4265
Electromagnetic simulation analysis of an RF burn injury due to an ECG lead1Graduate School of Health Sciences, Hokkaido University, Sapporo, Japan, 2Faculty of Health Sciences, Hokkaido University, Sapporo, Japan
Synopsis
It is commonly believed that forming of a conductive loop in an MRI scanner is dangerous because a loop induces a large electric current by the RF excitation and causes RF burn injuries. To verify this belief, we modeled an RF burn injury case, which was caused by an ECG lead, on an electromagnetic analysis software, and simulated SAR and electric field. A large SAR that causes RF burns was confirmed with and without looping that induced small electric field not to cause RF burns. It was suggested that loop formation is not a major cause of RF heating.
Purpose
RF burn injuries are the most frequent incident during MRI examinations.1 It is commonly believed that that forming of a loop is dangerous, because a loop induces a large electric current by the RF excitation and causes RF burn injuries. Therefore, the loop formation is avoided in MRI examinations. However, it was reported that an RF burn injury case induced by an unlooped Electrocardiogram (ECG) lead.2 To clarify the validity of the common belief of the caution to the loop formation, we modeled this reported case with and without a loop formation on the computable human phantom and simulated the specific absorption rate (SAR), the electric strength and temperature rise with the maximum permissible whole-body SAR.Materials and Methods
Using the finite-difference time-domain software Sim4Life (ZMT, Zurich, Switzerland), we modeled the reported case of RF burn injury due to an ECG lead during a thoracic spine examination. 2 The generic MRI birdcage model operating at 128 MHz was employed as a transmission RF coil. The simulation was performed on the model that an ECG lead (diameter 4 mm) was designed on the abdomen of the computable human phantom Duke (Fig.1a). The ECG lead was made of carbon graphite fibers. The models with a looped ECG lead (Fig.1b) and no lead (Fig.1c) were also simulated. The diameter of the ECG lead loop (Fig.1b) was designed as 60 mm. The SAR and the electric field strength (E) distribution under the maximum permissible whole-body SAR were mapped. The mesh size of these simulations was 2 × 2 × 2 mm3. In addition, the temperature rises during the 15-minutes RF exposure was also simulated for each model under the maximum permissible whole-body SAR. Moreover, for the model with the ECG lead loop (Fig.1b), the theoretical electric strength (Eth) in the loop which was induced by alternating B1 field was calculated. The following electromagnetic equation gives Eth by using the simulated B1 in a loop circle S,Eth =ω/2πR ∫S B1 ds (1)
where ω and B1 are an angular frequency and an amplitude of B1 respectively, and R is the radius of the loop circle. Eth and the simulated E value were compared.
Results and Discussion
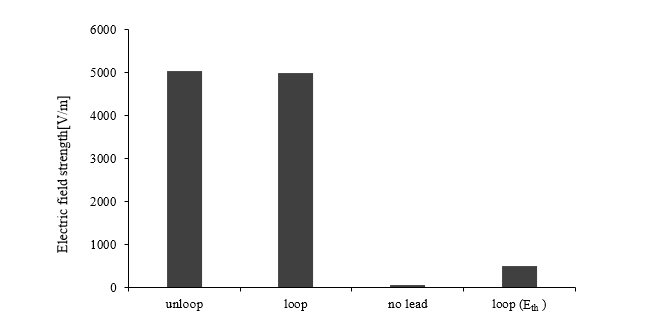
The maximum SARs (SARmax) on the abdomen with and without a looped lead were almost equivalent as 11677 W/kg and 11908 W/kg (Fig. 2d, e) and the values of maximum E (Emax) were 4978 and 5027 V/m (Fig. 2g, h), respectively. The temperature rises in 15 minutes were up to 80.6°C (looped model) and 107.9°C (unlooped model); both temperatures would cause RF burn injuries. These results indicate that the loop formation is not the main cause of RF burn injuries. On the other hand, the SARmax for no lead model was 2.9 W/kg (Fig. 2f); Emax was 70 V/m (Fig. 2i) which are far from the values of lead models. The temperature rose to 37.4°C showing that the RF burn injuries would not occur for no lead model. The Emax increased from no lead model to lead models (looped and unlooped models) dramatically (Fig.3) indicating a huge modulation of E distribution in an MRI scanner due to the existence of conductive lead. The SAR is expressed by the electric conductivity (σ) and E as follows:SAR∝σ・E² (2).
Since SAR is proportional to the square of E, it is reasonable that the SARmax increased strongly with an increase in Emax due to the existence of the ECG lead resulting in the large temperature rises. Whereas Eth induced in the loop was calculated from Eq. (1) as 514 V/m which was 1/10 of Emax on the loop, its contribution to SARmax is quite small as 1/100. Our results showed comparable SARmax, Emax and temperature rise for looped and unlooped lead models, indicating that the loop formation does not contribute to RF burn injuries. Although the electric field is induced in the loop following the basic physics, its contribution to SAR is small. The Emax and temperature rise increased dramatically from no lead model to models with a lead suggesting that the electric field in the MRI scanner is modulated by the existence of conductive martials and it mainly determines RF heating.
Conclusions
The high heating of the RF burn injury due to an unlooped ECG lead was simulated successfully suggesting the main contribution to RF burn injuries is not the loop formation, but the electric field strength in an MRI scanner.Acknowledgements
No acknowledgement found.References
1. Grainger D. MHRA MRI safety guidance: review of key changes and emerging issues. Imaging and Oncology. 2015;42-47.
2. Othman D. MRI-Induced Burns from ECG Leads: Thermal or Electrical Burns? 2017; 1(1):1004
Figures
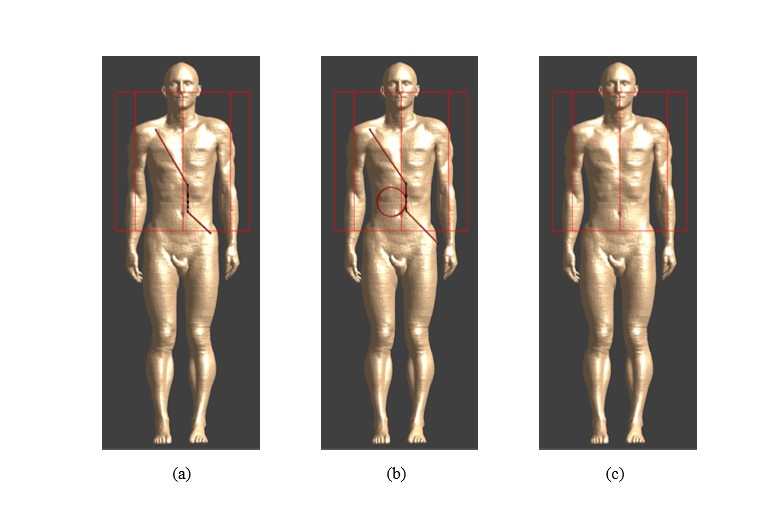
Fig. 1 Simulated models in the electromagnetic analysis software
The ECG lead (brown) was placed on the human model: unlooped (a) and looped (b) no lead (c).
Red lines represent a RF transmit coil (birdcage type).
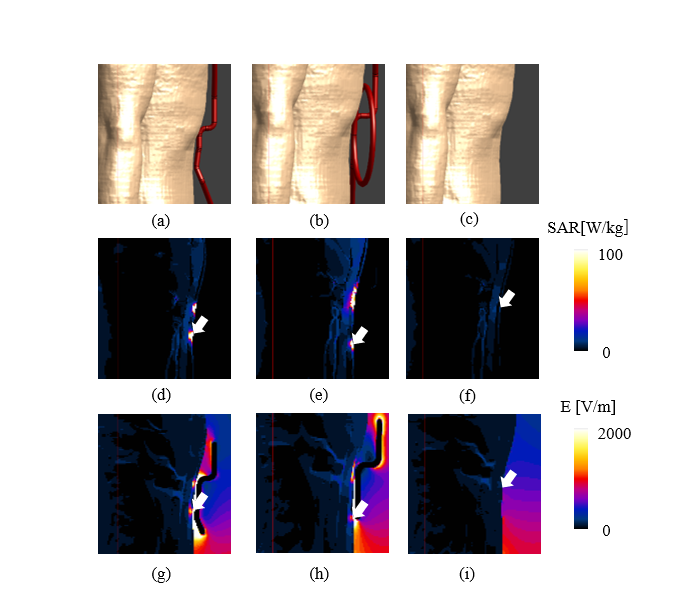
Fig. 2 Simulation models and results in the electromagnetic analysis software
The ECG lead (brown) was placed on the human model: unlooped (a), (d), (g) and looped (b), (e), (h) no lead (c), (f), (i). Upper panels show the abdomen part of the human model, middle panels show SAR maps (arrows indicate points of maximal SAR) and bottom panels shoe the electric field strength distribution.