4511
Utility of DWI with quantitative ADC in diagnosing residual or recurrent HCCs after TACE: A systematic review and meta-analysis1Department of Radiology, Third Affiliated Hospital of Soochow University, changzhou, China
Synopsis
This meta-analysis was to investigate the accuracy of DWI and ADC value in diagnosing residual or recurrent HCCs after TACE. This study suggested DW have high diagnostic efficacy, and ADC value can be used to differentiate residual or recurrent HCCs after TACE.
Background and Purpose
Transarterial chemoembolization (TACE) is a first-line therapy for hepatocellular carcinoma (HCC) patients who are diagnosed at an intermediate-advanced stage by concentrating chemotherapeutic agents at the tumor site while blocking the tumor’s primary feeding artery. However, the tumor recurrence rate after TACE is relatively high, with reported 6- and 12- month recurrence rates of 22.3% and 78%, respectively1. By detecting the water molecules diffusion process indirectly, diffusion weighted imaging (DWI) provides information regarding tissue cellularity and cell membrane integrity, and its quantitative value of apparent diffusion coeffcient (ADC) is highly associated with tumour cellularity2, indicating DWI and ADC value may be potentially used to diagnose residual or recurrent HCCs after TACE. Therefore, based on the currently available published articles of DWI and ADC value in detecting residual or recurrent HCCs after TACE, this meta-analysis was performed to provide evidence-based conclusion for imaging diagnostics.Materials and Methods
An electronic literature search of Pubmed, Embase, Web of Science, Ovid and the Cochrane library database was performed to select original studies up to July 2019 that evaluate the accuracy of DWI and quantitative ADC value in diagnosing residual or recurrent HCCs after TACE. Two researchers independently extracted data and assessed the methodological quality of the included studies by applying Quality Assessment of Diagnostic Accuracy Studies-2 (QUADAS-2) tool. Data syntheses and statistical analysis were performed using STATA software. Pooled sensitivity (SEN), specificity (SPE), positive likelihood ratio (PLR), negative likelihood ratio (NLR), and area under ROC curve (AUC) with its 95% confidence interval (CI) were calculated to assess the performance of DWI in diagnosing residual or recurrent HCCs after TACE. Additionally, possible factors including design type (retrospective or prospective), b value (<800 or ≥800) and threshold method (visual analysis or ADC measurement) that may lead to heterogeneity was analyzed through subgroup analysis. Morever, ADC value between residual or recurrent HCCs group and necrotic lesion group were compared and pooled as mean difference (MD) with random-effect model. A P-value < 0.05 was representative of statistical difference.Results
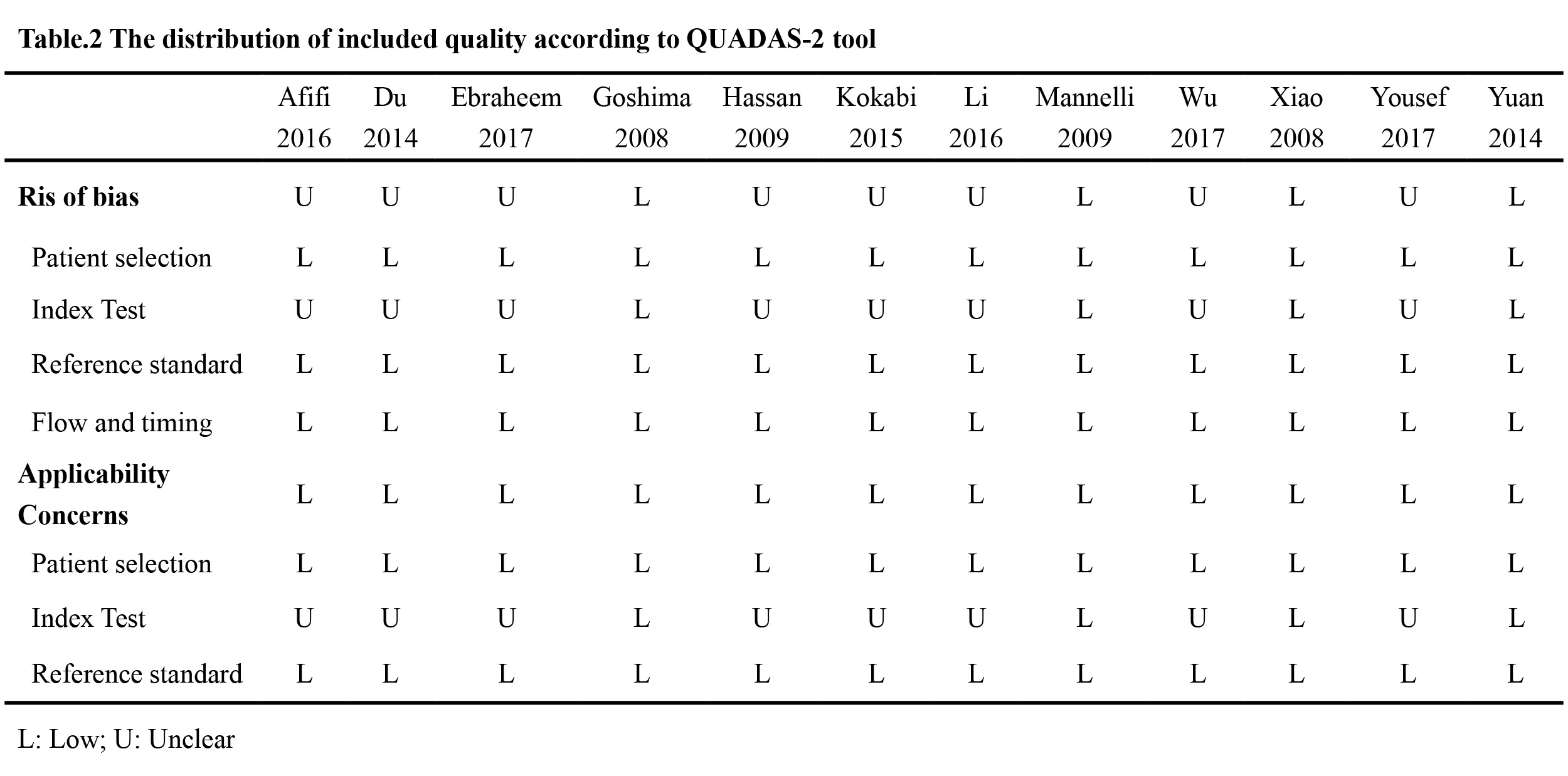
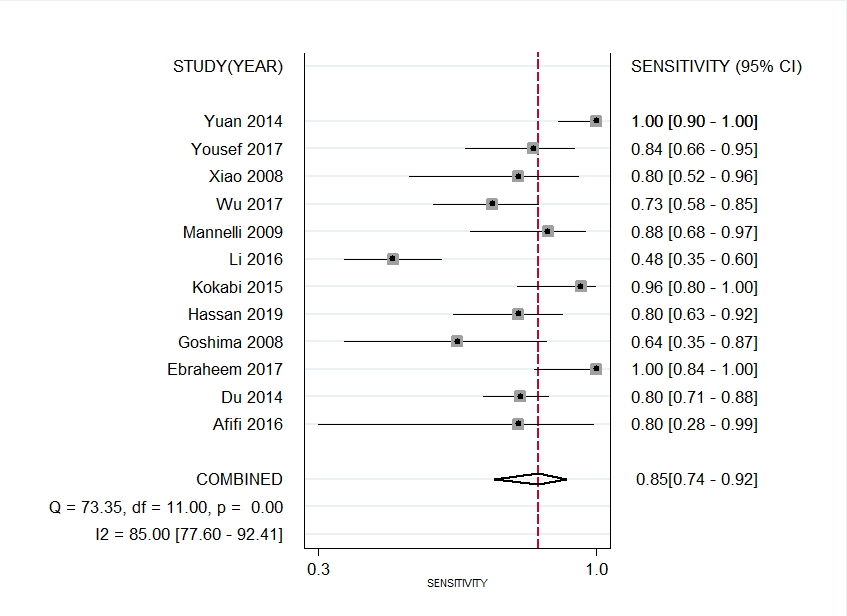
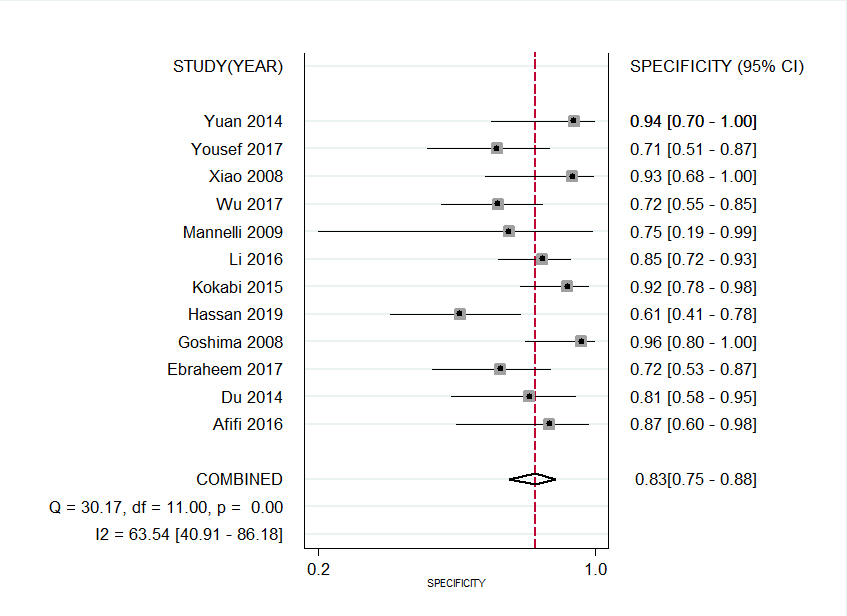
Fig. 1 demonstrates flowchart of study selection process. Ultimately, a total of 12 studies comprising 624 patients and 712 tumors evaluated by DWI were finally included. The methodological assessment of included study using the QUADAS-2 guideline were shown in Figure.2. The pooled weighted values of DWI in diagnosing residual or recurrent HCCs after TACE were as follows: SEN =85% (95%CI: 74%-92%), SPE =83% (95%CI: 75%-88%), PLR =5.12 (95%CI: 3.27-7.38), NLR =0.18 (95%CI: 0.09-0.34), and AUC =0.90 (95%CI: 0.87-0.92), respectively. Forest plots were shown in Fig. 3-4. Additionally, this study demonstrated residual or recurrent HCCs have significantly lower ADC values than necrotic tumors (MD=-0.48, 95%CI: -0.69~-0.27, P<0.01), which shown in Fig.5, indicating ADC value may be of importance to differentiate residual or recurrent HCCs after TACE. For the subgroup analysis, study design type, b value and threshold method used will not pose significant difference to DWI in diagnosing residual or recurrent HCCs after TACE.Discussion
In this study, 12 studies with comprising 624 patients and 712 tumors detected on DWI were included. The SEN, SPE, and AUC value of DWI diagnosing residual or recurrent HCCs after TACE was 85% (95%CI: 74%-92%), 83% (95%CI: 75%-88%) and 0.90 (95%CI: 0.87-0.92), respectively, indicating high value of DWI. The PLR of DWI was 5.12 (95%CI: 3.27-7.38), revealing moderate accuracy. The NLR value of DWI was 0.18 (95%CI: 0.09-0.34), a negative DWI result may be used as a moderate justification to rule out residual or recurrent HCCs after TACE. Morever, this pooled analysis indicated that ADC value of necrotic tumors were significantly higher than residual or recurrent HCCs, revealing ADC value can be used as an efficient imaging to differentiate properties of lesion after TACE.In this meta-analysis, the opposite result of false-negative (1-SEN) and false-positive (1-SPE) rate were 15% and 17%, respectively, for DWI diagnosing residual or recurrent HCCs after TACE, and the following possible factors could contribute to this result. 1) Adjacent hepatic inflammation could be able to restrict water diffusion, resulting in sustained hyperintensity on DWI and therefore produce false-positive DWI diagnosis in the lesion followed by TACE 3. 2) Intralesional hemorrhage or liquefactive necrosis after TACE, which may also contribute to diffusion restriction in necrotic tumors and can decrease the accuracy of DWI in detecting residual or recurrent HCCs 4. 3) Owing to the limited spatial resolution of DWI, small tumors would not be able to be diagnosed precisely, thus leading false negative and false positive results demonstrated on DWI. 4) The signal intensities observed on DWI are easily affected by T2-relaxation time of the tissue, because the false positive diagnosis of necrotic tissue may be induced by well-differentiated HCCs, high-grade dysplastic nodules, and hemangioma 5. Only histopathology can be regarded as the absolute gold standard for diagnosing residual or recurrent HCCs. DSA or follow-up results may contribute to false positive results.Acknowledgements
This work was supported by the National Natural Science Foundation of ChinaReferences
1. Cheng HY, Wang X, Chen D, et al. The value and limitation of transcatheter arterial chemoembolization in preventing recurrence of resected hepatocellular carcinoma. World J Gastroenterol, 2005, 11(23):3644-6.
2. Chapiro J, Wood LD, Lin M, al. Radiologic-pathologic analysis of contrast-enhanced and diffusion-weighted MR imaging in patients with HCC after TACE: diagnostic accuracy of 3D quantitative image analysis. Radiology, 2014, 273(3):746-58.
3. Hwang SH, Yu JS, Chung J, et al. Transient hepatic attenuation difference (THAD) following transcatheter arterial chemoembolization for hepatic malignancy: changes on serial CT examinations. Eur Radiol, 2008, 18(8):1596-603.
4. Tung GA, Evangelista P, Rogg JM, et al. Diffusion-weighted MR imaging of rim-enhancing brain masses: is markedly decreased water diffusion specific for brain abscess? Am J Roentgenol, 2001, 177(3):709-12.
5. Duran R, Ronot M, Kerbaol A, et al. Hepatic hemangiomas: factors associated with T2 shine-through effect on diffusion-weighted MR sequences. Eur J Radiol, 2014, 83(3):468-78.
Figures