red arrows) that drain
via a vertical vein (blue arrow) to the brachiocephalic vein.