4145
4D-MRI of Thorax and Abdomen with Variable Contrast at 1.5T1Institute for Biomedical Engineering, University and ETH Zurich, Zurich, Switzerland, 2Department of Radiology, Division of Radiological Physics, University Hospital Basel, Basel, Switzerland, 3Department of Biomedical Engineering, University of Basel, Allschwil, Switzerland, 4High Field Magnetic Resonance, Max Planck Institute for Biological Cybernetics, Tübingen, Germany, 5Center for Proton Therapy, Paul Scherrer Institute, Villigen-PSI, Switzerland
Synopsis
Time-resolved volumetric imaging (4D-MRI) of moving organs is essential for several clinical applications, e.g., in interventional treatments, radiation therapies, and high-intensity focused ultrasound ablations. In this work, an interleaved time-resolved data-navigator acquisition strategy for 4D-MRI with flexible contrast is developed offering versatile settings for thoracic and abdominal imaging: for both, image and navigator, not only the flip angle but also the basic acquisition type (pulse sequence kernel) can be chosen independently from either balanced SSFP (i.e., T2/T1-weighted) or spoiled gradient echo (i.e., T1-weighted).
Introduction
Respiratory and organ motion challenge treatments of thoracic and abdominal targets (such as tumors), e.g., during radiotherapeutic interventions or high-intensity focused ultrasound ablations1,2. Hence, these clinical applications strongly rely on real-time and time-resolved volumetric MR imaging, occasionally paired with other imaging modalities such as ultrasonography3 or optical tracking devices4. For treatment planning, accurate organ motion modeling is necessary, while for therapy delivery, highly precise target localization and tracking is crucial.One of the most sophisticated methods for capturing motions and drifts of targeted organs is based on continuous free-breathing acquisitions of 2D data-navigator slice pairs (with moving imaging data-slice and stationary navigator-slice), retrospectively stacked into time-resolved three-dimensional datasets (4D-MRI)5. While data and navigator images generally should have diametrical objectives, i.e., providing pathology-tuned image contrasts (data) and feature tracking for accurate motion modeling (navigator), current implementations do not offer sufficient flexibility since the imaging is performed with identical acquisition types and settings (i.e. pulse sequence kernels and flip angles). Moreover, the magnetization is in quasi steady-state for the navigator (continuously acquired), but in thermal equilibrium for the acquisition of the consecutive data slices, leading to different optimal acquisition parameter settings.
In this work, we thus propose Variable Contrast (VC) data-navigator imaging for 4D-MRI (VC-4DMRI). The implementation offers maximum flexibility, that is, for both, data and navigator images, not only different flip angles (FA) but also the sequence kernel can be set independently to offer either balanced steady-state free precession (bSSFP) or spoiled gradient echo (SPGR) contrast. Generally, VC-4DMRI is developed based on an ultra-fast SSFP kernel6, which offers substantially reduced repetition times and thus artifact-free thoracic bSSFP imaging.
Methods
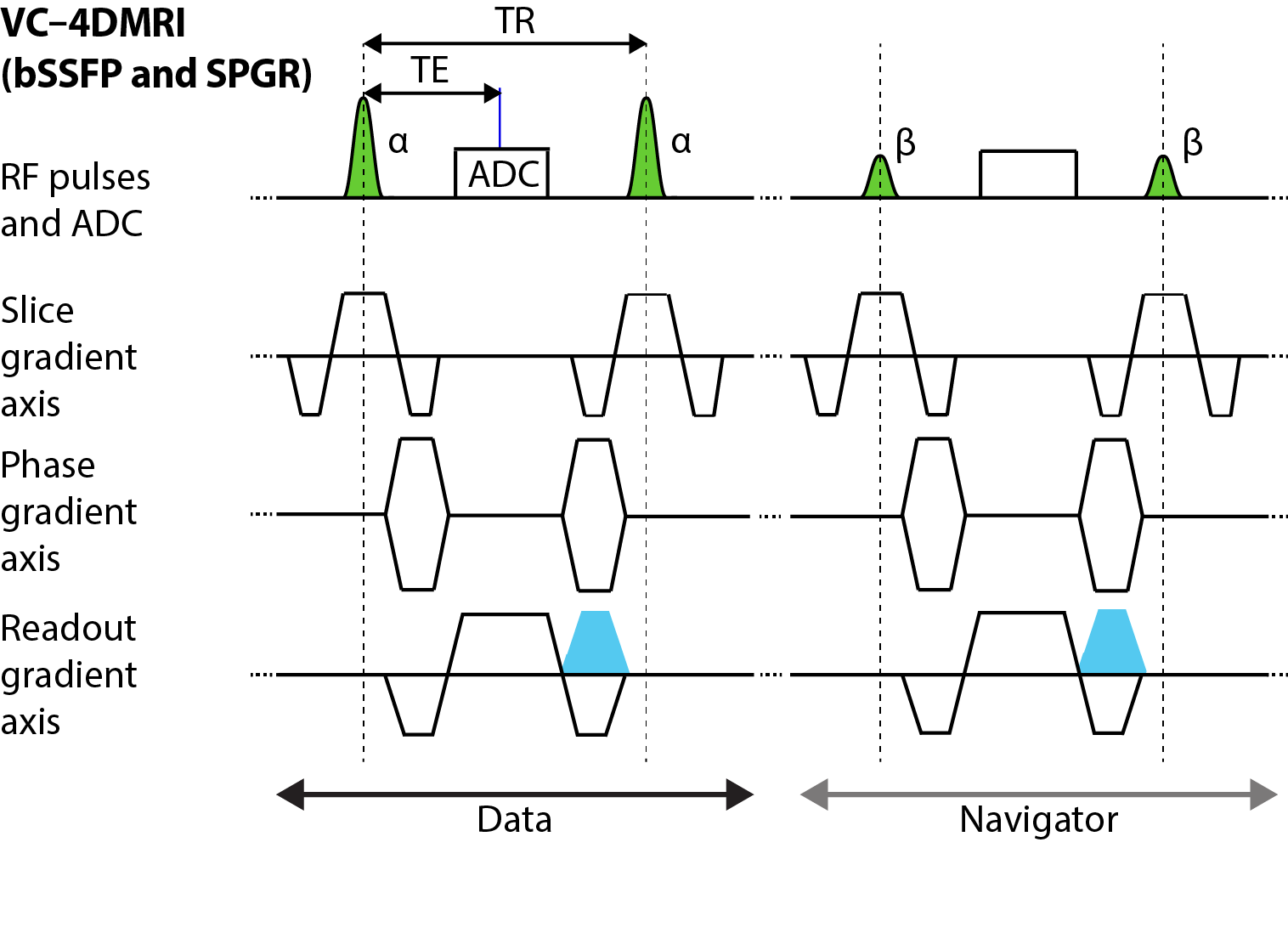
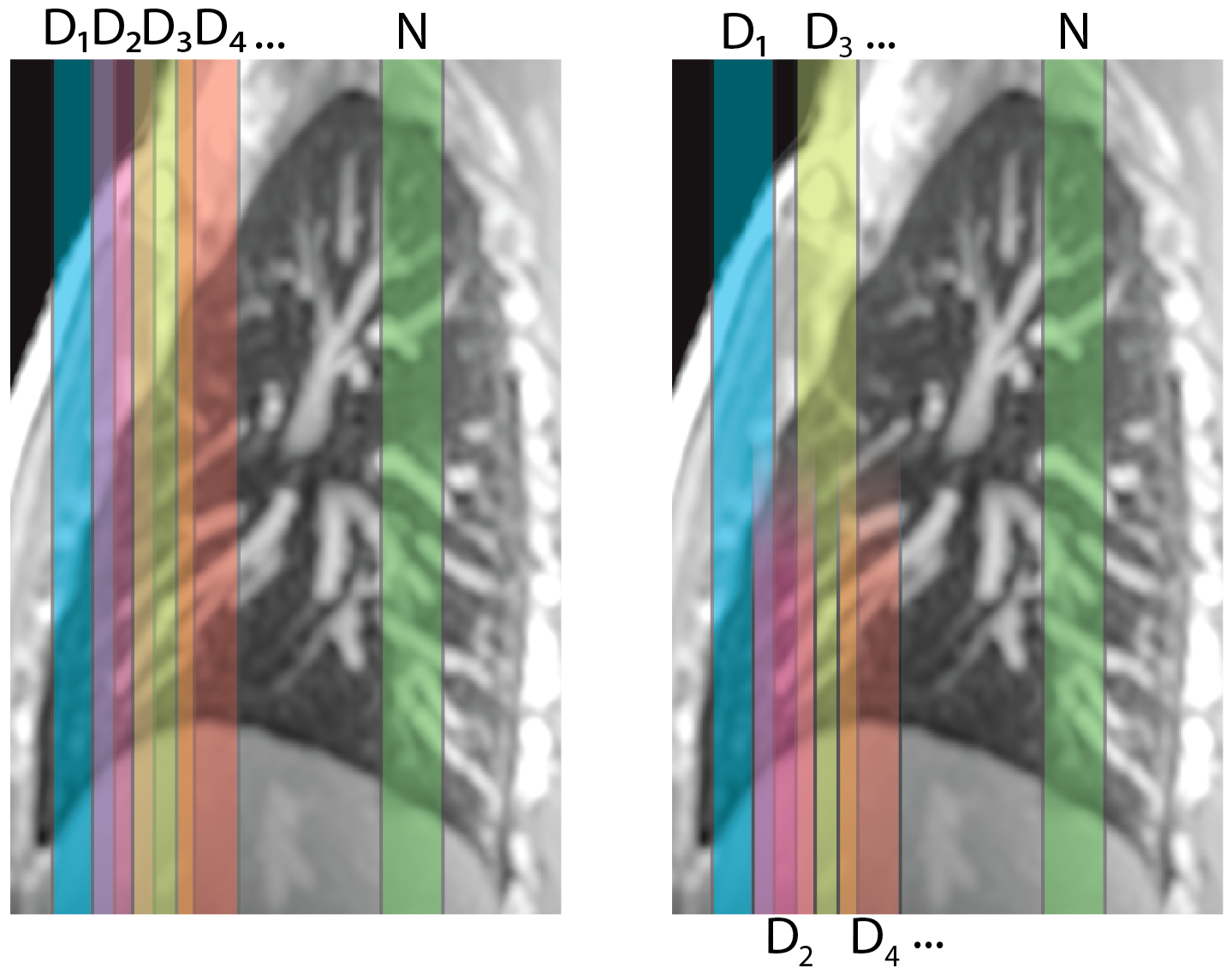
VC-4DMRI was tested in healthy volunteers (in accordance with local ethical guidelines) on a 1.5T whole-body MR-system (MAGNETOM Avanto-Fit, Siemens Healthineers, Erlangen, Germany). A schematic illustration of the proposed VC-4DMRI scheme is shown in Figure 1, allowing selection of a specific contrast, that is T2/T1 (bSSFP) or T1 (SPGR), and a specific flip angle independently for both, data and navigator acquisitions. In addition, an interleaved slice-order acquisition scheme was employed to reduce partial saturation due to the overlapping slices (Figure 2).Imaging was performed in the coronal orientation with a TE/TR = 0.78/1.88 ms, bandwidth = 1860 Hz/pixel, FA = 5-90°, GRAPPA factor 2, partial Fourier factor 7/8, field-of-view = 425×425 mm2, in-plane resolution = 2.2×2.2 mm2 (matrix size = 192×192), slice thickness = 9 mm, slice overlap = 35% (see Figure 2), acquisition time per image = 205 ms (i.e., sampling frequency = 5Hz).
Image stacking into 4D datasets was performed according to von Siebenthal et al.5, but by using a thorax-specific image registration approach7 for determining the respiratory state.
Results
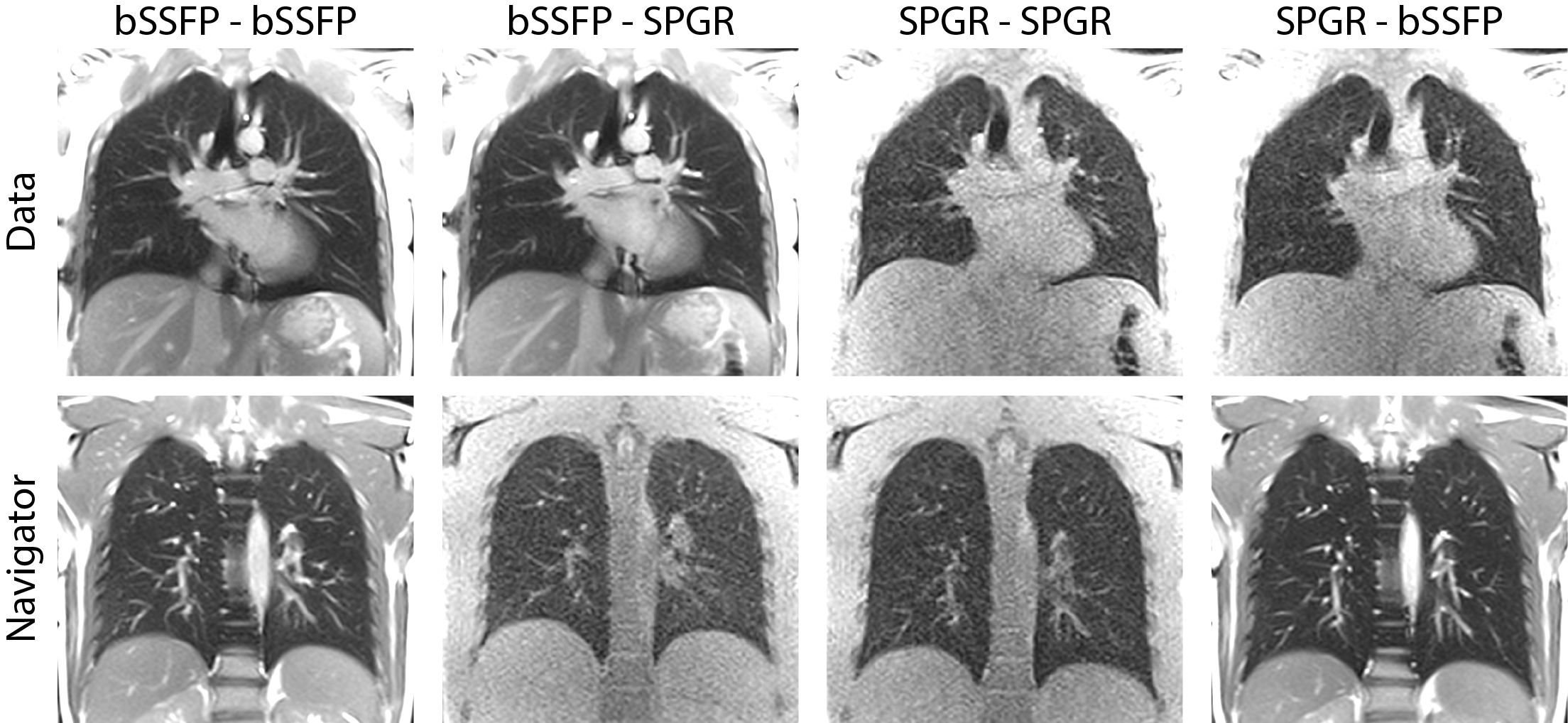
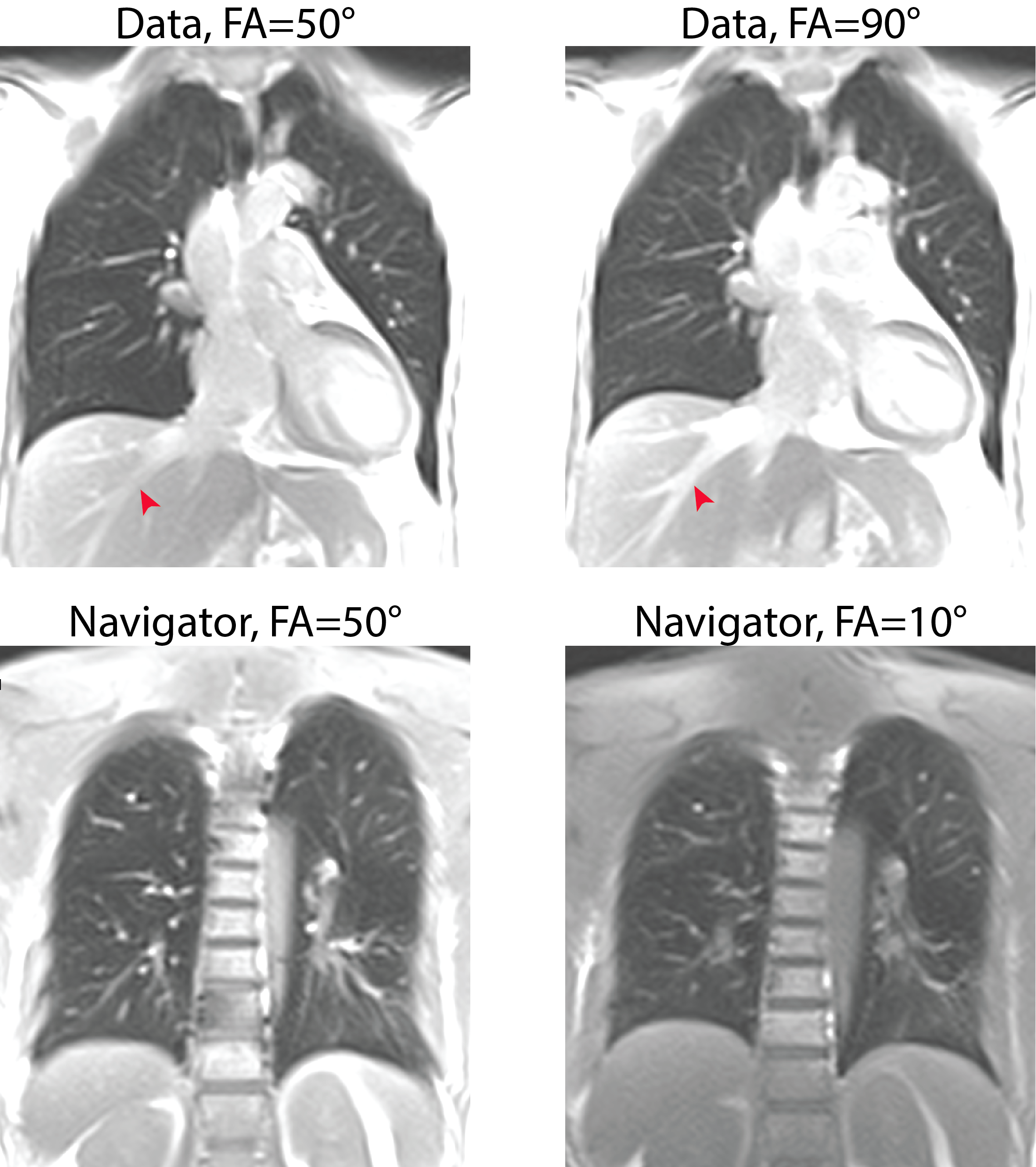
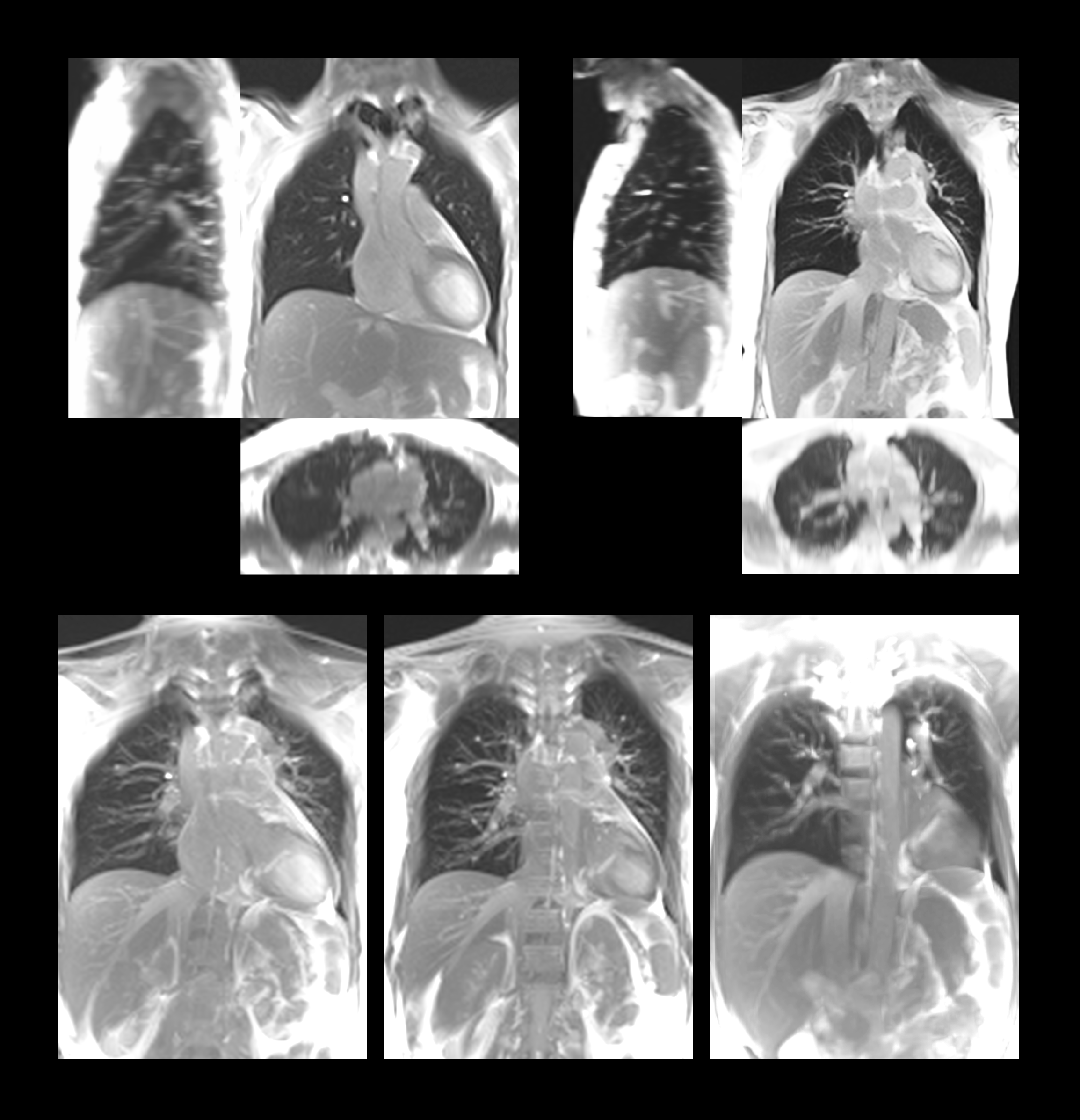
Representative data-navigator acquisitions with VC-4DMRI using bSSFP-T2/T1 and SPGR-T1 contrasts are shown in Figure 3. Both pulse sequences (bSSFP and SPGR kernels) offer artifact-free thorax images. Vessels and fine vascular structures are well discernible in bSSFP, which clearly delivers a higher signal-to-noise-ratio (SNR) in comparison to SPGR (SNR bSSFP ≈ 35, SNR SPGR ≈ 11). In the spine and next to the ribcage, bSSFP suffers from signal drops. The interleaved slice-order acquisition scheme (see Figure 2) provides a signal increase of about 8% in the lung parenchyma and in the liver as compared to the sequential slice-order acquisition scheme.The versatility of adapting the flip-angle for data and navigator imaging can be appreciated in Figure 4. VC-4DMRI offers for instance an improved discrimination of the hepatic vessels from the surrounding liver tissue using bSSFP with a very large FA (here 90°). Such a high FA for data-slices is only achievable combined with low-FA bSSFP or SPGR navigator-slices (here bSSFP with 10°) due to specific absorption rate (SAR) constraints (SAR$$$\propto$$$FA2).
Finally, a representative volume of a reconstructed VC-4DMRI dataset is shown in Figure 5. With the proposed setup, i.e. low-FA navigator combined with high-FA data-slices and both set to bSSFP contrast, time-resolved volumetric reconstructions are exceptionally improved since no saturation of signal is discernible around the navigator plane, as commonly observed with conventional approaches (i.e. using the same FA for data and navigator3).
Discussion and Conclusion
In this work, we have broadened and improved contemporary 4D-MRI with the possibility to acquire data and navigator slices with variable contrasts, allowing dedicated, versatile and optimized protocol settings for motion detection and target imaging with optimal contrast and improved SNR.VC-4DMRI provides time-resolved volumetric imaging, e.g., of lung and liver with flexible contrast, high frame rate and high resolution (here: 2.5Hz for data slices, 2.2×2.2×5 mm3 after stacking reconstruction). In general, bSSFP acquisitions appear superior to SPGR, nevertheless the SPGR contrast might be advantageous for an improved differentiation and characterization of e.g. tumor tissues, or for imaging at field strength higher than 1.5T.
In summary, VC-4DMRI offers excellent prospects for time-resolved volumetric imaging of thoracic and abdominal organs during free-breathing with wide contrast flexibility for treatment planning and interventions.
Acknowledgements
This work was supported by the PHRT Initiative of the ETH Domain, Switzerland.References
1. Bert C and Durante M. Motion in radiotherapy: particle therapy. Phys. Med. Biol. 56, 2011, R113.
2. Celicanin Z, Auboiroux V, Bieri O, et al. Real-time method for motion-compensated MR thermometry and MRgHIFU treatment in abdominal organs: MRgHIFU treatment method in abdominal organs. Magn Reson Med 2014;72:1087–95.
3. Giger A, Stadelmann M, Preiswerk F, et al. Ultrasound-driven 4D MRI. Phys Med Biol. 2018 Jul 16;63(14):145015.
4. Fattori G, Safai S, Carmona PF, et al. Monitoring of breathing motion in image-guided PBS proton therapy: comparative analysis of optical and electromagnetic technologies. Radiat Oncol 2017; 12:63. 10.1186/s13014-017-0797-9.
5. Von Siebenthal M, Székely G, Gamper U, et al. A 4D MR imaging of respiratory organ motion and its variability. Phys. Med. Biol., 2007, 52 1547.
6. Bieri O. Ultra-fast steady state free precession and its application to in vivo 1H morphological and functional lung imaging at 1.5 tesla. Magn Reson Med 2013; 70:657–663.
7. Sandkühler R, Pezold CS, Cattin P.C, et al. Adaptive graph diffusion regularisation for discontinuity preserving image registration. Int. Workshop on Biomedical Image Registration. Springer, Cham, 2018.
Figures