4399
Using Diffusional Kurtosis Imaging to Quantify non-Gaussian Water Diffusion in Normal Human Liver1Medical Imaging, Shandong First Medical University, Jinan, Shandong, China, China, 2Medical Imaging, Shandong Provincial Qianfoshan Hospital,the First Hospital Affiliated with Shandong First Medical University, Jinan City, Shandong Province, China, China, 3GE Healthcare, MR Research China,Bejing, Bejing,China, China
Synopsis
This study aimed to test the reproducibility of DKI technique in normal liver and to explore the microscopic and diffusion differences between the left and right hepatic lobes.
32 healthy volunteers were scanned in DKI twice and the interval time was two weeks. All DKI-derived parametrical maps were reconstructed and mean values in eight liver segments were calculated.
We demonstrated that DKI in the liver showed excellent reproducibility between two measurements and found interesting regional distributions of the parameters in liver. Additionally, significant difference was found in DKI-derived parameters between the left and right hepatic lobes
Introduction
While diffusion kurtosis imaging(DKI) has been extensively employed in the central nervous system , fewer DKI studies have been applied in the liver but with controversial views[1-2]. For Mk, Yoshimaru studied the correlation between Mk and Child-Pugh scores in 79 patients with different degrees of liver decompensation, and obtained a moderate correlation between the two parameters. In contrast, Rosenkrantz analyzed the correlation between Mk and Child-Pugh score and not any significant correlation was found. Our research therefore aimed to test the stability of DKI technique in normal liver by using test-retest measurement.Additionally, different lesions in liver, such as cholangiocarcinoma, show a specific location. It remains unclear whether distinct episodes of the disease caused by intrahepatic microstructure or perfusion are varied. Another purpose of this study, on this basis, was thus to explore the microscopic and diffusion differences between the left and right liver lobes.
Material and Methods
32 healthy volunteers (25±3.5 years old) were imaged twice with a GE750 3.0T MR scanner. The time interval of two measurements was two weeks. The applied scan parameters for DKI scanning were of TR 3333ms, TE 69.4ms, slice thickness 6mm, slice spacing 2.0mm, FOV 360mm×288mm, matrix size 128×128, and with five b values (400,800,1200,1600,2000s/mm2) and 15 directions per b value.All acquired DKI data were analyzed using vendor provided DKI postprocessing software on ADW 4.6 workstation (GE Medical Systems). The DKI derived parameters (Md, Mk, FAK, Da, Dr, Ka and Kr) maps were obtained.The mean levels of each metric among eight segments (S1-S8) of liver were calculated.
In SPSS software, the agreement of two scans was measured using the intra-class correlation coefficient (ICC). The Bland-Altman analysis was used to show the intra-reproducibility of eight segments. Multivariate analysis of variance was applied to explore the regional distributions of DKI derived parameters.
Results
Among twice measurement, except for FAk(ICC:0.102), other DKI metrics showed good reproducibilities (0.43<ICC<0.83). In detail, the right lobe had the better reproducibility than the left lobe. The S6 had the highest reproducibility, and the reproducibility of S4 is the worst (Table 1).Mean values of DKI derived parameters in S1-S8 segments were showed in Table 2. The distribution curves of the kurtosis parameters(Mk, Ka and Kr) showed an overall upward trend from S1 to S8 segments (Figure.1.A,C,E). In comparison, the diffusion parameters(Md, Da, Dr) had an opposite pattern (Figure.1.B,D,F). No statistical difference was found between the hepatic caudate lobe (S1) and the left lobe (S2-4) (P>0.05). Statistic differences were found between the left and right hepatic parameters (Table 3).
Discussion
In this study, our results showed that, except for FAk, other DKI metrics showed excellent reproducibility in two scans. The reproducibility of the right lobe was significantly greater than that of the left side. The reason may be explained that the left lobe is adjacent to the phrenic apex and more likely to be affected by the heart beat. The worst reproducibility was found in Segment S4, largely because that partial S4 region close to the heart was affected by cardiac motion artifacts. As for the poor reproducibility for FAk between two measurement, it could be explained by the concept of "pseudo-fractional anisotropy artifact of liver"[3] . Due to the elasticity of the liver, the probability of producing artifacts at the end of breath is 48%, and this artifact has the most significant impact on FAK, which represents the anisotropy parameter. Moreover, not like central system the fiber structures in the liver does not show a positive fractional anisotropy. The superiority of FAk can't thus be shown well.The obtained DKI parameters (Md,Da,Dr,Mk,Ka and Kr) are significantly different between the left and right hepatic lobes, which has not been reported before. The reason, in addition to the cardiac pulsatile artifacts mentioned earlier, may be due to the perfusion or structural differences. An earlier study[4] has reported that the arteriovenous distribution of the left and right hepatic lobes in pets exists difference. Compared to the left lobe, the right lobe receives more blood flow from the portal vein which carries rich nutrients. Together with the relatively sparse free water molecules, higher Mk value may be presented. Other factors including bile duct, gastrointestinal peristalsis and respiratory factors may also lead to the diffusion difference between both lobes[5].
Conclusion
In conclusion, DKI have shown excellent reproducibility in liver imaging. The obtained regional distribution characteristics of the DKI-derived parameters in eight segments may also provide a reference for further studies. In addition, DKI technique in the molecular level is essentially a non-invasive method to demonstrate the perfusion or structural differences between the left and right hepatic lobes.Acknowledgements
No acknowledgement found.References
[1] Yoshimaru D, Miyati T, Suzuki Y, et al. Diffusion kurtosis imaging with the breath-hold technique for staging hepatic fibrosis: A preliminary study. Magnetic Resonance Imaging. 2017; 47:33.
[2] Rosenkrantz AB, Sigmund EE, Winnick A, et al. Assessment of hepatocellular carcinoma using apparent diffusion coefficient and diffusion kurtosis indices: preliminary experience in fresh liver explants. Magnetic Resonance Imaging. 2012; 30(10):1534-40.
[3] Nasu K, Kuroki Y, Fujii H, Minami MJM. Hepatic pseudo-anisotropy: a specific artifact in hepatic diffusion-weighted images obtained with respiratory triggering. 2007; 20(4):205-11.
[4] Taniguchi H, Oguro A, Koyama H, Masuyama M, Takahashi T. Analysis of Models for Quantification of Arterial and Portal Blood Flow in the Human Liver Using Pet. Journal of Computer Assisted Tomography. 1996; 20(1):135.
[5] Yanqi H, Xin C, Zhongping Z, et al. MRI quantification of non-Gaussian water diffusion in normal human kidney: a diffusional kurtosis imaging study. 2015; 28(2):154-61.
Figures
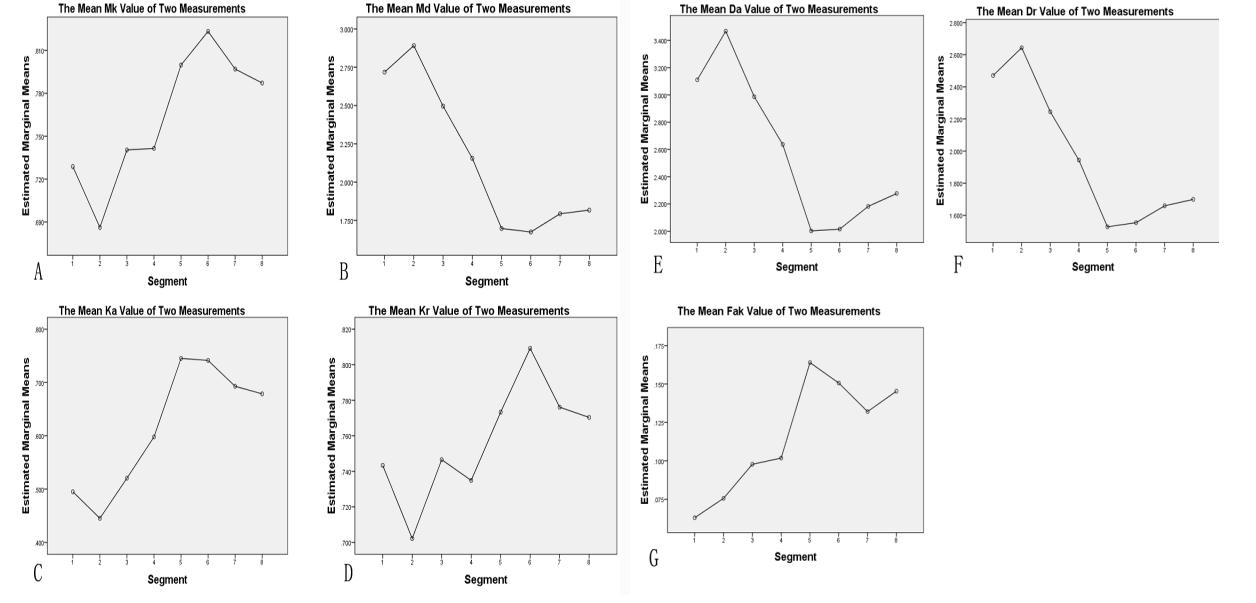
Figure.1 The regional characteristic curve of eight segments
Note:The horizontal axis represents eight liver segments.The longitudinal axis represents the mean value of each parameter in two scans. A-G representing the regional distribution characteristics of DKI derived parameters of Mk, Md, Ka, Kr, Da, Dr and FAk respectively.