4518
Evaluation of simultaneous multislice acquisition with advanced processing vs. conventional sequence in free-breathing DWI for liver patients1Royal Marsden Hospital and Institute of Cancer Research, London, United Kingdom, 2Siemens Healthcare, Erlangen, Germany
Synopsis
Diffusion Weighted Imaging (DWI) in combination with simultaneous multislice (SMS) acquisition has the potential to decrease acquisition time and improve image quality in abdominal MRI. In this study, we evaluated the image quality of free-breathing DWI acquired from 25 patients with liver metastases and compared SMS (with/without an advanced processing option) DWI with conventional bipolar echo planar DWI. We found that free-breathing liver DWI based on a SMS-accelerated protocol with advanced processing methods was faster and demonstrated better image quality when compared with a conventional bipolar DWI protocol.
Introduction
Diffusion Weighted Imaging (DWI) is a valuable functional MRI technique that can characterise tumour cellularity and assess tumour response to therapy1. To overcome its relatively long acquisition time, DWI can be combined with a method called simultaneous multislice (SMS) acquisition2,3 that allows data acquisition acceleration. This study assessed DWI quality obtained from 25 patients with liver metastases and compared SMS (with/without advanced processing) and conventional diffusion sequences.Patients and methods
PatientsTwo cohorts of patients referred for liver MRI were scanned on a 1.5T scanner (MAGNETOM Aera, Siemens Healthcare, Erlangen, Germany). Initially, free-breathing axial DWI of the liver was performed with four different acquisition and reconstruction schemes in a cohort of 5 patients (3 females, 2 males, mean age 61.2 years). Three DWI schemes were assessed on a further cohort of 25 patients (18 males, 7 females, mean age 63.2, range 36-84 years) that were referred for diagnosis or therapy response assessment between January and June 2019.
MRI protocols
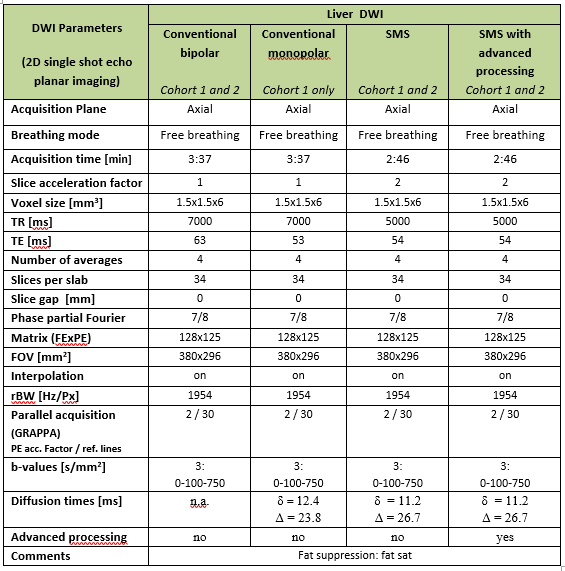
The four initial DWI series, with matched resolution and b-values, were: 1) bipolar conventional DWI, 2) monopolar conventional DWI, 3) monopolar SMS-DWI and 4) monopolar SMS-DWI with advanced processing. MR protocols are detailed in Table 1. All DWIs were acquired in free breathing using a 3-direction trace-weighted diffusion encoding with 3 b-values (0, 100, 750 s/mm2), 4 averages per b-value, and a resolution of 1.5x1.5x6 mm3. After an initial assessment of image quality of the 5-patient cohort data, the monopolar conventional DWI was dropped and only the remaining 3 types of DWI were further acquired on the main cohort of 25 patients.
Monopolar means Stejskal-Tanner type single refocused diffusion sensitising, whilst bipolar uses a double refocused diffusion preparation scheme4 which is less prone to eddy-current-induced distortions. SMS-DWI used a prototype sequence that provided image series with and without additional advanced processing options. The latter employed a non-rigid motion correction algorithm, intensity correction due to locally corrupted images and adaptive averaging of complex-valued images before magnitude extraction.
Image quality assessment
The overall image quality of the higher b-value images and ADC maps for all DWI schemes in the 25-patient cohort were assessed independently by two radiologists with >5 and >20 years of experience in abdominal MRI. The reviewers were blinded to the sequences and scored images on a 3-point Likert scale (1=poor, 2=fair, 3=best quality). The overall scoring of image quality was based on evaluating the liver contour, tumour/vasculature delimitation, intra/inter-slice signal homogeneity, image distortions, and image sharpness.
Statistics
Ratings from each observer were summarized as means per each method and type of image. Friedman non-parametric tests (MATLAB, R2019a, MathWorks, Natick, MA) compared the image scoring for the 3 DWI approaches. Where Friedman results were significant, further post-hoc analysis based on pairwise Wilcoxon tests (signed rank) with Bonferroni correction was performed. The inter-observer degree of agreement regarding the visual evaluation results was measured using kappa statistics (quadratic weighting) with kappa values of 0.01–0.20 representing slight agreement, 0.21–0.40 fair, 0.41–0.60 moderate, 0.61–0.80 substantial, and 0.81–1.00 excellent5.
Results and discussion
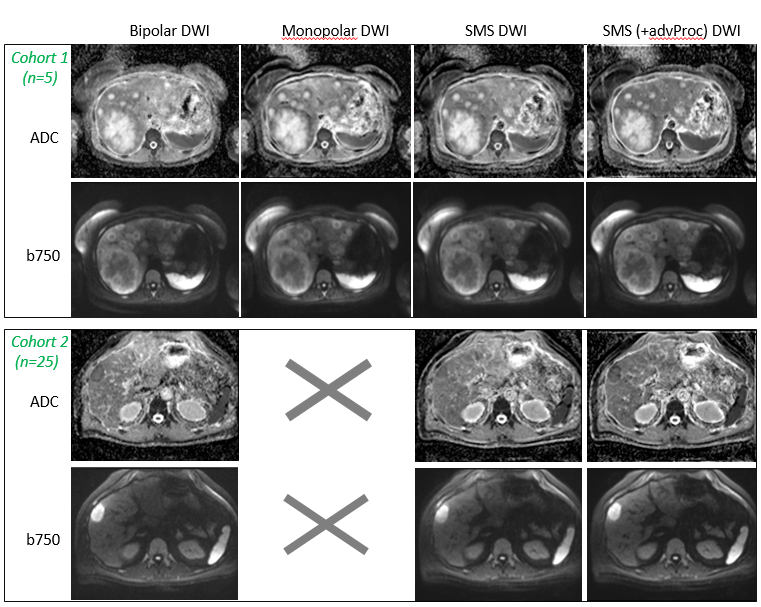
Examples of b=750 s/mm2 images and ADC maps from two patients with liver metastases from colorectal (rows 1&2) and bowel carcinoma (rows 3&4) are presented in Figure 1. Columns 1&2 display images derived from conventional DWI, whilst the SMS-derived images are shown in columns 3&4. The conventional DWI was acquired with a TR=7s (the minimal required for the bipolar sequence) and an acquisition time of 3:37 min. The accelerated DWI used a reduced TR=5s and a slice acceleration factor of 2 allowing faster acquisitions (2:46 min).The SMS-DWI with advanced processing demonstrates more homogeneous signal across the slice, in particular for the left lobe of the liver (column 4 vs 1). The advanced processing operations reduce motion artefacts and generate crisper images with a sharper delimitation of the liver or blood vessels (column 4 vs columns 3,2,1; second row).
The summary of the radiological scoring of all images derived from the 25 patients is shown in Table 2. The SMS protocol with advanced processing was ranked as best in terms of image quality by both observers for b100, b750 and ADC evaluations. For the other sequences, the two readers did not agree over the worst images for b100 and ADC; they ranked, however, the SMS sequence without advanced processing as worse than conventional bipolar DWI for the b750 image evaluation. Note that the SMS method is based on a monopolar acquisition which could explain the poorer ranking of its b750 image as the lack of advanced image processing leads to stronger eddy-current induced distortions between different diffusion directions.
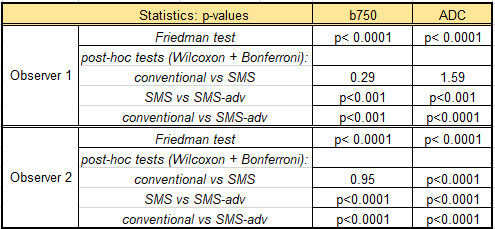
The Cohen kappa test statistics found moderate agreement between the readers only when assessing ADC maps (k=0.56, p<0.0001) and b750 (0.60, p<0.0001) images. Moreover, the Friedman tests were statistically significant across all DWI approaches and results of the further post-hoc analysis are presented in Table 3, confirming again the superiority of the SMS with advanced processing method against the other two sequences.
Conclusion
Free-breathing liver DWI based on a SMS protocol with advanced processing method was faster and demonstrated better image quality when compared with a conventional bipolar DWI.Acknowledgements
We acknowledge the support of NHS funding to the NIHR Biomedical Research Centre and NIHR Royal Marsden Clinical Research Facility. This report is independent research funded partially by the National Institute for Health Research. The views expressed in this publication are those of the author(s) and not necessarily those of the NHS, the National Institute for Health Research or the Department of Health.References
1. Koh DM and Collins DJ, Diffusion-weighted MRI in the body: applications and challenges in oncology. Am J Roentgenol 2007; 188(6):1622-35.
2. Obele CC, Glielmi C, Ream J, et al. Simultaneous multislice accelerated free-breathing diffusion-weighted imaging of the liver at 3T. Abdom Imaging 2015; 40(7):2323-2330.
3. Taron J, Weiss J, Martirosian P, et al. Simultaneous multislice Diffusion-Weighted MRI of the liver: analysis of different breathing schemes in comparison to standard sequences. Journal of Magnetic Resonance Imaging 2016; 44(4):865-879.
4. Reese TG, Heid O, Weisskoff RM, et al. Reduction of Eddy-Current-Induced Distortion in Diffusion MRI Using a Twice-Refocused Spin Echo. Magnetic Resonance in Medicine 2003; 49(1):177-182.
5. Landis JR and Koch GG. The measurement of observer agreement for categorical data. Biometrics 1977; 33(1):159-174.
Figures