3964
A machine learning investigation of resting-state fMRI abnormalities in HIV-associated neurocognitive disorder1GuangXi Medical University Cancer Hospital, Nanning, China, 2MR Research, GE Healthcare, Beijin, China
Synopsis
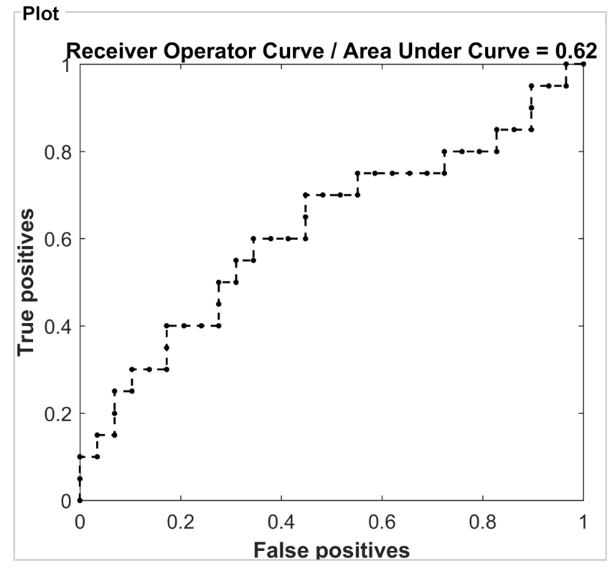
Frascati criteria for diagnosis of HIV-associated neurocognitive disorder lacks sensitivity, specificity, susceptible to learning effect, socioeconomic position and other confounding factors. fMRI can sensitively discover pathophysiological changes in HIV-infected central nervous system. In our study, ALFF and fALFF separately well classified HIV-positive and HIV-negative groups with AUC = 0.65 and 0.62, respectively. Our findings of injured frontal,parietal and occipital cortex associated with execution and attention function were consistent with previous studies, indicating activations reduced in the frontal lobe but increased in occipital lobe among patients with HAND. Both ALFF and fALFF could be biomarkers for objectively classifying HIV individuals.
Introduction
Diagnosis of HIV-associated neurocognitive disorder has relied on Frascati criteria in the neuropsychometric tests; however, it lacks sensitivity, specificity, susceptible to learning effect, socioeconomic position and other confounding factors. 1 It may be difficult to positively confirm psychiatric symptoms ahead of occurrences. 2 fMRI can sensitively discover pathophysiological changes in HIV-infected central nervous system. 3 For example, injured frontal lobe causes impairments of voluntary movements, speech and spirits; damaged angular gyrus causes dyslexia; injured precuneus induced impairments of self-awareness, episode memory and visual spatial processing and reflection; injured temporal lobe and occipital lobe lead to impairments of audition and speech. Thus, this study aims to explore the role of low-frequency amplitude in neurocognitive impairments in patients with HIV using resting-state MRI (rs-MRI) using a machine learning approach. Resting state images were post-processed with DPABI to obtain Amplitude of Low Frequency Fluctuation (ALFF) and fractional Amplitude of Low Frequency Fluctuation(fALFF) values.Materials and Methods
29 HIV-positive patients without anti-virus therapy and 14 normal subjects were enrolled in our study. Additionally, the HIV group was further divided into HAND (HIV-associated neurocognitive disorder) and non-HAND subgroups based on neuro-psychometric tests as reference criteria. All patients gave the informed consent form to receive MR imaging. Routine axial T1WI, axial T2WI, sagittal T1WI and gradient echo-echo planar image were performed on 3.0T clinic scanner (GE Discovery MR 750w). Resting state images were post-processed with DPABI to obtain Amplitude of Low Frequency Fluctuation (ALFF) and fractional Amplitude of Low Frequency Fluctuation(fALFF) values. Then, the PRoNTo toolbox and SPSS 20.0 were applied for classification of HIV patients and determination of HAND related brain regions.Results and Discussion
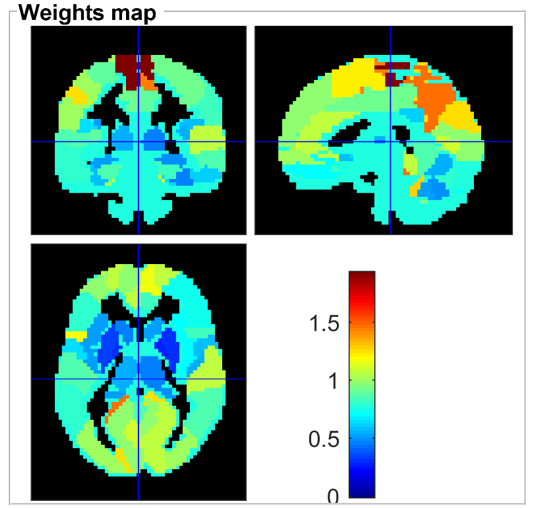
ALFF and fALFF separately well classified HIV-positive and HIV-negative groups with AUC = 0.65 and 0.62, respectively (Figure 1). The top 10 discriminative brain regions were demonstrated in Table 1and Figure 2. All those aberrant brain regions detected in HIV-positive group showed the consistent results with previous studies. 2,3 ALFF values in right paracentral lobule and section 1, 2 and 10 of cerebellar vermis showed significant differences between the two HIV subgroups (p < 0.05). A study4has shown that activations reduced in the frontal lobe but increased in occipital lobe among patients with HAND, compared to patients without HAND and healthy subjects. Moreover, patients with HAND had declined functions of execution memory, and motor while they still retained speed of information processing, attention, working memory and verbal fluency. Our findings of injured frontal,parietal and occipital cortex associated with execution and attention function were consistent with these aforementioned.Conclusions:
Our results demonstrated that both ALFF and fALFF could comprehensively and objectively classify HIV individuals. Moreover, the neuroimaging biomarker for identification of HAND were also reported.Acknowledgements
No acknowledgement found.References
- Antinori A, Areodt G,Becker JT,et a1.Updated research nosology for HIV-associated neurocognitive disorders[J]. Neurology, 2007, 69(18):1789-1799.
- Chockanathan U , Dsouza A M , Abidin A Z , et al. Automated diagnosis of HIV-associated neurocognitive disorders using large-scale Granger causality analysis of resting-state functional MRI[J]. Computers in biology and medicine, 2019, 106:24-30.
- Yue L, Chang-Bin J, YIN-Jian, et al. CT and MRI study of vascular cognitive impairment[J]. Journal of Dalian Medical University, 2011,33(1):82-85.
- Ma X, Li S, Tian J, et al. Altered brain spontaneous activity and connectivity network in irritable bowel syndrome patients: A resting-state fMRI study[J]. Clinical Neurophysiology, 2015, 126(6):1190-1197.
Figures