4540
A comparison of RESOLVE DWI with delayed gadolinium-enhanced T1-weighted MRI in detecting cholesteatoma based on 531 patients’ data1Radiology, EENT Hospital of Fudan University, Shanghai, China, 2Siemens Healthcare, Shanghai, China
Synopsis
This study aimed to compare the performance of readout-segmented echo-planar imaging (RESOLVE) DWI and delayed gadolinium-enhanced T1-weighted MRI to diagnose cholesteatoma on 531 patients. The results showed that RESOLVE DWI can be an excellent tool for the detection of primary cholesteatoma.
Abstract
IntroductionIn recent years, diffusion-weighted imaging (DWI) has been proven to be an important diagnostic tool for evaluating head and neck lesions, which provides additional diagnostic information compared to conventional MRI1,2. Further, many studies have shown that DWI has a high sensitivity and specificity for identifying the presence of cholesteatoma due to its high keratin content. However, conventional single-shot echo-planar imaging (SS-EPI) diffusion imaging suffers from distortion artifacts due to the susceptibility change at tissue interfaces. The spatial resolution is also limited, and failed to detect lesions smaller than (5mm)3. Currently, with the implementation of novel DWI techniques to the diagnosis of cholesteatoma, especially the RESOLVE sequence, the detection rate of cholesteatoma and the sensitivity of diagnosis of small lesions has been greatly improved, because this sequence employs a multi-shot EPI trajectory to reduce the image distortion artifacts. The purpose of this study was to retrospectively compare the value of RESOLVE DWI imaging in detecting cholesteatoma in the middle ear with delayed gadolinium-enhanced T1-weighted MR imaging. The combination of RESOLVE and delayed gadolinium-enhanced T1-weighted MR imaging techniques in the diagnosis of cholesteatoma was further evaluated. The role of RESOLVE DWI for differentiating cholesteatoma and non-cholesteatoma lesions by measuring the apparent diffusion coefficient (ADC) in a large series of surgically verified cases was conducted. ADCs of cholesteatoma and non-cholesteatoma were measured. Furthermore, a possible cut-off in ADC values is also discussed.
Methods
From August 2014 to November 2018, 531 patients(311 men and 220 women, mean age, 37.1 years; range, 2–80 years) with clinical suspicion of cholesteatoma in the middle ear were enrolled in this study, 59 of them, who had undergone previous surgery for cholesteatoma, were suspected of recurrent cholesteatoma. All MR exams were performed on a 3 T MRI scanner (MAGNETOM Verio, Siemens Healthcare, Erlangen, Germany) with a 32-channel head coil. The axial T1W1 and coronal and axial TSE T2W images were acquired before contrast injection. The parameters of the used DWI and post-contrast T1W sequences were: 1) axial RESOLVE DWI (TR/TE =4000/65/ms, slice thickness = 2 mm, inter-slice distance = 0.2 mm, slices = 21, bandwidth =766 Hz/Px, FOV = 220 × 220 mm2, matrix = 192 × 192, voxel size = 1.4 × 1.4 × 2.0 mm3, b = 0, 1000 s/mm2, segments=5, acquisition time = 1 min 50s); and 2) axial T1WI after gadoterate dimeglumine injection of 0.1 mmol per kilogram of body weight, and the axial and coronal T1W sequences were repeated with the same parameters as those used before contrast material administration. Axial delayed contrast-enhanced T1W images were obtained 5 minutes after contrast material administration. For data analysis, overall sensitivity, specificity, negative predictive value (NPV), and positive predictive value (PPV) were assessed. ADCs between cholesteatoma and non-cholesteatoma were measured. Furthermore, a possible cut-off in ADC-values is also discussed. Receiver operating characteristic (ROC) curve analysis was utilized to examine the accuracy of ADC values.
Results
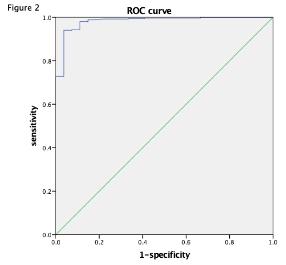
Sensitivity, specificity, NPV, and PPV of RESOLVE are higher than those of delayed gadolinium- enhanced T1-weighted MR image (table 1a). Specificity of the combined images of RESOLVE DWI and delayed gadolinium-enhanced T1-weighted MR image is higher than RESOLVE DWI (table1b,1c). The ADC value of cholesteatoma (852.67×10-6mm2/s) measured in RESOLVE DW images is significantly lower than that of non-cholesteatoma (1529.78×10-6 mm2/s) (figure1). The area under the ROC curve of the mean ADCs is 0.98, and the optimal cutoff point is 1195×10-6mm2/s (figure 2).
Discussion & Conclusions
ADC value can be used as a diagnostic tool for differentiating cholesteatoma from non-cholesteatoma in the middle ear. The sensitivity and specificity of the RESOLVE DW imaging sequence in the diagnosis of cholesteatoma are significantly higher than those of enhanced T1-weighted MR imaging. RESOLVE DWI can be an excellent tool for the detection of primary cholesteatoma, which is better than using delayed enhanced T1-weighted image alone, and can be used as an alternative to second-look surgery for the detection of residual cholesteatoma. Further, enhanced T1-weighted image can be used to improve the diagnostic rate of RESOLVE for cholesteatoma with a large number of inflammatory granulation. In this study, the smallest diameter of cholesteatoma measured by T2WI was 2.3 mm (Figure 3). The results suggest that RESOLVE imaging is sensitive to small lesions (2-5 mm), and trained radiologists can confidently diagnose cholesteatoma with a diameter > 3 mm. Smaller lesions may be missed.
Acknowledgements
The authors of this manuscript declare no relationships with any companies, whose products or services may be related to the subject matter of the article. The authors state that this work has not received any funding. No complex statistical methods were necessary for this paper. Institutional Review Board approval was not required because this was a retrospective study. No study subjects or cohorts have been previously reported.References
1.Panyarak W, Chikui T, Yamashita Y et al. Image Quality and ADC Assessment in Turbo Spin-Echo and Echo-Planar Diffusion-Weighted MR Imaging of Tumors of the Head and Neck. Academic radiology. 2018; undefined(undefined):undefined.
2.Thoney HC, Keyzer FD, et al. Diffusion-weighted MR imaging in the head and neck. Radiology. 2012;263(1):19-32.
3.Vercruysse JP, De Foer B, Pouillon M, Somers T, Casselman J, Offeciers E. The value of diffusion-weighted MR imaging in the diagnosis of primary acquired and residual cholesteatoma: a surgical verified study of 100 patients. European radiology. 2006;16(7):1461-1467.
Figures