4164
Diffusion and Dynamic Contrast-enhanced MRI for Evaluation of Prostate Response to 90Yttrium Radioembolization in A Canine Hyperplasia Model1Radiology, Northwestern University, Chicago, IL, United States, 2Research Resource Centers, University of Illinois at Chicago, Chicago, IL, United States, 3Radiology, University of Chicago, Chicago, IL, United States
Synopsis
Management options for localized prostate cancer have largely remained the same for the past 30 years. 90Yttrium (90Y) radioembolization is a novel radiotherapy approach that offers the potential to deliver high-dose radiation therapy with minimal non-target radiation. However, currently no accurate way exists to evaluate radiation effects noninvasively following embolization. In this study, we sought to apply diffusion and dynamic contrast-enhanced perfusion MRI to investigate assess the effects of treatment following 90Y prostate artery radioembolization in a dog prostate model.
Introduction
Prostate cancer is the second most common cancer in men worldwide. Management options for localized prostate cancer have largely remained the same for the past 30 years.1 90Yttrium (90Y) radioembolization offers the potential to deliver high-dose radiotherapy for prostate cancer with minimal non-target radiation.2 However, while this novel approach is currently being carried out, there is a need to evaluate radiation effects upon the prostate. The objective of this preliminary study was to assess the response of prostate tissue to 90Y prostate artery radioembolization using diffusion and dynamic contrast-enhanced (DCE) MRI in a dog prostate hyperplasia model.Methods
Canine model: All the experiments are approved by the Institutional Animal Care and Use Committee. Four male 10-14 kg castrated beagles were treated with hormones for 3 months, per the model for benign prostatic hypertrophy induction in canines.390Y administration: Each dog was catheterized through femoral artery approach with a 2.1 F catheter (Merit Medical, South Jordan, UT) under fluoroscopy. The catheter was used to select the right or left prostatic artery for delivery 90Y microspheres to one lobe of prostate gland with contralateral side serving as a control. Under fluoroscopic control, the microspheres (approximately 100 Gy dose) were administered.
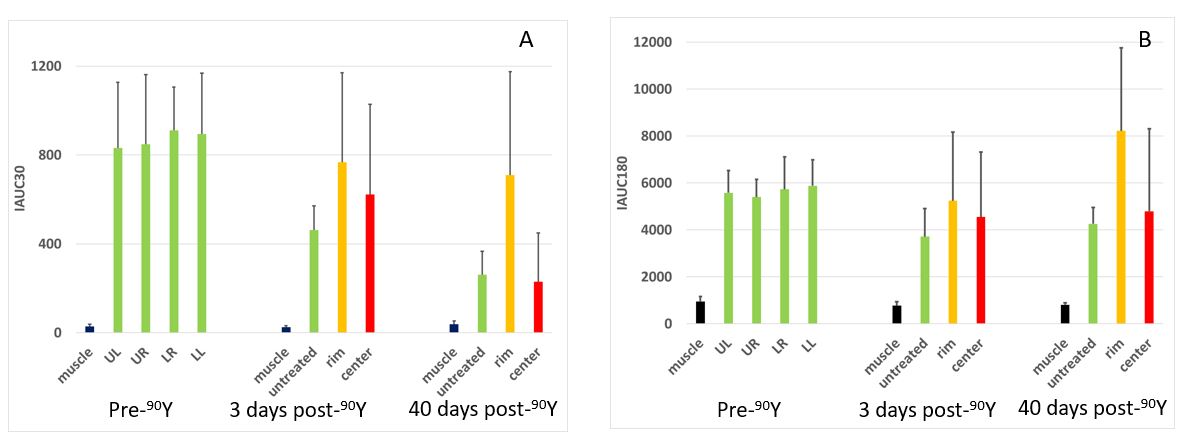
MRI: All MRI studies were performed using 1.5T Siemens Aera. Beagles were scanned prior to, 3 and 40 days post-90Y radioembolization and were anesthetized with isoflurane during MRI measurements. Multiparametric MRIs were acquired with T2-weighted, T1-weighted, diffusion-weighted and dynamic contrast-enhanced (DCE) MRI. T2-weighted turbo spin echo was acquired with the following parameters: repetition time (TR)/echo time (TE) = 4,000/67 ms; field of view (FOV) = 135 x 160 mm2; matrix size = 320 x 270; turbo factor = 23, slice thickness = 1.1 mm. Diffusion imaging was performed using a diffusion-weighted SE-EPI sequence with b-values of 400, 600, 800 s/mm2 and other parameters: TR/TE = 4100/64 ms, FOV=137x 200 mm2, thickness = 1.5 mm, matrix size 176 x 256. Gadopentetate dimeglumine (Magnevist, Bayer Healthcare) was injected intravenously as a rapid bolus (0.1 mmol/kg) at a rate less than 10 mL per 15 seconds. Contrast uptake was followed for 5 minutes with DCE-MRI. The DCE-MRI acquisition consisted of a 3D VIBE dynamic acquisition with the following parameters: TR/TE = 4.47/1.81 ms, FOV=159 x 159 mm2, matrix size = 192 x192, flip angle = 12°, slice thickness = 3 mm, and a temporal resolution of 2.8 sec. A post-contrast T1-weighed VIBE scan with fat saturation was performed with scanning parameters: TR/TE = 9/2.38 ms, FOV = 160 x 160 mm2, matrix size = 224 x 224, flip angle = 10°, slice thickness = 1 mm, scan time = 4 min. Image post-processing was performed in MATLAB (MathWorks). Signal-to-noise ratios (SNRs) were calculated from regions of interest (ROIs) manually drawn in muscle, normal prostate, center of the treated region, and rim of the treated region. Initial area under the curve (IAUC) for Gd was calculated with integration times of 30 and 180 second post–contrast infusion (IAUC30 and IAUC180).4 Apparent diffusion coefficient (ADC) map was generated with a monoexponential fitting.
Results
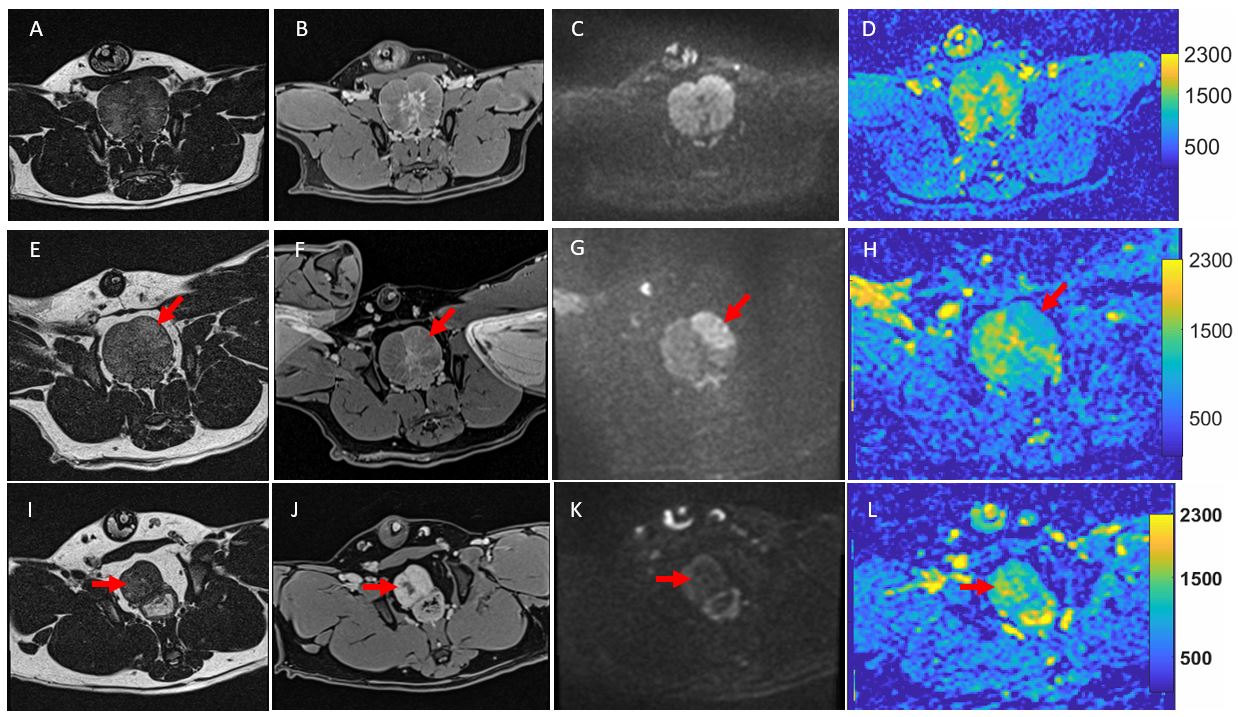
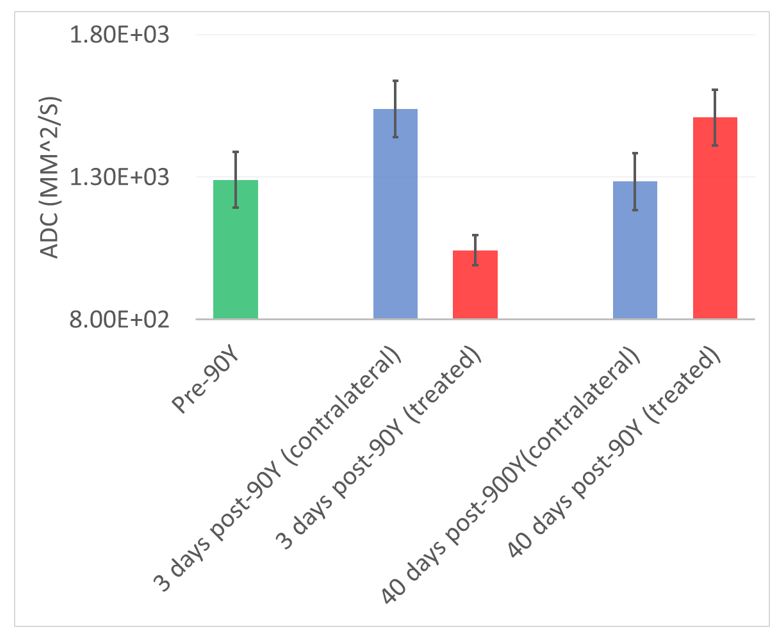
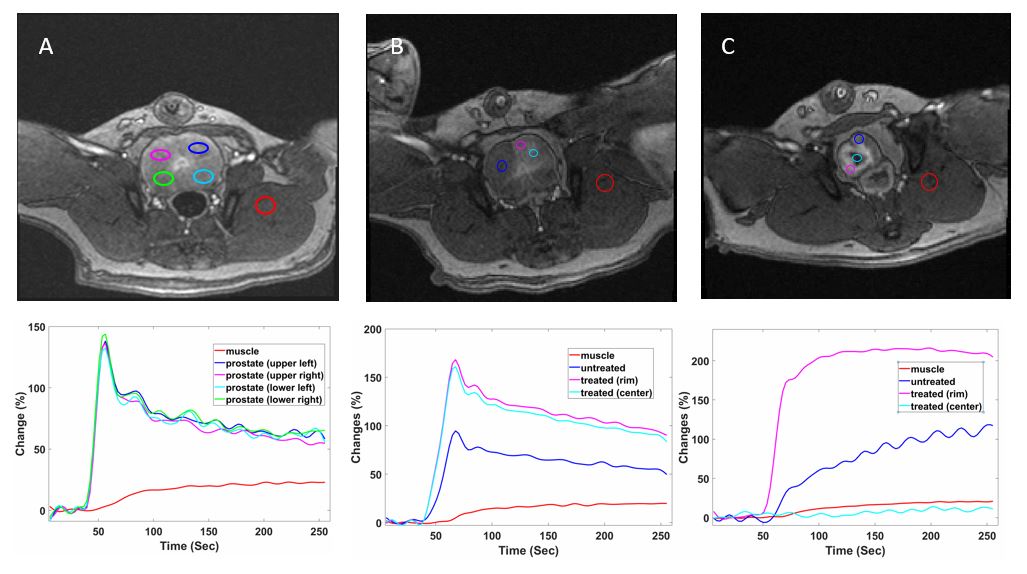
Representative images of T2-weighted, post contrast T1-weighted, diffusion-weighted, and diffusion maps at pre-, 3 and 40 days post-90Y radioembolization are shown in Fig. 1. Compared to the pre-treatment images (top panel in Fig. 1), T2-weighted images (Fig. 1A, E, I) and post contrast T1-weighted images (Fig. 1B, F, J) showed only weak increase of image intensity in the 90Y treated lobe of prostate (arrows). As shown in Fig. 2., ADC was found decreased in the treated lobe and increased at the contralateral control side at 3 days post-90Y when compared to measurements pre-90Y. However, an increased ADC was found in the treated lobe at 40 days post-90Y (Fig 1 and 2). The 90Y treated regions showed more signal enhancement compared to the contralateral control regions in the DCE T1-weighted images 3 days post-90Y radioembolization (Fig. 3B) and the rim of the treated regions showed more signal enhancement at 40 days post-90Y (Fig. 3C and Fig. 4). The calculated IAUC values showed changes in treated and contralateral control regions of the prostate with time, while those of neighboring muscle remained stable (Fig. 4).Discussion
Focal therapies for prostate cancer represent the next major advancement in prostate cancer therapy. 90Y radioembolization offers the potential to deliver high-dose radiation therapy with minimal non-target toxicity. In this study, our results indicated that both 90Y treated lobe and untreated contralateral control of prostate show changes in diffusion and DCE perfusion parameters at short-term (3 days) and relative long-term (40 days) post-90Y radioembolization.Conclusion
90Y radioembolization is a novel radiotherapy approach that offers the potential to deliver high-dose radiation therapy with minimal off-target toxicity. This preliminary study showed that diffusion and DCE MRI are sensitive to 90Y radioembolization therapeutic effects in the prostate.Acknowledgements
This research was supported by NCI grant Number RO1CA181658 and grant from BTG.References
1. Siegel RL, Miller KD, Jemal A. Cancer statistics, 2018. 2018; 68(1): 7-30.
2. Zaorsky NG, Davis BJ, Nguyen PL, et al. The evolution of brachytherapy for prostate cancer. Nature Reviews Urology 2017; 14: 415.
3. DeKlerk DP, Coffey DS, Ewing LL, et al. Comparison of spontaneous and experimentally induced canine prostatic hyperplasia. J Clin Invest. 1979 Sep; 64(3):842-9.
4. Chung WJ, Kim HS, Kim N, et al. Radiology. 2013 Volume 269: Number 2—November 2013 https://doi.org/10.1148/radiol.13130016.
Figures