4575
The importance of fetal MRI in the evaluation of external ear deformities1Shandong University, Jinan, China, 2Shandong Medical Imaging Research Institute, Jinan, China, 3MR Collaboration, Siemens Healthcare Ltd., Beijing, China
Synopsis
Fetal external ear
deformities sometimes indicate that a chromosomal abnormality is present. This
study aimed to demonstrate the feasibility of fetal MRI in the evaluation of
auricular deformities, as well as the added value of external auditory canal atresia.
We calculated the diagnostic sensitivity, specificity, and accuracy of fetal
MRI and described the imaging features. Our study showed that fetal MRI can
provide valuable information to assist in the diagnosis of external ear
deformities.
Introduction/Purpose
External ear deformities can indicate aneuploidy. Examining these deformities on the fetal face can help to diagnose chromosomal abnormalities in utero1. Ultrasonography (US) is the first line of investigation in these cases but is sometimes limited because of suboptimal fetal positioning and shadowing artifacts from developing bone structures2. The purpose of this study was to evaluate the clinical utility of fetal magnetic resonance imaging (MRI) in the diagnosis of external ear deformities and to describe the morphologic characteristics of fetal MRI.Methods
Eighteen pregnant women (mean age, 30.5 years, range, 22-40 years; mean gestational age, 27 weeks, range, 23-35 weeks) with fetuses that had suspected external ear deformities on US underwent MR scans on a 1.5-Tesla (1.5T) MR scanner (MAGNETOM Amira, Siemens Shenzhen Magnetic Resonance Ltd., Shenzhen, China) with a 13-channel body coil between November 2017 and September 2019. For the control group, a total of 36 normal fetal ears from 18 age- and gestational age-matched pregnant women (mean age, 30 years, range, 21-39 years; mean gestational age, 26.9 weeks, range, 24 -34 weeks) were also examined. The true fast-imaging with steady-state precession (TrueFISP) sequence was obtained in the axial, coronal, and sagittal planes, with the following parameters: TR = 621.61 ms, TE = 1.76 ms, flip angle = 79°, FOV = 380 × 310mm², slice thickness = 4 mm, slice gap = -2 mm, voxel size = 1.3 × 1.3 × 4.0 mm³, 20 slices, and acquisition time = 13s. Images were independently reviewed by two neuroradiologists (with more than 10 years of experience in fetal MRI) who were blinded to any of the fetal information. The sensitivity, specificity, and accuracy of MRI in being able to diagnose fetal auricular deformities and atresia of the external auditory canal were calculated using postnatal follow-up as the gold standard. In addition, auriculocephalic angles (the angle formed by the planes of auricle and skull) of all auricles were recorded. Differences in auriculocephalic angles between the two groups were analyzed by an independent-sample t test using SPSS software (v. 25, IBM Corp., Armonk/NY, USA). A P value of less than 0.05 was considered to indicate statistical significance.Results
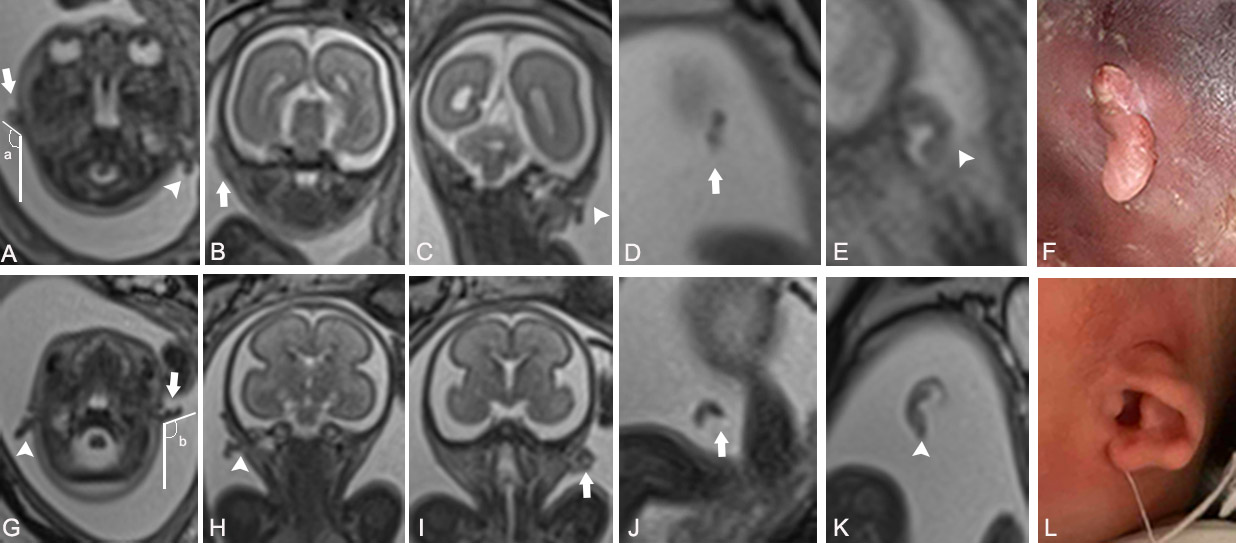
A total of 36 fetal external ears were detected among 18 fetuses with deformities. Twenty-two external ear deformities were confirmed at postnatal follow-up, including 22 cases with an auricular deformity (3 with a cup ear deformity and 19 with microtia) and 18 cases with external auditory canal atresia. Among the 18 fetuses, one had a unilateral cup ear deformity, one had a bilateral cup ear deformity, thirteen had unilateral microtia (four on the left, nine on the right), and three had bilateral microtia (figure 1). Cleft palate was found in one fetus with bilateral microtia and bilateral external auditory canal atresia. The accuracy of MRI in the diagnosis of auricular deformities was 100% (22/22). For the diagnosis of external auditory canal atresia, the sensitivity, specificity, and accuracy of MRI were 94.4% (17/18), 75.0% (3/4), 90.9% (20/22), respectively. In all, 22 cases showed an increased auriculocephalic angle. Significantly increased auriculocephalic angles were observed in the deformity group compared with those in the control group (P<0.05). External auditory atresia was characterized by a low tubular signal instead of a high tubular signal.Discussion
We used fetal MRI to evaluate external ear deformities and describe their morphologic characteristics. Our results show that there is a right-sided dominance in unilateral microtia, which is consistent with the previous study3. Compared with US, MRI can not only provide information about the deformed auricle but also provide additional information about the external auditory canal. In addition, auriculocephalic angles can be used as an important basis and objective index in the diagnosis of external ear deformities. Since the sample size of this study was small, increasing the sample size for a more comprehensive evaluation is needed to confirm our conclusions further.Conclusions
MRI plays an important role in the diagnosis of fetal external ear deformity and can be used as an effective supplement to US, especially for the diagnosis of external auditory atresia. On MRI, deformed auricles have abnormal shapes and auriculocephalic angles. External auditory atresia is characterized by a low signal instead of a high tubular signal.Acknowledgements
This study was supported in part by grants from The National Natural Science Foundation of China (81671668).References
1.Nagarajan M, Sharbidre K G, Bhabad S H, et al. MR imaging of the fetal face: comprehensive review[J]. Radiographics, 2018; 38(3): 962-980.
2.Levine D, Barnes P D, Robertson R R, et al. Fast MR imaging of fetal central nervous system abnormalities[J]. Radiology, 2003; 229(1): 51-61.
3.Klockars T, Rautio J. Embryology and epidemiology of microtia[J]. Facial Plast Surg, 2009; 25(3): 145-148.
Figures