4025
A Novel Ultra-Flexible High-Resolution AIR (Adaptive imaging receive) 64-Channel Bilateral Phased Array for 3T Brachial Plexus MRI
Yun-Jeong Stickle1, Clyve Follante1, Mark Giancola1, David Anderson1, Fraser Robb1, Victor Taracila1, Robert Stormont2, Holly Blahnik3, Simone Winkler4, and Darryl Sneag5
1MR Engineering, GE Healthcare Coils, Aurora, OH, United States, 2MR Engineering, GE Healthcare, Waukesha, WI, United States, 3MR Apps&WF, GE Healthcare, Waukesh, WI, United States, 4MRI Engineering, Weill Cornell Medicine, New York, NY, United States, 5Radiology and Imaging, Hospital for Special Surgery, New York, NY, United States
1MR Engineering, GE Healthcare Coils, Aurora, OH, United States, 2MR Engineering, GE Healthcare, Waukesha, WI, United States, 3MR Apps&WF, GE Healthcare, Waukesh, WI, United States, 4MRI Engineering, Weill Cornell Medicine, New York, NY, United States, 5Radiology and Imaging, Hospital for Special Surgery, New York, NY, United States
Synopsis
An ultra-flexible AIR
64-Channel bilateral phased array coil is described for acquiring
high-sensitivity images of the brachial plexus by wrapping coil elements snugly
around the cervical, shoulder, axillary, and arm regions. This coil comprises a foam posterior and flexible flaps
with a low loss malleable conductor optimized for zero reactance. An
exceptionally low noise preamplifier is tolerant of a wide range of loading. This
coil facilitates imaging large fields of view bilateral brachial plexi, as well
as higher resolution unilateral imaging for detailed evaluation of nerve
fascicular architecture and other pathology, thereby optimizing
setup time and patient comfort.
Introduction
As most peripheral nerves in the human body are < 1 cm in diameter, and many < 1mm, spatial resolution is critical for reliable evaluation. Typically, a rigid neurovascular array or the combination of two flexible coils for the brachial plexus are used (Fig. 1 (a) and (b)). These coils do not generally provide deep depth or high-resolution due to the large distance between coil elements and nerves of interest. High acceleration factors are also not practical due to the low SNR and number of elements in the FOV (field of view). Coil positioning can also be challenging. In this paper, a novel, ultra-flexible high-resolution AIR 64-channel bilateral phased-array coil for BP MRI is presented. A prototype of the flexible 64-channel bilateral phased-array coil was constructed on foam and flexible fabric materials (fitting more than 95th - percentile US male) with AIR technology. The prototype coil was evaluated on phantoms as well as symptomatic and asymptomatic human volunteers under an IRB-approved protocol.Methods
A range of body habiti were evaluated to ensure the coil provided the flexibility to accommodate body sizes spanning the 5th percentile US female to the 95th percentile US male. A novel ultra-flexible high-resolution 64-channel bilateral phased-array coil was developed using AIR coil loops [3, 4], foam and flexible materials. The AIR coil loops are made from highly flexible 1.0 mm conductor optimized for zero reactance and low loss with no lumped components at 127.73 MHz. The electronics module including the preamplifier, decoupler, matching, and baluns is connected to the new AIR coil loop. Nearest neighboring elements were decoupled by overlapping and next nearest neighbor and more distant elements were decoupled by preamplifiers which is exceptionally low noise and is tolerant of a wide range of loop loading conditions. Full coverage of the brachial plexus and its branches area was achieved by 64 elements located in a posterior base with flexible neck, shoulder and body flaps (Left and Right-side). The flexible materials and AIR Coil loops provide a light weight flexible conforming coverage (Fig. 2). This coil shall support 1D acceleration factor of 3 (R=3) with ASSET and Multi-Band acceleration factor of 3 (SI) in FOV 30 cm. This coil provides deeper depth, higher resolution and highly accelerated images due to higher channel counts and the proximity to the patient body. AIR loops are between two thermoplastic coated thin fabrics (1mm). A medical grade foil was used as the coil cover sleeve for biocompatibility and a water seal. The SNR and max g-factors for R=2, 3, 4 were measured in phantoms. The coil was developed and tested on a 144-channel 3T GE Premier scanner (Signa Premier, GE Healthcare, Aurora, Ohio USA). A total of 22 volunteers were imaged at the Hospital for Special Surgery (New York, USA).Results
Brachial plexus MRI is inherently challenging due to anatomic coverage and high spatial resolution requirements. The unloaded phantom images were acquired with a SE sequence and all elements were well decoupled. This 64-channel “bilateral” prototype coil provided a large imaging volume for the brachial plexus and its branches while still supporting high spatial resolution. Coronal maximum intensity projections (MIPs) from 3-D short tau inversion recovery (STIR) pulse sequences with this prototype coil were used to obtain imaging of the bilateral plexus (40 cm FOV, Fig. 3 (a)) as well as the unilateral right plexus (22 cm FOV, Fig. 3 (b) ) with high spatial resolution. The image in Fig. 4 (a) was acquired with an oblique sagittal T2-weighted Dixon fat suppressed sequence, with a 16 cm FOV. This shows clear demonstration of the extraforaminal C5-T1 roots. The image in Fig. 4 (b) shows the curved multiplanar reformatted image of the right brachial plexus from a 3-D short tau inversion recovery (STIR) pulse sequence following intravenous gadolinium demonstrates clear depiction of the supra- and infra-clavicular portions of the plexus, with complete vascular suppression. Figure 5 shows the maximum g-factor results at R= 2, 3 and 4 for the novel flexible coil for 1D acceleration in the axial. Table 1 summarizes the maximum g-factor at 2, 3 and 4 for 1D acceleration in the axial, sagittal and coronal planes. The benefits of increased channel number for reducing g-factor were evident.Discussion
The loading shell phantom results for B1 sensitivity mapping and g-factors are matched to the results of the in vivo images.Conclusions
This novel 64-channel bilateral array that accommodate the 5th percentile female up to the 95th percentile male provides ultra-flexibility, comfort, and high-resolution imaging with AIR technology including highly flexible conductor, miniaturized electronics, exceptionally low noise preamp, and light-weight mechanical materials. The brachial plexus and its branches are able to be visualized on large field of view coronal images and low g-factors can also be obtained in all 3 (axial, sagittal and coronal) planes. This prototype coil provides high spatial resolution with improved patient comfort and reduced coil setup time.Acknowledgements
We thank Saban Kurucay, Dan Weyers, Dan Chirayath and Mohamed El-Demerdash from GE Healthcare for their continued support.References
- Sneag DB., et al., High-resolution Brachial Plexus Imaging using 3-D Short Tau Inversion Recovery (CUBESTIR) with IV Gadolinium for Vascular Suppression. Proceedings ISMRM 2019.
- Chhabra A., et al., High-resolution 3T MR neurography of the brachial plexus and its branches, with emphasis on 3D imaging. AJNR Am J Neuroradiology 2013 Mar;34:486-97.
- Rossman P., et al., Characterization of a new ultra-flexible low-profile RF receive coil technology. Proceedings ISMRM 2017, 763.
- Vasanawala S.S., et al., Development and Clinical implementation of very light weight and highly flexible Air technology arrays. Proceedings ISMRM 2017, 755.
- Roemer P.B., et al., The NMR phased array. MRM, 1990; 16(2):192-225.
- Pruessmann K.P., et al., SENSE: sensitivity encoding for fast MRI. MRM, 1999;42:952–962.
Figures
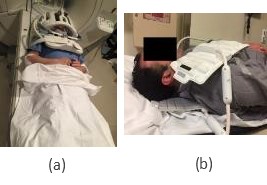
Fig. 1. Traditional brachial plexus coil setup options: (a) Combined
head/neurovascular array and (b) Two 16 channel flexible coils
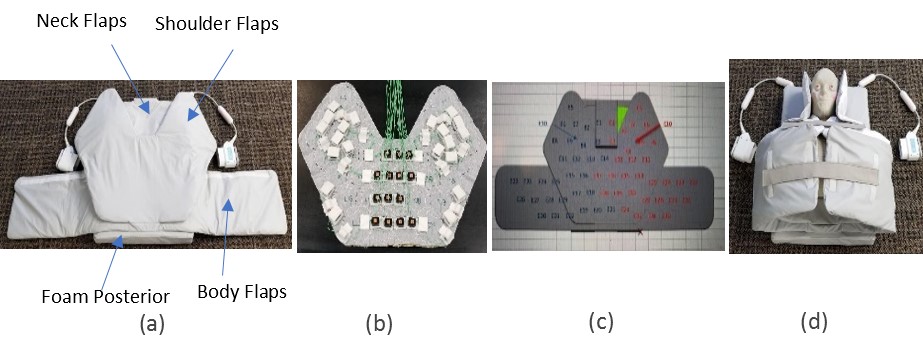
Fig. 2. Completed ultra-flexible AIR 64-channel
bilateral phased array for Brachial Plexus MRI (a) Mechanical assembly (b) Coil assembly (c) 64-Channel layout (d) Wrapped around a 95th
percentile phantom

Fig. 3. Coronal maximum intensity
projections (MIPs) from T2-weighted 3-D short tau inversion recovery (STIR)
pulse sequences of the (a) Bilateral plexus (40 cm FOV) and (b) Unilateral right plexus (22 cm FOV)

Fig. 4. (a) Oblique sagittal T2-weighted
Dixon fat suppressed image (16 cm FOV) demonstrates the extraforaminal C5-T1
roots. (b) Curved multiplanar reformatted image of the right brachial plexus
from a 3-D short tau inversion recovery (STIR) pulse sequence with vascular
suppression demonstrates multiple intrinsic constrictions of the suprascapular
nerve (blue bracket) in this patient with Parsonage-Turner syndrome.
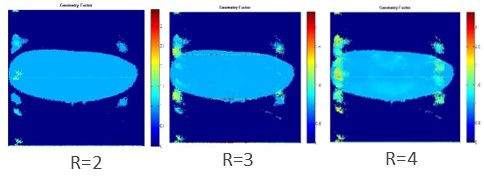
Fig. 5.
Maximum g-factor maps at R=2, 3 & 4, Axial: Ultra-flexible high-resolution AIR 64-channel bilateral
phased array coil

Table1. Maximum
g-factors at R=2,3 &4, Axial, Sagittal and Coronal planes