4158
Total cost of ownership is a useful tool for life cycle management of MRI scanners and managing costs in an MRI department.1Radiology, NIH Clinical Center, Bethesda, MD, United States
Synopsis
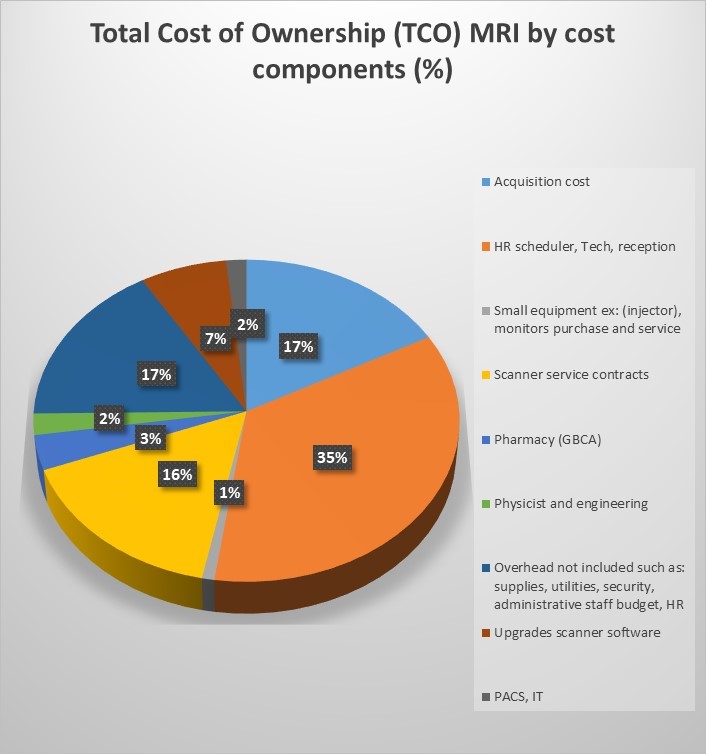
A total cost of ownership (TCO) model was developed for MRI scanners over the ownership life from fund allocation through decommissioning in an organization with outpatient, inpatient and research scanners. The TCO model included acquisition and installation costs; site modifications to comply with safety requirements; human resources including ancillary personnel; small equipment, supplies, contrast; service contracts; IT; overhead; and upgrades. The largest expense was human resources accounting for 35% of TCO. A cost reduction strategy is centralized remote scanning, reducing the total number of highly skilled technologists. TCO is tool for identifying hidden costs and comparing scenarios for managing costs.
Introduction
The concept of total cost of ownership (TCO) was developed initially to assist in strategic business decisions in IT systems and has been applied to many other areas including facilities and large hospital equipment1,2. The aim was to develop a model to use TCO to prioritize and support life cycle management of a suite of MRI scanners and to compare variables that contribute to acquisition, operation and human resource costs in order to make informed management choices. Exploring high value MRI, shortened protocols and efficiencies is an important mission. However, understanding true costs of MRI operations is also important. Awareness of the entire cost and value chain in imaging and methods that business managers and hospital or practice leaders use to make decisions may allow radiologists an increased role in strategic decisions in the organization3.Methods
A model was developed for TCO of MRI scanners in an organization which includes outpatient, inpatient and research scanners. A thorough accounting of all costs for acquisition, human capital and operations was performed with explicit search for and consideration of “hidden costs.”First steps in TCO were to define ownership life, considered as the actual number of years based on average time to from fund allocation for scanner purchase through design, installation, and operations until decommissioning. Costs for new scanner purchase and installation included design, architectural and engineering consultation; room/facility reconfiguration; physician and medical physicist time to evaluate scanners and the design.
Other infrastructure costs included reconfiguration of space for additional safety zones per updated guidelines, electronic security devices for facility security, and technologist applications training.
Thorough review of hidden costs for MRI operations included more complete accounting for all human resource costs in salary, benefits, and training, needed to support operations, including appointment schedulers, reception staff, MRI technologists, IV technicians/nurses, and supervisory technologists. A supply chain technician was modeled to order and replenish supplies, e.g., IV access and pharmaceuticals (contrast), rather than assigning these tasks to technologists. Average cost of living increases were incorporated in the model.
Costs of small equipment such as monitoring devices, injectors, supplies (e.g., IV access, contrast agents) were included. IT support included PACS operations, image storage and user support. Ongoing costs include scanner service contracts, infrastructure and utility costs (power, chilled water HVAC, which could only be estimated based on overhead from accounting services because of the hospital setting). Projected medical inflation rate was estimated and added to model for variables such as small medical equipment replacement and service, supplies, contrast agents, scanner service contracts and upgrades.
Physician interpretive time was not included in human capital expenses in this model, though may be included in TCO in some practice settings.
Results
A TCO model for a single scanner is shown in Figure 1. The highest cost related to operations was human capital (35%). Cost of purchase with 10-year ownership life of an MRI, on average, accounted for only 17%.Strategies to minimize costs were introduced into the model such as remote scanning by centrally located technologists which may be applicable to sites where imaging centers are in remote locations or spread throughout a metropolitan area. This strategy changes the mix of skillset among staff, with fewer highly skilled technologists, but increases IT support and equipment costs to deploy. The TCO can be used to compare tradeoffs between increased IT costs, decreased human capital costs and the number of scanners or sites that would be needed to realize savings. Because of the significant component of cost due to human capital, strategies employing fewer highly paid technologists is projected to have a financial advantage despite increased IT expenses to implement remote scanning. This may be financially beneficial in large practices or settings across the globe with scanners in more remote locations where there are fewer skilled technologists.
In our setting a complete TCO was not performed but would incorporate expected revenues and compare the ROI with alternative decisions, i.e., no purchase, delayed purchase or lease.
Discussion
Though the complete TCO includes additional steps incorporating revenues by scanner or center, the earlier steps provide useful lessons for understanding and predicting cost savings within a department. Full consideration of costs may alter impressions of expected cost savings and facilitate informed decision making.Limitations of TCO and this study include inaccurate indirect costs such as administrative overhead which do not correspond directly to MRI's use of these resources. However, most internal scenarios we modeled do not depend on this cost component.
Limitations of TCO in general are that it does not account for benefits such as increased overall patient recruitment to a facility by offering a new or unique MRI capability. In a similar manner, it does not account for benefits such as improved patient safety or employee satisfaction.
Conclusion:
TCO is a useful tool for identifying hidden costs, comparing scenarios for managing and decreasing costs and supporting organizational strategy.Acknowledgements
Clinical Center Budget Office and Administrative staff for gathering data on costs.References
Lisa M Ellram, Sue P Siferd. Total cost of ownership: A key concept in strategic cost management decisions. Journal of Business Logistics, 1998; 19(1):55-76
Matthias Weber, Michael Hiete, Lars Lauer, Otto Rentz. Low cost country sourcing and its effects on the total cost of ownership structure for a medical devices manufacturer. Journal of Purchasing and Supply Management 2010;
16(1):4-16
Geoffrey D Rubin. Costing in Radiology and Health Care: Rationale, Relativity, Rudiments, and Realities. Radiology, 2017; 282(2):333-347.
Figures