4157
Free-breathing 3D T2-weighted TSE using Cartesian acquisition with rewinded spiral profile ordering (rCASPR) for abdominal radiotherapy1Department of Radiotherapy, University Medical Center Utrecht, Utrecht, Netherlands, 2Computational Imaging Group for MRI diagnostics and therapy, Centre for Image Sciences, University Medical Center Utrecht, Utrecht, Netherlands, 3Department of Biomedical Engineering, Eindhoven University of Technology, Eindhoven, Netherlands
Synopsis
T2-weighted turbo spin-echo (TSE) sequences are used for abdominal tumour contouring in MR-guided radiotherapy, but these sequences are generally not compatible with most respiratory-correlated 4D imaging methods. To overcome this limitation we propose a free-breathing T2-weighted TSE sequence based on a Cartesian acquisition with rewinded spiral profile ordering in combination with motion compensated image reconstruction. We showed that high quality free-breathing T2-weighted TSE scans are feasible with short scan times (<5 min), which have similar contrast to the conventional linear sampled scans while simultaneously quantifying the respiratory motion.
Introduction
The excellent soft tissue contrast of MRI is exploited in radiotherapy to facilitate tumour and organ visualisation with simultaneous respiratory motion quantification1. The quantified motion can be used to account for respiration during radiotherapy2 or to improve image reconstruction quality for accurate contouring. Abdominal tumors are often contoured, using 3D turbo spin-echo (TSE) images, but these sequences are generally incompatible with most respiratory-correlated 4D imaging methods3. Due to this incompatibility, most protocols require two separate scans to both reconstruct a T2-weighted TSE and the corresponding respiratory motion4. However, the respiratory motion is not synchronized with the TSE acquisition and therefore cannot be used to improve the image reconstruction quality. To overcome this limitation we propose a free-breathing 3D T2-weighted TSE sequence based on a cartesian acquisition with rewinded spiral profile ordering (rCASPR) in combination with motion compensated image reconstruction (MCIR)5. The key idea of the sequence is to enable free-breathing 3D TSE, while minimizing changes in image contrast compared to the conventional linear cartesian acquisition while simultaneously quantifying the respiratory motion.Theory
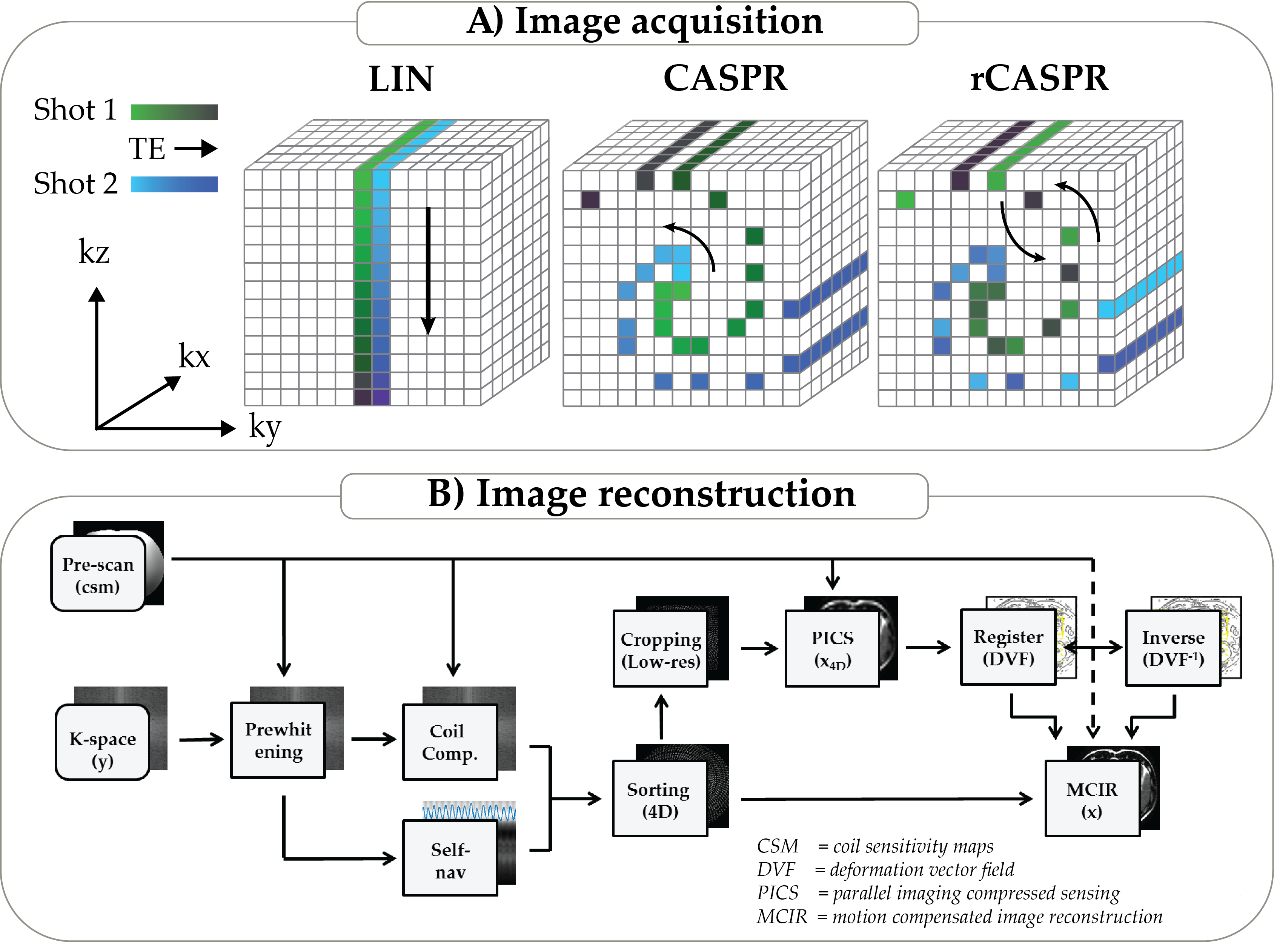
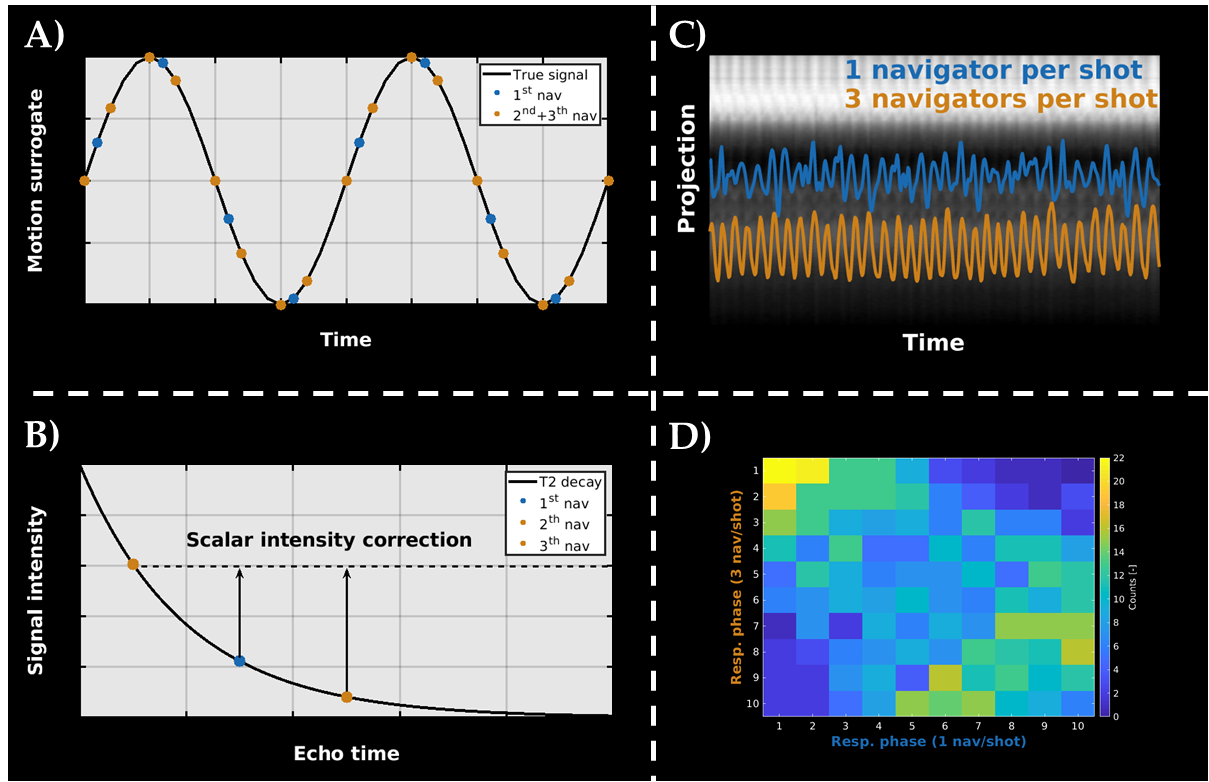
Cartesian acquisition with rewinded spiral profile ordering (rCASPR):CASPR acquires linear profiles along a spiral interleave on a cartesian grid6, where the number of profiles equals the TSE shot length (Figure-1A). These profiles are sampled from the center towards the periphery, which yields a much shorter effective echo time (Teff) compared to the conventional linear (LIN) profile ordered acquisition. We modified CASPR to consist of a rewinded (in-out) spiral trajectory (rCASPR) to yield comparable Teff as LIN, in which the feet-head projection line (ky,z = 0) is sampled every TSE shot. In addition, we sample ky,z = 0 at the beginning and at the end of the TSE shot to increase the temporal resolution for self-navigation (Figure-2A).
Respiratory-resolved deformation vector field reconstruction:
The MCIR requires deformation vector fields (DVFs), which were approximated using a respiratory correlated 4D image reconstruction7,8. The k-space data was sorted into 10 respiratory phases and reconstructed with parallel imaging (PI) and compressed sensing (PICS) using the BART toolbox9 :
\begin{eqnarray}arg\min\limits_{x_{4D}} \ || FSx_{4D} - y ||^2 + ||TVx_{4D}||^1\end{eqnarray}
Here F is the Fourier operator, S the coil sensitivities and TV the spatiotemporal finite difference operator. To further reduce the sampling requirements, the images were reconstructed with reduced spatial resolution (4mm3), which is sufficient for accurate motion estimation10. The reconstructed x4D were jointly non-rigidly registered to the time-averaged position11 using nD + t B-splines and a groupwise optimization approach12. The joint registration reduces potential bias in the DVFs due to residual undersampling artefacts. The inverse deformation vector fields (DVF-1) were computed using an iterative inversion method13. For a schematic overview of the reconstruction algorithm see Figure-1B.
Motion compensated image reconstruction (MCIR):
The DVFs were incorporated in the final MCIR8 and optimization was performed using nonlinear conjugate gradient implementation in Matlab:
\begin{eqnarray}arg\min\limits_{x} \ || FSUx - y ||^2 + ||TVx||^1\end{eqnarray}
Here U is the operator that warps the images to the exhale position using the DVFs and TV is the spatial finite difference operator.
Imaging experiments
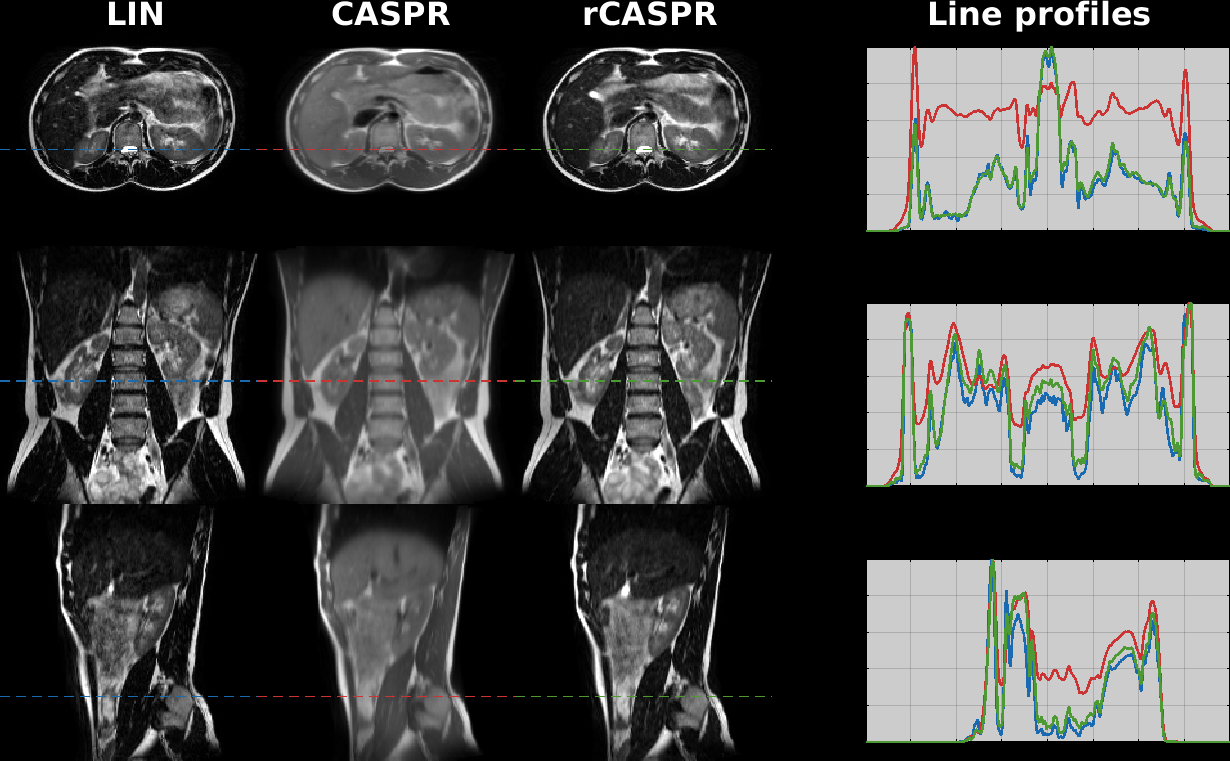
Comparison of image contrast - LIN vs rCASPR:To investigate the differences in image contrast and image quality between the rCASPR and LIN, 2 volunteer data-sets were acquired on a 1.5T (Ingenia MR-RT, Philips Healthcare, The Netherlands). Scan times of both sequences were matched to 248s. Other sequence parameters can be found in the caption of Figure-3. The images were qualitatively compared by inspection of the line profiles.
Comparison of image quality - LIN vs MCIR rCASPR:
To investigate the improvement in image quality of the proposed MCIR rCASPR two additional scans were acquired in two volunteers in the abdomen. Scan 1: LIN free breathing TSE; Scan 2: rCASPR TSE. In addition to the conventional reconstruction, scan 2 was reconstructed using soft-gated PICS (SG-PICS) for comparison14. Image quality was compared using the negative log of the gradient entropy (-log(GE)). Scan times of both sequences were matched to 286 s. and other sequence parameters can be found in the caption of Figure-4/5. The added value of the two additional projections was assessed using a confusing matrix, which visualizes differences in the respiratory phase sorting.
Results
Figure-2 shows the improved temporal resolution of the self-navigation signal due to the additional sampling of the feet-head projection in the beginning and end of the TSE train. Note that the respiratory binning yielded different results when 1 or 3 k-space centers were used (Figure-2D). Figure-3 shows the comparison of image contrast between LIN and rCASPR acquisitions. The intensity profiles are in very good agreement between LIN and rCASPR. Figure-4 and Figure-5 show the improvement of MCIR rCASPR compared to free-breathing LIN, which shows sharper image features (also reflected in the gradient entropy measurements).Discussion & Conclusion
We demonstrated that free-breathing T2-weighted TSE sequences are feasible within acceptable scan times (<5 min) using MCIR rCASPR. Figure-4 and Figure-5 show that rCASPR yield image quality improvements over free-breathing LIN acquisitions when using self navigated, motion corrected rCASPR. We anticipate that (r)CASPR readouts in combination with MCIR have the potential to enable free-breathing 3D TSE sequences that facilitate mid-position reconstruction, provide DVFs for motion margins and improve tumor contouring for abdominal radiotherapy treatment planning.Acknowledgements
This work is part of the research program HTSM with project number 15354, which is (partly) financed by the Netherlands Organization for Scientific Research (NWO).References
1. Schmidt MA, Payne GS. Radiotherapy planning using MRI. Phys Med Biol. 2015;60(22):R323-R361. doi:10.1088/0031-9155/60/22/R323
2. W Lagendijk JJ, Raaymakers BW, T Van den Berg CA, Moerland MA, Philippens ME, van Vulpen M. MR guidance in radiotherapy. Phys Med Biol. 2014;59. http://iopscience.iop.org/0031-9155/59/21/R349.
3. Stemkens B, Paulson ES, Tijssen RHN. Nuts and bolts of 4D-MRI for radiotherapy. Phys Med Biol. 2018;63(21). doi:10.1088/1361-6560/aae56d
4. Freedman JN, Collins DJ, Bainbridge H, et al. T2-Weighted 4D Magnetic Resonance Imaging for Application in Magnetic Resonance-Guided Radiotherapy Treatment Planning. Invest Radiol. 2017;52(10):563-573. doi:10.1097/RLI.0000000000000381
5. Batchelor PG, Atkinson D, Irarrazaval P, Hill DLG, Hajnal J, Larkman D. Matrix description of general motion correction applied to multishot images. Magn Reson Med. 2005;54(5):1273-1280. doi:10.1002/mrm.20656
6. Prieto C, Doneva M, Usman M, et al. Highly efficient respiratory motion compensated free-breathing coronary MRA using golden-step Cartesian acquisition. J Magn Reson Imaging. 2015. doi:10.1002/jmri.24602
7. Feng L, Axel L, Chandarana H, Block KT, Sodickson DK, Otazo R. XD-GRASP: Golden-angle radial MRI with reconstruction of extra motion-state dimensions using compressed sensing. Magn Reson Med. 2016. doi:10.1002/mrm.25665
8. Cruz G, Atkinson D, Buerger C, Schaeffter T, Prieto C. Accelerated motion corrected three-dimensional abdominal MRI using total variation regularized SENSE reconstruction. Magn Reson Med. 2016. doi:10.1002/mrm.25708
9. Uecker M, Ong F, Tamir J, Bahri D, Virtue P, Cheng J, Zhang T, and Lustig M. Berkeley Advanced Reconstruction Toolbox, ISMRM 23:2486 (2015)
10. Glitzner M, de Senneville BD, Lagendijk JJW, Raaymakers BW, Crijns SPM. On-line 3 D motion estimation using low resolution MRI. Phys Med Biol. 2015;60(16):N301-N310. doi:10.1088/0031-9155/60/16/N301
11. Wolthaus JWH, Sonke JJ, van Herk M, Damen EMF. Reconstruction of a time-averaged midposition CT scan for radiotherapy planning of lung cancer patients using deformable registration. Med Phys. 2008;35(9):3998-4011. doi:10.1118/1.2966347
12. Metz CT, Klein S, Schaap M, van Walsum T, Niessen WJ. Nonrigid registration of dynamic medical imaging data using nD+t B-splines and a groupwise optimization approach. Med Image Anal. 2011;15(2):238-249. doi:10.1016/j.media.2010.10.003
13. Dubey A, Iliopoulos AS, Sun X, Yin FF, Ren L. Iterative inversion of deformation vector fields with feedback control. Med Phys. 2018;45(7):3147-3160. doi:10.1002/mp.1296
14. Spincemaille P, Liu J, Nguyen T, Prince MR, Wang Y. Z intensity-weighted position self-respiratory gating method for free-breathing 3D cardiac CINE imaging. Magn Reson Imaging. 2011;29(6):861-868. doi:10.1016/j.mri.2011.02.011
Figures