4524
Presurgical planning of MRgFUS for Essential Tremor (ET) with protocol for high quality DTI1Henry Jackson Foundation for advancement in Military Medicine Inc, Rockville, MD, United States, 2National Insitutes of Health, Bethesda, MD, United States, 3Azienda Ospedaliera Universitaria Integrata, Verona, Italy
Synopsis
This study evaluates the role of a high quality DTI in presurgical planning of MRgFUS for initial target localization.
Introduction
Essential Tremor (ET) is a progressive, neurological disorder characterized by bilateral shaking, with or without tremor in other locations such as head, voice or lower limbs.[1] Severe ET is very debilitating. Recently, magnetic resonance guided focused ultrasound (MRgFUS) has been shown to be an effective therapeutic approach to reduce ET symptomatology. MRgFUS produces a thermal ablation of the ventral intermediate nucleus [VIM] of the thalamus [1-4] without requiring craniotomy. The challenge in the presurgical planning of this procedure is the accurate and precise identification of VIM. Due to the proximity of VIM to the posterior limb of internal capsule (PLIC), inaccurate targeting may result in important motor or sensory impairment. Moreover, direct identification of the VIM in T1W- and T2W-MRI is problematic because of lack of contrast with adjacent structures. Therefore, the initial target region, for MRgFUS sonication is determined based on a-priori stereotactic coordinates using landmarks identifiable on structural MRIs images, such as the posterior commissure and the third ventricle. A series of sub-threshold sonications are often necessary to reposition the target to obtain the optimal functional response and absence of undesired effects. This iterative repositioning process is time consuming and may be risky. Therefore, achieving a more accurate initial targeting is highly desirable. Diffusion Tensor Imaging (DTI) has been shown to be informative for thalamic parcellation, [5-8] which could be used for more accurate guidance of the initial sonication in individual patients. However, typical diffusion MRI acquisitions suffer from geometric distortions, low SNR, and other artifacts that currently preclude their use for accurate planning. Here, we used a diffusion acquisition protocol [9] and a diffusion processing pipeline [10,11] that yield morphologically accurate, high quality DTI data. Our goal was to assess if the availability of this high quality presurgical DTI scan, that can be co-registered with high accuracy to structural MRIs acquired pre- and post-surgery, could be helpful for more accurate initial identification of the sonication target in ET patients.Materials and methods
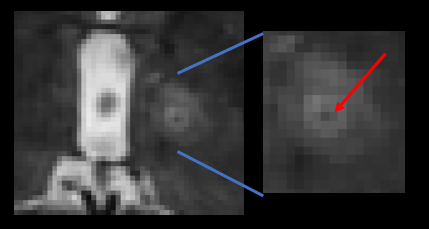
Experimental designWe considered the center of the MRgFUS lesion at the 6 hours post-surgery MRI, in patients that had improved tremor symptomatology and no adverse effects, as the optimal target that should have been achieved in presurgical planning. We then evaluated the position of this target in the presurgical directionally encoded color (DEC) maps computed from high quality presurgical DTI.
Subjects included in the study were referred for the MRgFUS treatment due to disabling ET. They were between 70-80 years of age. Established recommended MRgFUS procedures were followed[1], including no more than 20 (mean 15) sonications and a maximum temperature of 60°C on the final target. The target for final sonication was decided based on the functional feedback received after each sub -threshold sonication.
T2W and DWIs were acquired before surgery and at 6 hours post surgery. DWIs were collected with four different phase-encodings, AP-PA-RL-LR ( with AP-PA 20 + 4 b0; RL-LR 21 + 4b0); slice thickness 2 mm; b-value 1000 s/mm2. Fat suppressed T2WI scans were acquired on the same scanner at a slice thickness of 1.4 mm.
Data processing pipeline
1. manual ac/pc alignment [12] of presurgical T2WI
2. rigid registration of postsurgical T2WI to presurgical T2WI [13]
3. Motion, eddy and epi distortion correction of diffusion data of presurgical DTI using the corresponding rigidly aligned presurgical T2WI.[10,11] The final result of the processing pipeline is the rigid co-registration of presurgical DTI and postsurgical T2WI.
Results
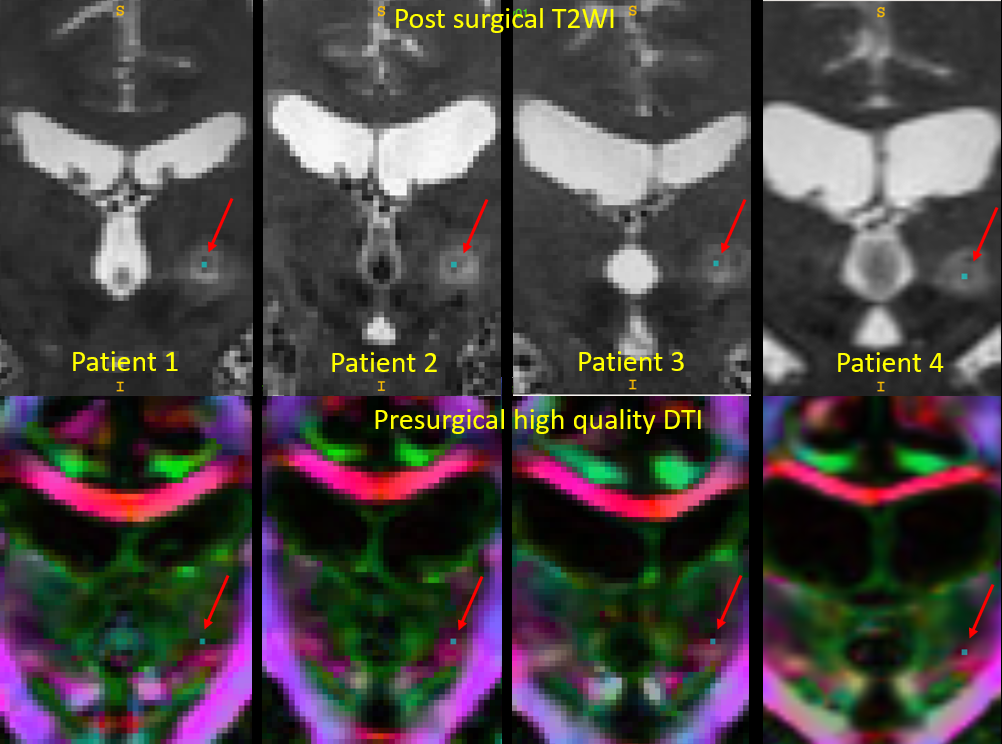
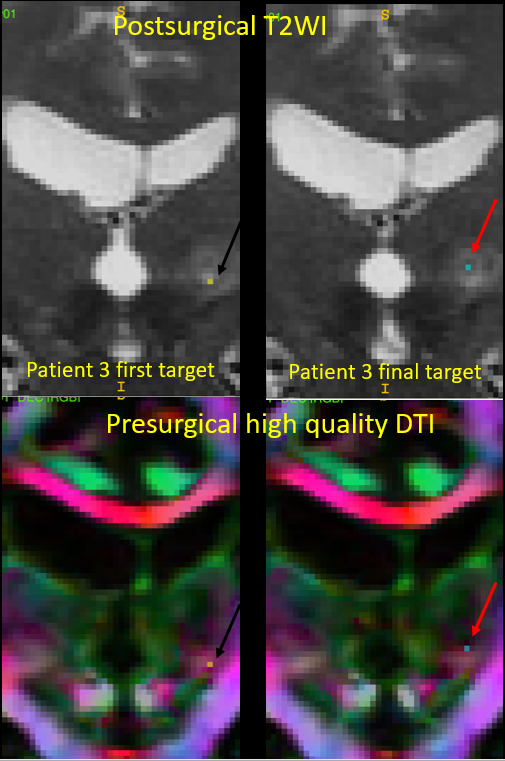
Figure 2 shows the location of the final MRgFUS lesion in four patients. All these patients showed improved ET symptomatology and no adverse effects due to treatment. It can be observed that the final target regions selected for the MRgFUS surgery correspond to a consistent location in the presurgical DTI. The location of these regions corresponds to a pink area in the DEC maps and a few millimeters medial to the PLIC.We examined the location of the initial target of sonication in a patient who experienced slight paresthesia and compared it to the final target location (fig3). On the presurgical DTI, we could document that the initial target location was very close to the PLIC, while the final target that was identified guided by the functional feedback from the patient, is consistent with the final target region identified in other patients.
Discussion
The localization of VIM in MRgFUS surgery currently relies on a-priori defined stereotactic location of the structure, combined with the functional feedback received during iterative sonications.The role of high quality DTI is clearly highlighted in this preliminary evaluation, to more accurately identify the initial target for sonication in presurgical planningAcknowledgements
References
1) Elias W..J., et al A pilot study of focused ultrasound thalamotomy for essential tremor N Engl J Med, 2013,369:640-648
2) Deuschl, G & Bergman H: Pathophysilogy of nonparkinsonian tremors. Movement disorders, 2002, Vol 17 suppl 3, pp. S41-8
3) Dobrakowski P.P., et al. MR-guided focused ultrasouns: a new generation treatment of parkinsons disease, essential tremor and neuropathic pain. Interventional neuroradiaology, 2014, 20:275-282
4) Jolesz F.A and McDannold, N.J. Magnetic resonance guided focused ultrasound. A new technology for clinical neurosciences. Neurologic clinics, 2014, 32(1): 253–269
5) Wiegell M.R., et al, Automatic segmentation of thalamic nuclei from diffusion tensor magnetic resonance imaging, Neuroimage, 2003, vol 19, Pages 391-401
6) Coenen VA.,et al, A role of diffusion tensor imaging fiber tracking in deep brain stimulation surgery: DBS of the dentato-rubro-thalamic tract (drt) for the treatment of therapy-refractory tremor, Acta Neurochirurgica, 2011,Vol 152:8, pp 1579-1585
7) Hyam., et al, Contrasting Connectivity of the Ventralis Intermedius and Ventralis Oralis Posterior Nuclei of the Motor Thalamus Demonstrated by Probabilistic Tractography, Neurosurgery, Volume 70:1,2012, Pages 162–169
8) Pouratian.N,et al, Multi dimensional evaluation of deep brain stimulation targeting using probabilistic connectivity based thalamic segmentation, Journal of Neurosurgery, 2005, 115(5):995-1004
9) Irfanoglu.,et al, Evaluating corrections for EDDY-currents and other EPI disortions in diffusion MRI:methodology and a dataset for benchmarking, Magnetic Resonance in Medicine, 2018
10) Irfanoglu.,et al, TORTOISEv3: Improvements and new features of the NIH diffusion MRI processing pipeline, ISMRM 25th annual meeting, Honolulu, HI, abstract #3540
11) Irfanoglu.,et al, DR-BUDDI (Diffeomorphic Registration for Blip-Up Blip-Down Diffusion Imaging) method for correcting echo planar imaging distortions, Neuroimage, 2015
12) Matthew J McAuliffe.,et al, Medical Image Processing, Analysis & Visualization in Clinical Research. 2001, CBMS’01 Proceedings of the Fourteenth IEEE Symposium on Computer -Based Medical Systems Page 381
13) Brian Avants.,et al, A Reproducible Evaluation of ANTs Similarity Metric Performance in Brain Image Registration, Neuroimage, 2011
Figures