4138
Multi-Radiofrequency Thermal Magnetic Resonance Targeting Glioblastoma Multiforme1Berlin Ultrahigh Field Facility (B.U.F.F.), Max Delbrück Center for Molecular Medicine in the Helmholtz Association, Berlin, Germany, 2MRI.TOOLS GmbH, Berlin, Germany, 3Clinic for Radiation Oncology, Charité Universitätsmedizin, Berlin, Germany, 4Experimental and Clinical Research Center (ECRC), joint cooperation between the Charité Medical Faculty and the Max-Delbrück-Center for Molecular Medicine in the Helmholtz Association, Berlin, Germany
Synopsis
Ultrahigh field (UHF) MR employs higher radio frequencies (RF) than conventional MR and has unique potential to provide focal temperature manipulation and high resolution imaging (ThermalMR), as our simulations and experimental work demonstrated for f=300MHz. Here we use EMF simulations to demonstrate the added value for multi-frequency thermal intervention (f=300MHz-500MHz) to boost the efficacy of the heating paradigm for clinical target volumes (TVs) of two brain tumor patients. An optimization algorithm was developed to study RF power deposition in the TV for a single, double or triple frequency set permitting highest RF power deposition in the TV.
Introduction
Hyperthermia has proven beneficial as an adjunct treatment of Glioblastoma Multiforme (GBM)1. Advances in RF based hyperthermia have evoked developments in the designs of annular2,3 or helmet shaped4 RF applicators for the treatment of brain tumors. Optimization algorithms used to confine the RF power deposition to the target volume (TV) are under constant revision5,6. Introducing RF antenna designs that support a wide frequency range up to Δf=300MHz enable the choice of frequency to be based on the shaped and size of the TV rather than initial engineering constraints7. Previous works claim that frequencies up to 1GHz increase the focusing capabilities of RF applicators3,8. Control over the resulting temperature distribution can be further increased by driving wide band antennas at a RF frequency range that includes the Larmor frequency of an MR system to enable anatomic MRI for treatment planning and MR Thermometry (MRTh) for treatment supervision and dosage control, designated as Thermal MR. Recognizing this opportunity, this work examines the efficacy of multi-frequency thermal intervention targeting the clinical target volume of two GBM patient-derived head voxel models using a 20 channel RF applicator supporting a frequency range of 270-550MHz.Methods
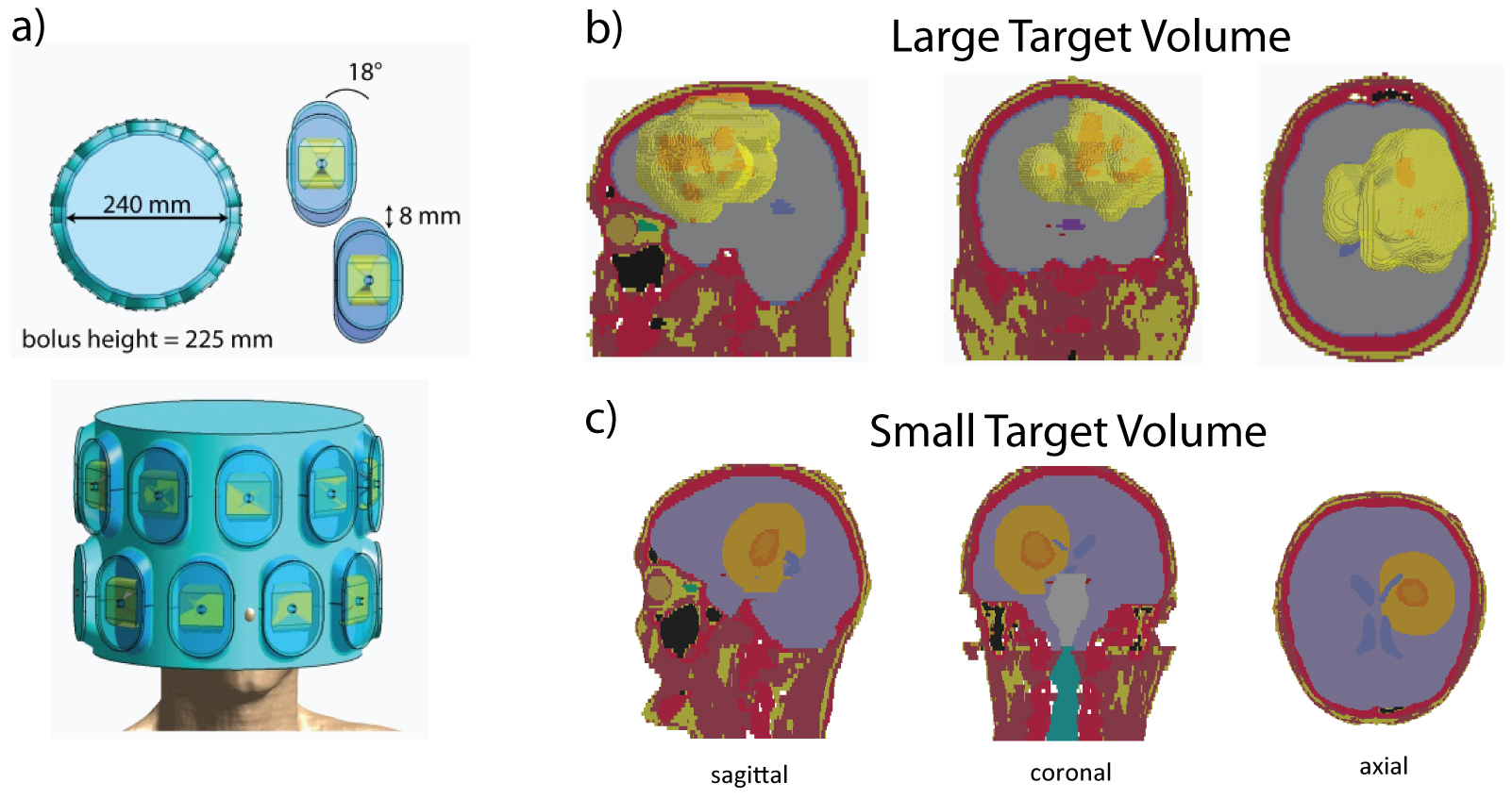
For this simulation study, two head models with TV of a) 500ml (bounding box: 10.3x10.3x9.2cm³) and b) 170ml (bounding box: 5.7x6.4x6.8cm), were placed in an annular phased array Thermal MR RF applicator. 20 self-grounded wideband bowtie antenna building blocks9 were azimuthally arranged in two rings around the head, with the center of the array being aligned with the center of the TV in z-direction (Fig.1).Broadband electromagnetic field (EMF) simulations were performed using Sim4Life10. From the channelwise E- and H-field data, SAR matrices were calculated, averaging over 10g of tissue11. For phase and amplitude optimization, a quadratically constrained quadratic program was simplified via its semidefinite relaxation12, which was solved using the MatLab13-based optimization framework YALMIP14 with different constraints. The optimization goal is set to maximize total power absorption in the TV:
maximize $$$ \sum_f tr\left(X_fQ_f\right) $$$
subject to $$$ \sum_f tr\left(X_fS_{f,i}\right) \leq SAR_{Lim} $$$ & $$$ \sum_f tr\left(X_fP_f\right) \leq P_{Lim} $$$
where tr=trace, f=frequency, Xf=frequency-specific solution matrix, Q=tumor-SAR matrix, Si=SAR-matrices in the healthy tissue and SARLim=40W/kg the exposure limit in the healthy tissue. Head power deposition was constrained via the global SAR matrix P.
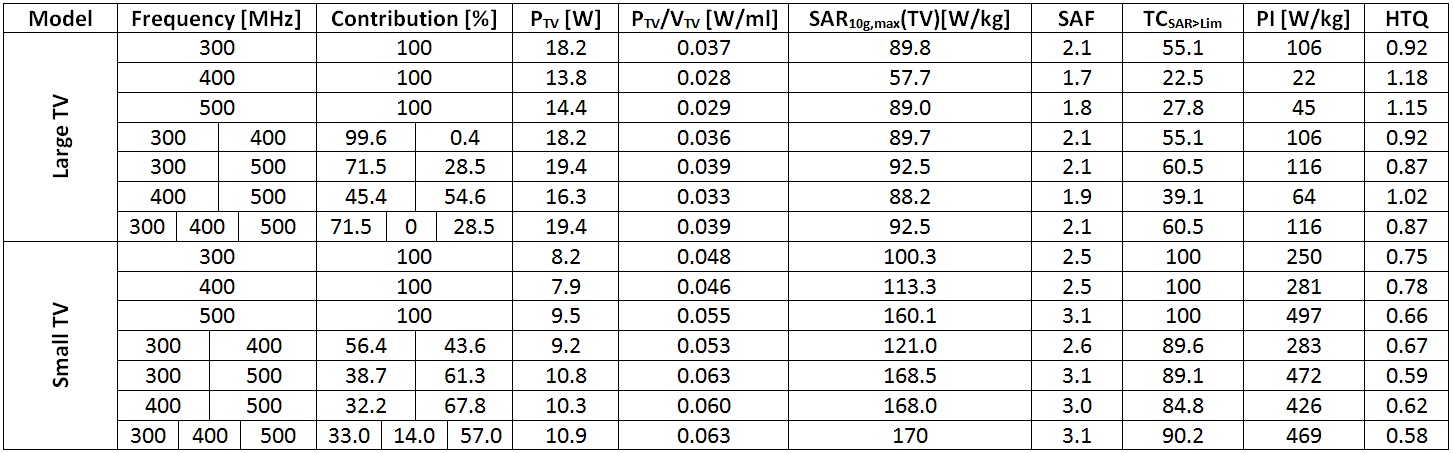
EMF simulations were performed for individual frequencies (300; 400; 500MHz). All possible combinations of frequencies were studied and benchmarked against the single frequency results. For performance assessment of the SAR10g based hyperthermia treatment planning the total RF power delivered to the TV, PTV, the performance indicator PI=SAR10g,max(TV)·SAF·TCSAR>Lim15 and the hotspot to target quotient HTQ were determined.
Results
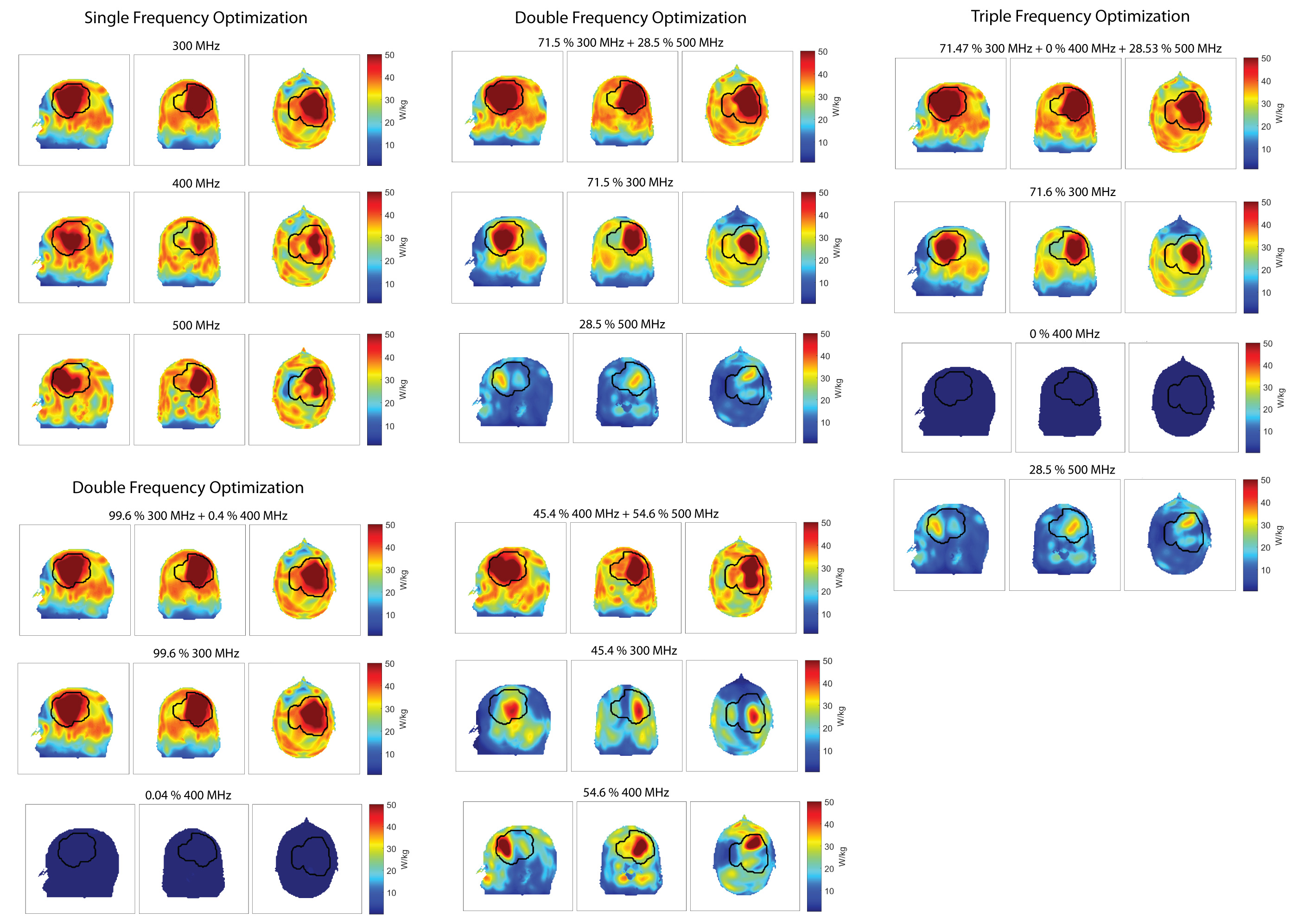
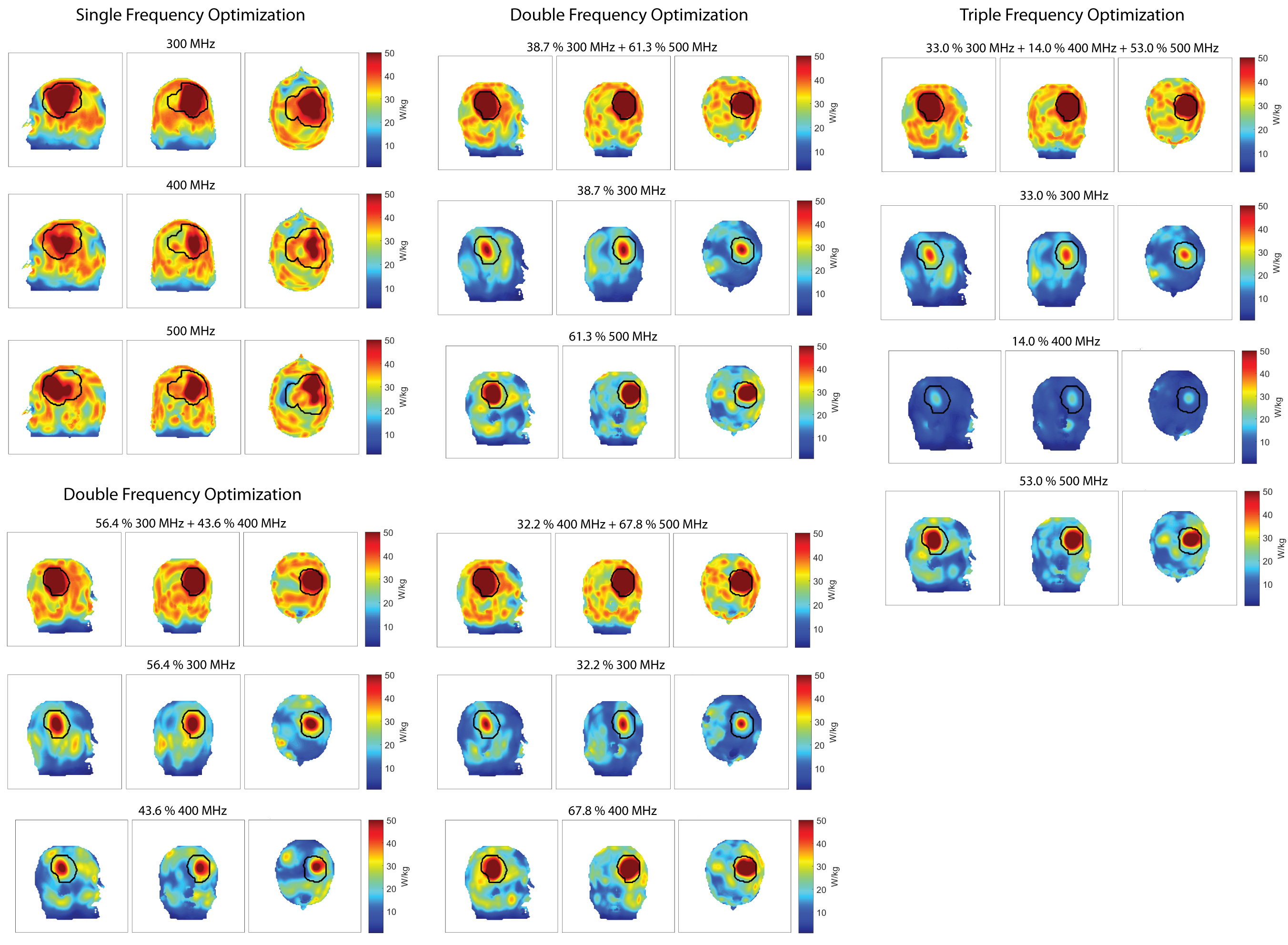
Our results demonstrate that the multi-frequency optimization algorithm was successfully implemented. For the large TV, the best single frequency result is obtained at the lowest investigated frequency (Table1, PTV(300MHz)=18.22W, PTV(400MHz)=13.75W, PTV(500MHz)=14.42W). The total target power achieved by the double frequency optimization is at least as good (Table1, PTV(300MHz) = PTV(300+400Mz)=18.22W) as the single frequencies used or better (PTV(300+500MHz)=19.38W, PTV(400+500MHz)=16.3W). The triple frequency optimization identified the most powerful combination to be a combination of 300MHz and 500MHz and sets the contribution of 400MHz to zero in the additive process (Table1). The maximum intensity projections of the additive SAR10g distributions are shown in Fig.2 for the large TV together with the double and triple frequency optimization results and the contributing SAR10g distributions of each frequency.For the small TV, the best single frequency result is obtained for the highest investigated frequency (Table1, PTV(300MHz)=8.18W, PTV(400MHz)=7.92W, PTV(500MHz)=9.49W), see Fig.4. Here, all double frequency results outperform the single frequencies used in the combination (Table1, PTV(300+400Mz)=9.2W, PTV(300+500MHz)=10.8W, PTV(400+500MHz)=10.3W). For the small target volume, the triple frequency set proved to achieve the highest total RF power deposition (PTV(300+400+500MHz)=10.9W).
Discussion and Conclusion
Our results demonstrate that multi-frequency Thermal MR holds the potential to increase the power delivered to the TV in the brain. Our optimization algorithm successfully discarded a frequency that did not boost the RF power delivery to the large TV and combined all frequencies used in this study to obtain the largest RF power delivery to the small TV. Our results also show that increasing the frequency does not necessarily result in a better target delineation if the TV exceeds the wavelength at said frequency. The high focusing at smaller wavelengths leads to insufficient coverage of the TV and thus smaller total RF power deposition. For the small TV, the highest frequency did show the best result for the single frequency optimization but was outperformed by the triple frequency optimization.To conclude, our preliminary results obtained for two patient data sets motivate inclusion of more patient data sets into our optimization algorithm to examine the correlation between the TV size and the (combination of) frequencies. In this process, we will also enhance the frequency sampling rate within the operational range of the RF applicator.
Acknowledgements
This project has received funding from the European Research Council (ERC) under the European Union's Horizon 2020 research and innovation program under grant agreement No 743077 (ThermalMR).References
1. Sneed, P.K., et al., Survival benefit of hyperthermia in a prospective randomized trial of brachytherapy boost±hyperthermia for glioblastoma multiforme. International Journal of Radiation Oncology* Biology* Physics, 1998. 40(2): p. 287-295.
2. Winter, L., et al., Design and Evaluation of a Hybrid Radiofrequency Applicator for Magnetic Resonance Imaging and RF Induced Hyperthermia: Electromagnetic Field Simulations up to 14.0 Tesla and Proof-of-Concept at 7.0 Tesla. PLoS One, 2013. 8(4): p. e61661.
3. Winter, L., et al., Thermal magnetic resonance: physics considerations and electromagnetic field simulations up to 23.5 Tesla (1GHz). Radiation Oncology, 2015. 10(1): p. 1.
4. Dobsicek Trefna, H., et al. Antenna Applicator for Microwave Hyperthermia Treatment of Pediatric Brain Cancer. in 8th European Conference on Antennas and Propagation, EuCAP 2014, The Hague, The Netherlands 6-11 April 2014. 2014.
5. Rijnen, Z., et al., Clinical integration of software tool VEDO for adaptive and quantitative application of phased array hyperthermia in the head and neck. International Journal of Hyperthermia, 2013. 29(3): p. 181-193.
6. Bellizzi, G.G., et al., Selecting the Optimal Subset of Antennas in Hyperthermia Treatment Planning. IEEE Journal of Electromagnetics, RF and Microwaves in Medicine and Biology, 2019: p. 1-1.
7. Takook, P., et al., Compact self-grounded Bow-Tie antenna design for an UWB phased-array hyperthermia applicator. International Journal of Hyperthermia, 2017. 33(4): p. 387-400.
8. Guérin, B., et al., Computation of ultimate SAR amplification factors for radiofrequency hyperthermia in non-uniform body models: impact of frequency and tumour location. International Journal of Hyperthermia, 2018. 34(1): p. 87-100.
9. Eigentler, T.W., et al., Ultra-Wideband Self-Grounded Bow-Tie Antenna Building Block for Thermal Intervention, Diagnostic MRI and MR Thermometry at 7.0 Tesla. Proceedings of the 27th ISMRM Annual Meeting and Exhibition, Montreal, Canada, 2019.
10. Sim4Life V3.4, ZMT, Zurich, Switzerland
11. IEEE, Recommended Practice for Determining the Spatial‐Peak Specific Absorption Rate (SAR) in the human body Due to Wireless Communications Devices: Measurement Techniques. 2003..
12. Luo, Z.-Q., et al., Semidefinite relaxation of quadratic optimization problems. IEEE Signal Processing Magazine, 2010. 27(3): p. 20. 13. MatLab, The MathWorks Inc., Natick, Massachusetts, US
14. Löfberg J. YALMIP : A Toolbox for Modeling and Optimization in MATLAB. In: Proceedings of the CACSD Conference. Taipei, Taiwan; 2004.
15. Oberacker, E., et al., Radiofrequency applicator concepts for RF hyperthermia treatment and MR imaging of glioblastoma multiforme at 7.0 T (298 MHz). Proceedings of the 26th Joint ISMRM-ESMRMB Annual Meeting and Exhibition, Paris, France, 2018.
Figures