4211
Damping of acoustic noise for fetal/neonatal MRI and MR-guided radiotherapy
Erik Rutger Huijing1, Koenraad Rhebergen2, Patrick Stroosnijder3, Dennis Klomp1, Jannie Wijnen1, Mariëlle Philippens4, Kim Annink5, and Stefano Mandija4,6
1Department of Radiology, University Medical Center Utrecht, Utrecht, Netherlands, 2Department of Otorhinolaryngology and Head & Neck Surgery, University Medical Center Utrecht, Utrecht, Netherlands, 3Medical Technology & Clinical Physics, University Medical Center Utrecht, Utrecht, Netherlands, 4Department of Radiotherapy, University Medical Center Utrecht, Utrecht, Netherlands, 5Department of Neonatology, University Medical Center Utrecht, Utrecht, Netherlands, 6Computational Imaging Group for MR Diagnostic & Therapy, University Medical Center Utrecht, Utrecht, Netherlands
1Department of Radiology, University Medical Center Utrecht, Utrecht, Netherlands, 2Department of Otorhinolaryngology and Head & Neck Surgery, University Medical Center Utrecht, Utrecht, Netherlands, 3Medical Technology & Clinical Physics, University Medical Center Utrecht, Utrecht, Netherlands, 4Department of Radiotherapy, University Medical Center Utrecht, Utrecht, Netherlands, 5Department of Neonatology, University Medical Center Utrecht, Utrecht, Netherlands, 6Computational Imaging Group for MR Diagnostic & Therapy, University Medical Center Utrecht, Utrecht, Netherlands
Synopsis
In this work, we investigated the noise attenuation provided by different acoustic hood designs particularly relevant for fetal/neonatal MRI and MRI-guided radiotherapy. We experimentally demonstrated that both increasing hood length and thickness have a positive influence on acoustic noise reduction up to 20dB for the investigated scenarios. These results will provide experimental information useful to design a new acoustic hood for different applications, e.g. neonatal MRI and MR-guided radiotherapy.
Introduction
Acoustic noise is a well-known cause of discomfort during MRI and, when hearing protection devices (earplugs/earmuffs/headphones) are not properly used, subjects are at risk of hearing damage. In principle, these devices should provide sufficient protection if correctly worn. This is not the case for patient with, e.g. small ear canals, fetal/neonatal MRI, or patients in immobilization masks undergoing MRI-guided radiotherapy. Previous research proposed the acoustic hood as solution(1). Here, we build upon that work and we investigate the noise attenuation for different hood designs applicable to fetal/neonatal MRI and MRI-guided radiotherapy.Methods
Three acoustic hoods were created, using foam layers (FireSeal or TC2-foam, Easy-Noise-Control, NL), and 1mm-thick polycarbonate (PC) sheet. The latter provides robustness and leads to sound wave reflection inside the foam layers, thus augmenting destructive interferences.We first investigated the impact of adding foam layers to the hood. This hood (Hood 1, Fig. 1) consisted of a wooden frame and the polycarbonate sheet folded between the wooden frame, creating an arc with diameter 476mm and length 1150mm. For each test, a foam layer (FireSeal) of 25mm thickness was added to prototype, first externally to the polycarbonate sheet and afterwards also internally.
The influence of hood length was then investigated (Hood 2, Fig. 1). Hood 2 consisted of a wooden frame and two foam layers (TC2) around the polycarbonate sheet. The starting setup was 1000mm long. For each test, segments of 200mm were added up to a final length of 2000mm.
Finally, a third hood (Hood 3, Fig. 1) was made to investigate the effect of a closed “chamber”. Hood 3 was equal to Hood 2 - length 1000mm. Two plates (each consisting of 2x25mm TC foam with polycarbonate sheet in the middle) were created to close the hood at the feet/head sides. Additionally, two segments of 200mm were applied as in Hood 2 to each side to fixate these plates.
The hood at test was placed inside a 7T Philips Achieva tube and a Polyoxymethylene (POM) plate (covered with foam layer 25mm thick) was used to close its bottom side. Noise attenuation tests were performed in an acoustic room (ISO 8253-2 2012): a microphone (Brüel & Kjær 4189 with ZC-0032 amplifier) was placed in the middle of the hood at test, and four loudspeakers (Yamaha MSP5) were placed around it. Every loudspeaker was separately calibrated to produce a noise level of 55dB(A) (measured with Brüel & Kjær 2250-S) in the test condition without the hood (see fig. 1).
For each test, three measurements were performed: 1) feet/head speakers ON, 2) left/right speakers ON, and 3) all four speakers ON.
Results
Figure 2 shows the measured dB(A) for Hood 1. We observed a steady decrease of sound levels measured inside the bore for the different tests. Ultimately, the achieved noise reduction was 5.5dB when all speakers were active.Figure 3 shows the measured dB(A) for Hood 2. Increasing noise reduction was observed for increasing hood lengths. A total reduction of 12.5dB was registered for Hood 2 with 2000mm length compared to the reference measurement. Additionally, when comparing Hood 2 (I) to Hood 1 (F), which have the same geometrical constructions but different foam materials, an additional reduction of about 5dB is observed, confirming what indicated by the supplier, i.e. TC2-foam has a 2x higher absorption rate than that TC2-foam as an absorption rate almost twice as FireSeal foam.
Figure 4 shows the measured dB(A) for Hood 3. These results show a considerable noise reduction, i.e. about 20dB, when the feet/head plates are included.
Discussion
Using Hood 1, consisting mostly out of FireSeal foam, the noise decreases with 5.5dB. The TC2-foam improved the decrease to 9.8dB. When a longer hood was tested, a noise decrease of 12.5dB was measured. By creating a sort of 'hood chamber' (Hood 3), noise could even be decreased by about 20dB.For the realization of an acoustic hood in clinical settings, it should be noted that a chamber might not be indicated for neonatal scans, as infants are regularly checked, while a thickness of 2x25mm foam might not be applicable for all adults scanned in a small-bore MRI.
In the light of these results, which give experimental indications for acoustic hoods constructions, we believe that a 2000 mm length hood with two foam layers around a PC plate would be an applicable solution for both fetal/neonatal MRI and MR-guided radiotherapy exams. For the latter, the possibility to extend the hood into a sort of chamber could also be possible. This is particularly important for radiotherapy patient, scanned with immobilization masks, since only inner earplugs are currently used for these patients.
Ultimately, these tests were performed using a 7T body coil. These hoods can also be used in diagnostic settings at lower field strengths, where larger body coils are available, thus allowing in principle for thicker foam layers and therefore more noise damping.
Conclusion
We demonstrated that both increasing hood length and thickness have a positive influence on acoustic noise reduction up to 20dB for the investigated scenarios. These results provide experimental information to design an acoustic hood for e.g. fetal/neonatal MRI and MR-guided radiotherapy.Acknowledgements
No acknowledgement found.References
1. A. Nordell, M. Lundh, S. Horsch, B. Hallberg, U. Aden, B. Nordell, M. Blennow. The acoustic hood: A patient-independent device improve acoustic noise protection during neonatal magnetic resonance imaging. 01-07-2009.Figures

Fig 1: The three hood
designs. Hood 1 with all layers of sound damping materials in place (they were
added one by one each step), Hood 2 with two out of five extensions, Hood 3
with two extensions and feet/head plates, and a photo of the testing in the
audio room (the speakers around the setup are marked with red arrows).

Fig. 2: Top:
Different setups of Hood 1: No hood. A: PC plate only. B: Setup A + outer foam
layer. C: Setup B + inner foam layer. D: Setup B + foam layer on table. E: Setup C + foam layer
on table. Bottom: measured dB(A) for these setups.
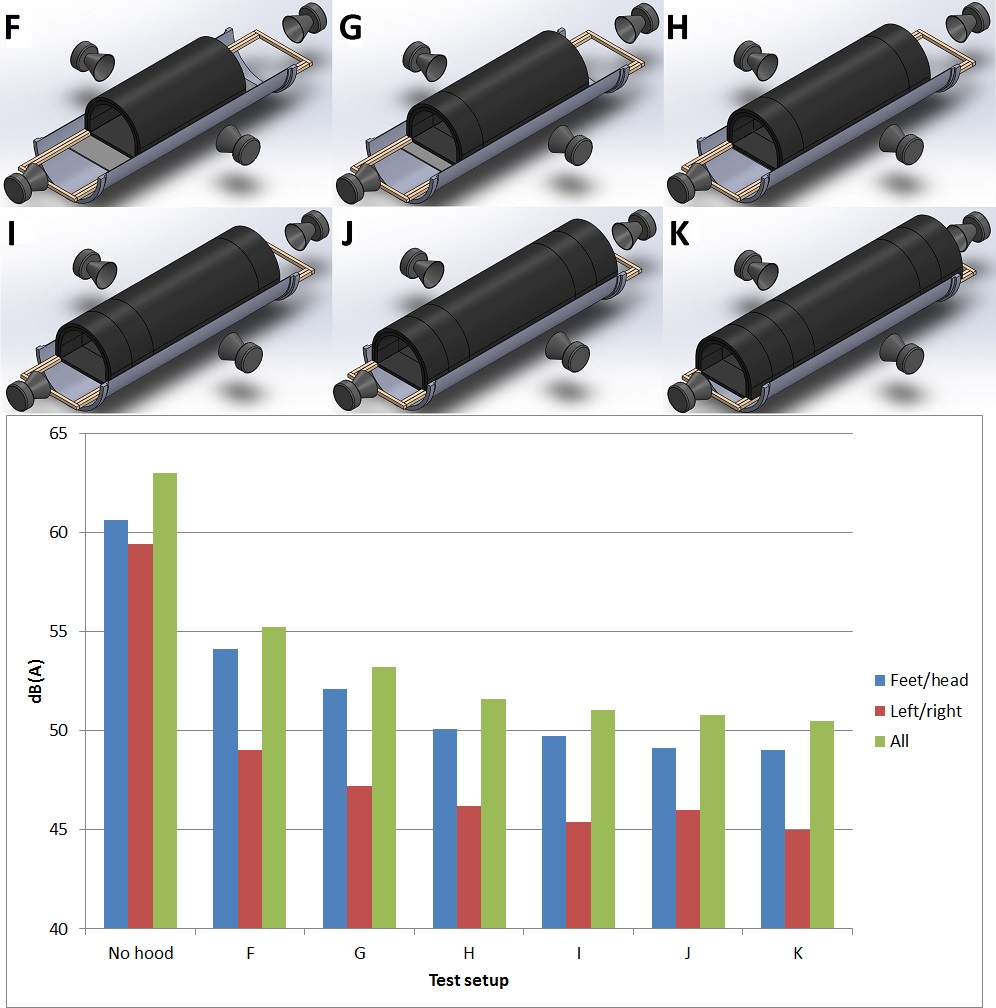
Fig 3: Top: different setups of Hood 2. F: acoustic hood
without any extension (1000mm). G: one extension (1200mm). H: two extensions
(1400mm). I: three extensions (1600mm). J: four extensions (1800mm). K: five
extensions (2000mm). Bottom: measured dB(A) of each setup. No hood: Measurement
without test setup (reproduction of no hood of fig. 2).
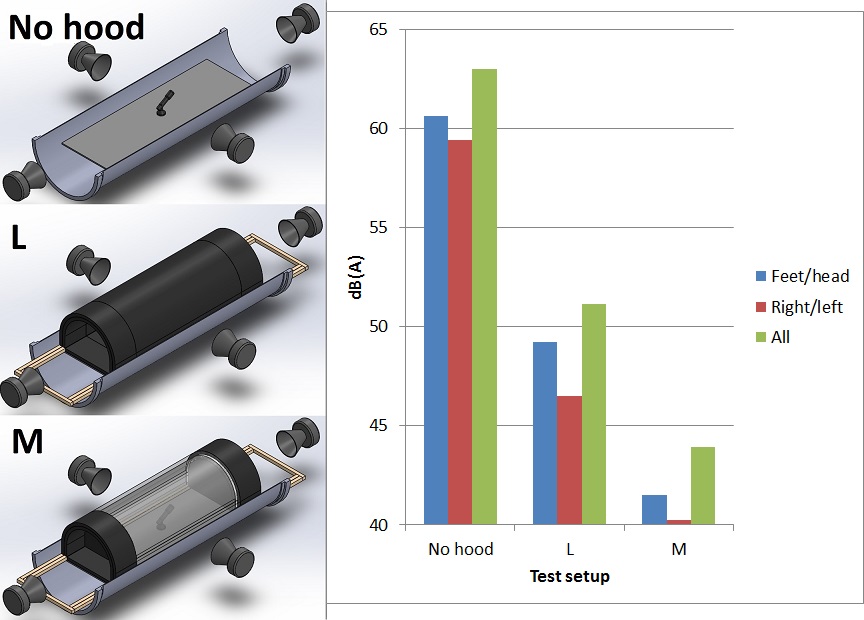
Fig 4: Left:
different setups of Hood 3. No hood (same measurement as no hood of fig. 3). L:
hood with two extensions (reproduction of setup J, fig. 3). M: addition of two
walls to create a chamber (center part made see-through for illustration).
Right: measured dB(A) of each setup.