3841
Cross vendor harmonization of water-extraction-phase-contrast-arterial-spin-tagging (WEPCAST) MRI for blood brain barrier assessment1Department of Radiology, Johns Hopkins University, Baltimore, MD, United States, 2Department of Radiology, New York University Langone Medical Center, New York, NY, United States
Synopsis
Water-extraction-with-phase-contrast-arterial-spin-tagging (WEPCAST) MRI was proposed recently as a non-invasive technique to assess blood-brain barrier (BBB) permeability to water. However, the reproducibility of this technique and cross-vendor reliability has not been reported. In this study, we harmonized WEPCAST technique across two major MRI vendors, Philips and Siemens and examined the test-retest reproducibility of the technique. The results showed that WEPCAST MRI can give a reliable assessment of BBB permeability with an excellent reproducibility.
INTRODUCTION
Water-extraction-with-phase-contrast-arterial-spin-tagging (WEPCAST) MRI was recently proposed for non-contrast assessment of blood-brain barrier (BBB) permeability to water1. By labeling water spins at the arterial side and evaluating non-exchanged spins at the venous side, the technique provides a measurement of water extraction fraction (E) and BBB permeability-surface-area-product (PS). Although WEPCAST MRI has been compared with Gd-based measurement2 and was also shown to be sensitive to several diseases, e.g. Alzheimer’s disease and Sickle Cell Anemia3,4, a systematic test-retest study of the technique has not been performed. Furthermore, the reliability of the technique across MRI vendors, the importance of which is increasingly recognized in this era of big-data, has not been evaluated. Therefore, in this study, we sought to harmonize the WEPCAST sequence between two major vendors, and examine the intra-session, inter-session, and inter-vendor test-retest reproducibility of this technique.METHODS
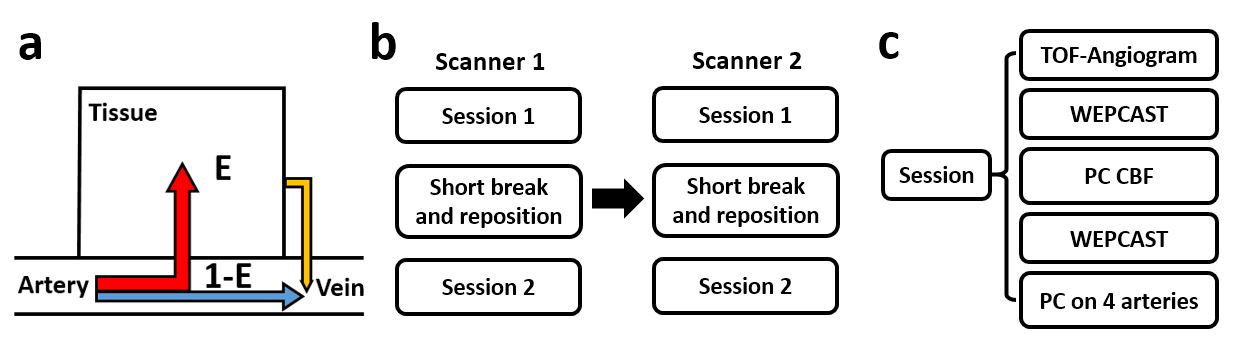
Pulse SequenceThe basic principle of WEPCAST MRI (Figure 1a) is to assess water extraction by measuring the arterially labeled spins in large draining veins, e.g. superior sagittal sinus (SSS). To separate venous blood from surrounding tissue, a phase-contrast gradient pair was applied in acquisition. WEPCAST signal can be written as: $$ΔM=2\alpha(1-E)e^{-\delta/T_{1b}}, [1]$$where E is extraction fraction of water, α is labeling efficiency (86%, assumed5), δ is BAT of SSS and T1b is blood-T1 (1.8s, assumed6). Thus the only unknowns here are δ and E. We took advantage of the fact that we measured WEPCAST signal along the entire length of the SSS, from which we can obtain signal profile. Then the peak signal should appear at the center of the labeling bolus, the BAT of which is 0.5*labeling-duration+post-labeling-delay(PLD). E can then be estimated using Eq.[1]. Together with cerebral blood flow (CBF), BBB permeability to water can then be calculated as: $$PS=-ln(1-E)·CBF, [2]$$
To evaluate WEPCAST technique across vendors, the sequence was implemented on two 3T platforms, a Philips Ingenia system and a Siemens Prisma system. The labeling module (in terms of B1 and gradient strength) and background-suppression pulses were carefully matched. Identical imaging parameters were used on both scanners: TE=13ms, TR=7200ms, labeling duration=2000ms, PLD=3500ms, velocity-encoding=15cm/s, 10 averages, scan duration=4min55s.
MRI Experiment
Ten healthy volunteers (24.6±2.3yrs, 5F/5M) were studied. Each participant was scanned on both systems within 2 hours. The order of Philips and Siemens scanner was counterbalanced across subjects. On each scanner, the subject went through two sessions (Figure 1b), with a short break and reposition between sessions. Before session 1, a T1-MPRAGE was acquired. Then in each session, WEPCAST and Phase-contrast CBF were performed twice (Figure 1c).
Data Analysis
WEPCAST data was processed following previous procedures1. Briefly, WEPCAST difference images were generated by subtracting complex-difference images in control and label conditions. Mask for the SSS was drawn manually and the resulting signal was used to quantify E. Phase-contrast MRI was analyzed as previously to generate CBF7. Together, PS was calculated as Eq.[2].
Test-retest reproducibility was evaluated by Coefficient of variation (CoV), ANOVA test, paired t-test, and Bland-Altman plot. Inter-rater reliability was also evaluated by having two raters independently analyze the same datasets.
RESULTS AND DISCUSSION
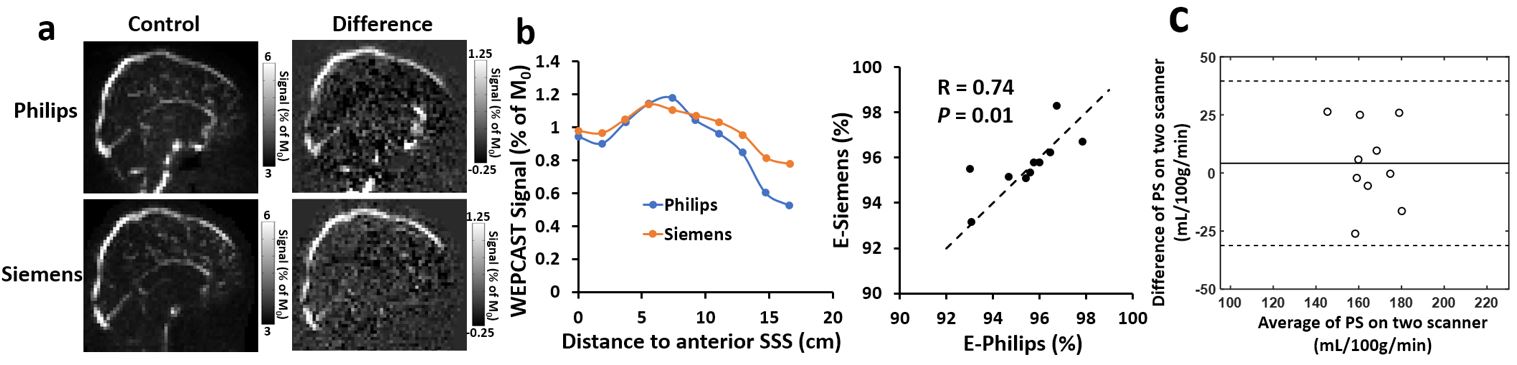
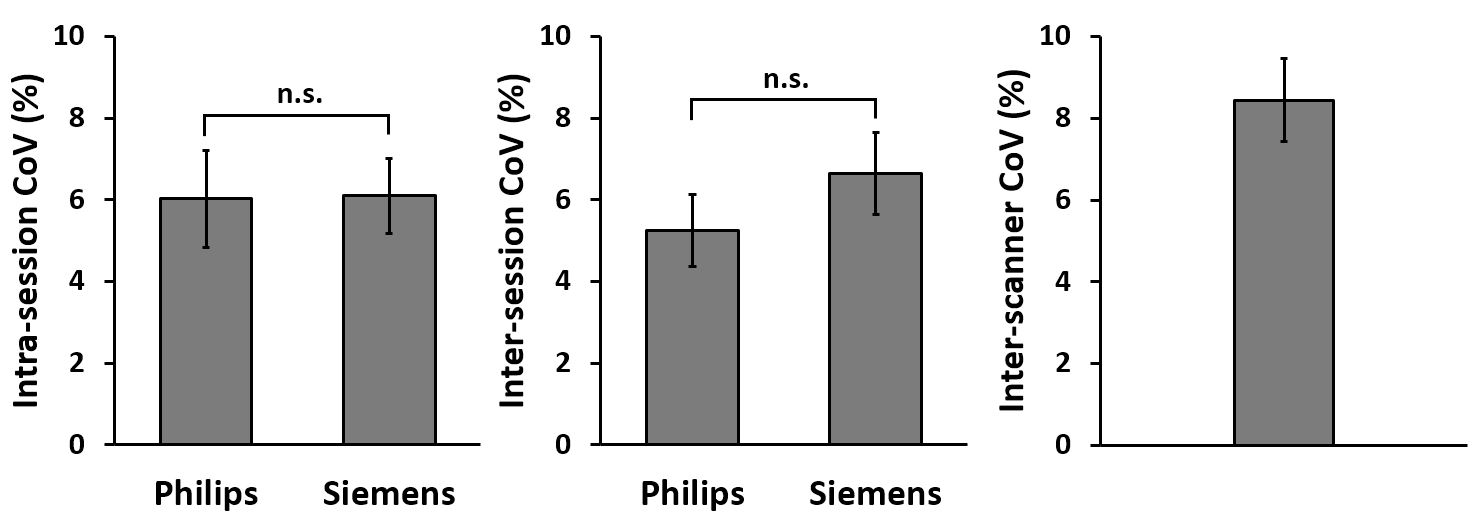
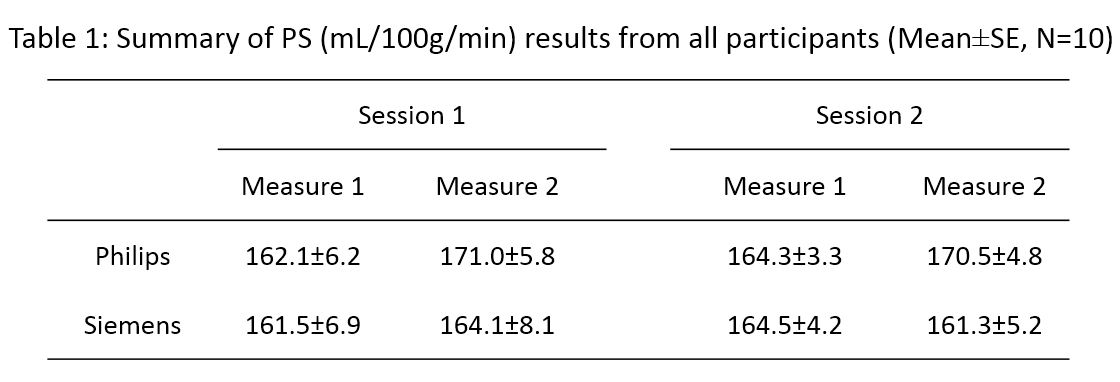
Figure 2a showed representative WEPCAST images of one participant from two scanners. The WEPCAST signals were used to derive E (Eq. [1]). Scatter plot of E between two scanners showed a good correlation (Figure 2b, p=0.01) and paired t-test showed no significant difference (p=0.47). PS was then calculated for all measurements, and the results were summarized in Table 1. ANOVA tests revealed no difference in PS between repetitions, sessions, or scanners (p=0.27, 0.92 and 0.45). Bland-Altman plot of PS from two scanners also demonstrated a good agreement between two platforms (Figure 2c). An interrater reliability was also examined and showed good consistency of PS obtained from two raters (R=0.93).Figure 3 displayed the intrasession and intersession CoV for PS measurement from each scanner and also interscanner CoV. It can be seen that the intrasession and intersession CoV on both scanners were around 6%. No significant difference was found between CoV calculated from two scanners (p=0.96 for intrasession and p=0.39 for intersession). Compared with arterial-spin-labeling (ASL) technique, which was reported to have a CoV of around 10%8-10, our results suggested that the WEPCAST technique has a good test-retest reproducibility.
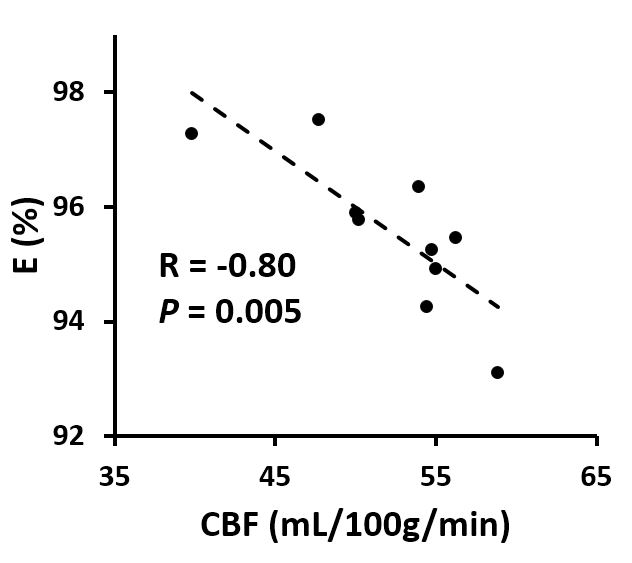
We also examined intersubject variations in WEPCAST MRI and found a CoV of 6.6% in PS values. However, it is interesting to note that the intersubject CoV of CBF and WEPCAST signal intensity were 9.6% and 26.9%, which were much higher than the variation of PS. We further explored this phenomenon by examining the relationship between CBF and E. It was found that individuals with a higher CBF tended to have a lower E (Figure 4, p=0.005), suggesting that BBB permeability is less variable across subjects compared to CBF or water extraction fraction.
CONCLUSION
In this study, we harmonized the WEPCAST MRI technique across two major MRI vendors and examined its test-retest reproducibility. The results demonstrated a good consistency of PS estimation between two platforms and also an excellent reproducibility for both intrasession and intersession measurements. These findings suggested that WEPCAST MRI can give a reliable assessment of BBB permeability and may be useful in diseases with BBB breakdown.Acknowledgements
No acknowledgement found.References
1. Lin Z, Li Y, Su P, Mao D, Wei Z, Pillai JJ, Moghekar A, van Osch M, Ge Y, Lu H. Non-contrast MR imaging of blood-brain barrier permeability to water. Magn Reson Med 2018;80:1507-1520.
2. Lin Z, Uh J, Li Y, Jiang D, Lu H. Non-contrast assessment of BBB permeability using WEPCAST MRI: validation with contrast-agent based method. 2019. Proceedings of the 27th Annual Meeting of ISMRM, Montreal, Canada. p 0539.
3. Lin Z, Lance E, Li Y, Su P, Liu P, Cannon A, Casella JF, Lu H. Impaired blood-brain barrier function in pediatric sickle cell disease. 2019. Proceedings of the 27th Annual Meeting of ISMRM, Montreal, Canada. p 0738.
4. Lin Z, Sur S, Liu P et al. Imaging disruption of blood-brain-barrier (BBB) in Mild Cognitive Impairment without using contrast agent. 2018. Proceedings of the 26th Annual Meeting of ISMRM, Paris, France. p 0724.
5. Alsop DC, Detre JA, Golay X et al. Recommended implementation of arterial spin-labeled perfusion MRI for clinical applications: A consensus of the ISMRM perfusion study group and the European consortium for ASL in dementia. Magn Reson Med 2015;73:102-116.
6. Li W, Liu P, Lu H, Strouse JJ, van Zijl PCM, Qin Q. Fast measurement of blood T1 in the human carotid artery at 3T: Accuracy, precision, and reproducibility. Magn Reson Med 2017;77:2296-2302.
7. Peng SL, Su P, Wang FN, Cao Y, Zhang R, Lu H, Liu P. Optimization of phase-contrast MRI for the quantification of whole-brain cerebral blood flow. J Magn Reson Imaging 2015;42:1126-1133.
8. Mutsaerts HJ, Steketee RM, Heijtel DF, Kuijer JP, van Osch MJ, Majoie CB, Smits M, Nederveen AJ. Inter-vendor reproducibility of pseudo-continuous arterial spin labeling at 3 Tesla. PLoS One 2014;9:e104108.
9. Chen Y, Wang DJ, Detre JA. Test-retest reliability of arterial spin labeling with common labeling strategies. J Magn Reson Imaging 2011;33:940-949.
10. Petersen ET, Mouridsen K, Golay X, all named co-authors of the Qt-rs. The QUASAR reproducibility study, Part II: Results from a multi-center Arterial Spin Labeling test-retest study. Neuroimage 2010;49:104-113.
Figures