3817
Whole-Brain Functional MRI in Human Subjects Wearing Metallic Orthodontic Braces1Neurosection, Division of MRI Research, Russell H. Morgan Department of Radiology and Radiological Science, Johns Hopkins University School of Medicine, Baltimore, MD, United States, 2F.M. Kirby Research Center for Functional Brain Imaging, Kennedy Krieger Institute, Baltimore, MD, United States, 3Department of Medical Imaging, Nanfang Hospital, Southern Medical University, Guangzhou, China, 4Johns Hopkins University School of Medicine, Division of Neuroradiology, Russell H. Morgan Department of Radiology and Radiological Science, Baltimore, MD, United States, 5Department of Neurosurgery, Johns Hopkins University School of Medicine, Baltimore, MD, United States
Synopsis
Metallic objects such as dental braces bring substantial susceptibility artifacts in MR images acquired using echo-planar-imaging (EPI) sequences. Gradient-echo EPI is currently the most commonly adopted sequence for blood oxygenation level–dependent (BOLD) functional MRI (fMRI) in humans, which suffers from susceptibility artifacts including signal dropout and geometric distortion in the presence of metallic implants. Here, we demonstrate that T2-prepared (T2prep) BOLD fMRI can significantly reduce susceptibility artifacts that are commonly seen in GRE EPI in the presence of metallic orthodontic braces.
Introduction
MR images acquired using echo-planar-imaging (EPI) sequences are sensitive to susceptibility artifacts such as signal dropout and geometric distortion in regions affected by large susceptibility effects. Dental fillings and orthodontic braces containing various metals can cause such artifacts extending from the facial region into the brain in EPI1,2,3. This is particularly a problem for functional MRI (fMRI) studies as gradient-echo EPI is currently the most commonly adopted sequence for blood oxygenation level–dependent (BOLD) fMRI in humans. A whole-brain T2-prepared BOLD fMRI approach4 was recently demonstrated, which uses a T2-preparation module to induce the BOLD contrast, immediately followed by a 3D fast GRE readout with short echo time (< 2 msec). T2-prepared BOLD showed little susceptibility artifacts throughout the brain, and greater functional sensitivity than GRE EPI BOLD in regions near air-filled cavities in healthy participants4, and around the lesions containing blood products in presurgical MRI patients5,6. In this study, we apply T2-prepared (T2prep) BOLD fMRI4 in healthy human subjects wearing metallic orthodontic braces to evaluate its ability to minimize susceptibility artifacts in the presence of metallic objects7.Methods
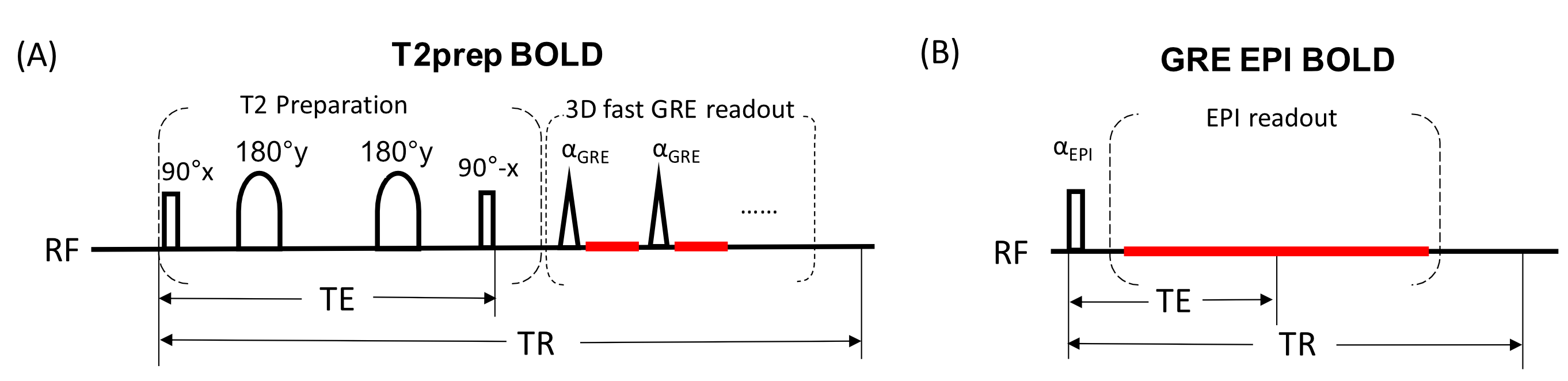
Six healthy participants (40±6yo, 3 females) were scanned. Removable dental braces with bonding trays were used so that MRI images can be acquired with and without braces in the same participants. Figure 1 illustrates the T2-prepared BOLD fMRI sequence, which consists of a double refocusing T2-preparation module for generating the BOLD contrast, followed by a 3D fast GRE readout. The following scans were acquired for each subject on a 3T Philips MRI scanner: 1) MPRAGE (voxel=1x1x1mm3); 2) GRE-EPI-BOLD-fMRI (TR/TE=2000/30ms, flip angle (FA)=90°, voxel=3.75×3.75×4 mm3, 40 slices, single-shot EPI, SENSE=3, fat suppression); and 3) T2prep-BOLD-fMRI (TR/TE=2000/50ms, FA=20°, voxel=3.75×3.75×4 mm3, 40 slices, single-shot 3D fast GRE, SENSE factor=2×1.5, centric phase encoding profile, TRGRE/TEGRE=3.2/1.34ms). The order of fMRI scans was pseudo-randomized. To assess BOLD fMRI signal changes in the entire brain, a breath-hold task8 was performed, which consists of 4 blocks of 40-second normal breathing, 4-second inhalation (5), and 16-second breath-holding, with an additional 20-second normal breathing period after the last block (total duration=4min20sec). fMRI data was analyzed using SPM12 and Matlab. Preprocessing steps include motion correction, slice timing correction (for 2D multi-slice EPI BOLD scans only, not needed for 3D T2prep BOLD scans), co-registration between fMRI and anatomical images, segmentation, and normalization. A general linear model (GLM) was employed to detect functional activation (adjusted P<0.05, cluster size≥3). fMRI results from the EPI and T2prep fMRI methods were compared using an region-of-interest (ROI) based analysis. Two ROIs were manually delineated in each subject: one with strong susceptibility artifacts (dropout), and one covering bilateral motor cortex with minimal susceptibility artifacts in EPI. To calculate the relative signal change (∆S/S) between breath-hold and normal breathing, the BOLD time course from each scan was first averaged across the 4 blocks, and the peak-to-trough difference described in the literature with similar breath-hold paradigms was taken as the signal change 9. Temporal signal-to-noise ratio (tSNR) was calculated as the signal divided by standard deviation along the time course in each voxel. Contrast-to-noise ratio (CNR) was defined as the product of tSNR and ∆S/S.Results
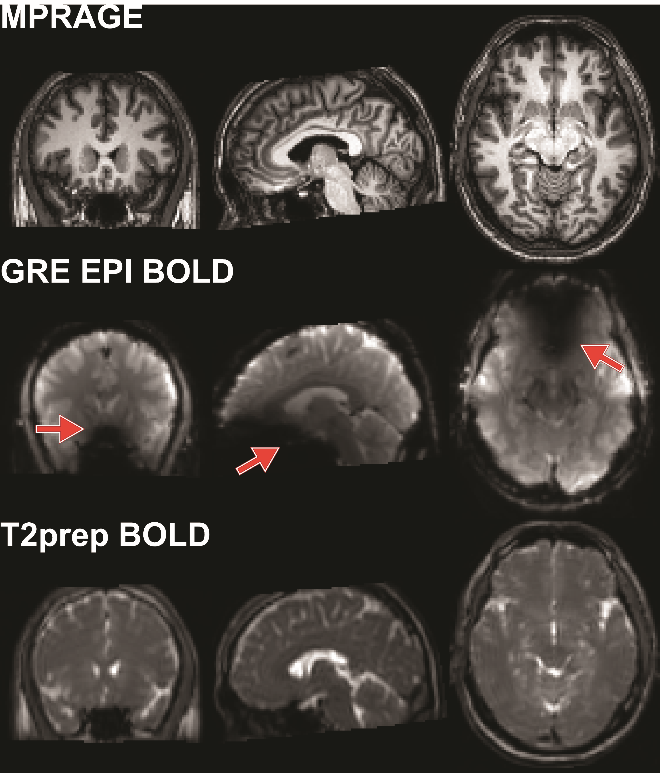
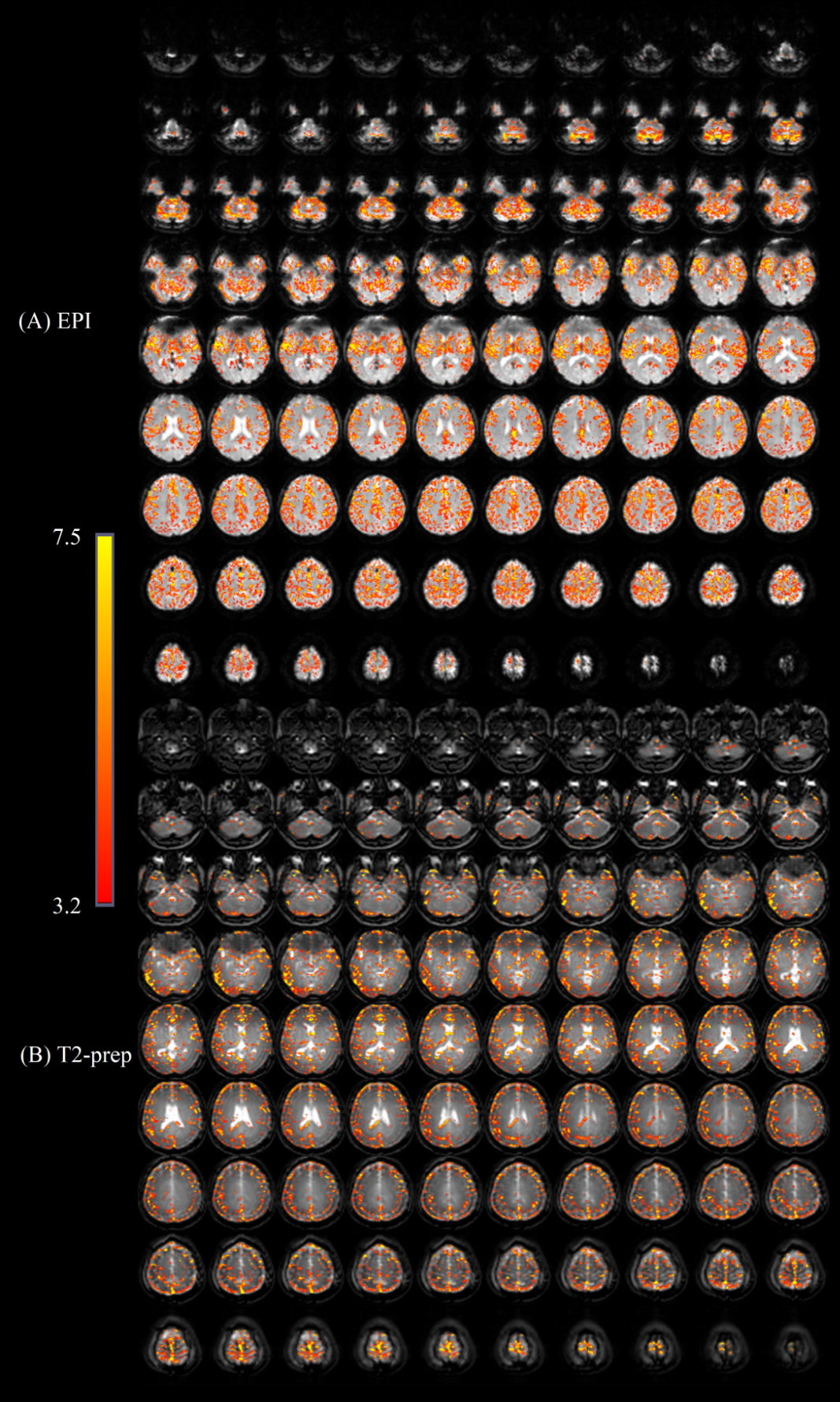
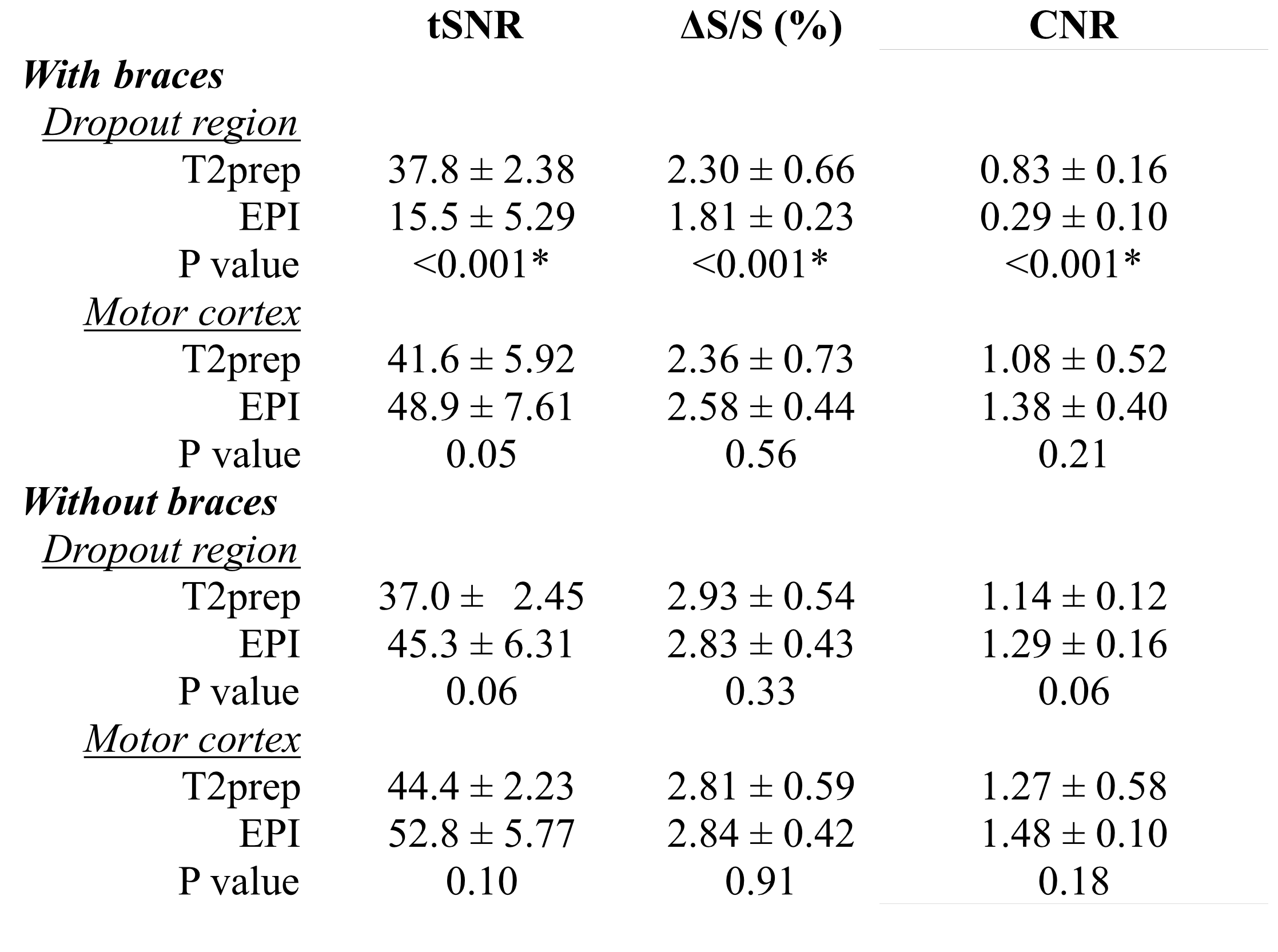
Figure 2 demonstrates the representative image quality of the fMRI scans from one subject wearing metallic braces. While little visible artifact in the brain can be observed on the anatomical (MPRAGE) images, large signal voids can be seen on the GRE EPI BOLD fMRI images, which include mainly the orbitofrontal and ventromedial prefrontal cortex (referred to as the “dropout region” in subsequent text). Similar to MPRAGE images, little visible artifact can be observed on T2prep BOLD fMRI images in the entire brain. Typical activation maps during breath-hold are shown in Figure 3. While activation was detected in most regions with minimal susceptibility artifacts using both methods, less activations were detected in the dropout region with GRE EPI BOLD than with T2-prepared BOLD. The group-averaged quantitative results from all participants are summarized in Table 1. As expected, tSNR, ΔS/S, and CNR in the dropout region were all significantly higher in T2prep BOLD than in EPI images. On the other hand, in the motor cortex where the susceptibility artifacts are expected to be minimal, GRE EPI BOLD showed a trend (not significant) of higher tSNR, ΔS/S and CNR compared to T2prep BOLD. In the same subjects when not wearing braces, tSNR, ΔS/S and CNR in the dropout region were comparable (P>0.1) in T2prep scans, but were significantly improved (P<0.001) in EPI scans compared to corresponding results with braces. The results in the motor cortex were comparable (P>0.1) with and without braces.Discussion & Conclusion
We demonstrate that T2prep-BOLD-fMRI can acquire BOLD images in healthy human subjects wearing metallic dental braces with preserved CNR in the entire brain, whereas conventional EPI approaches showed significantly reduced CNR in regions with strong susceptibility effects. T2prep-BOLD-fMRI is expected to provide an alternative approach in studies suffering from large susceptibility artifacts, for instance in the presence of metallic implants in the brain, or for adolescents wearing braces.Acknowledgements
NINDS (1R01NS108452), NIBIB (R21EB 023538 and P41 EB015909), NICHD (U54 HD079123).References
1. Starčuková J, Starčuk Z, Hubálková H, Linetskiy I. Magnetic susceptibility and electrical conductivity of metallic dental materials and their impact on MR imaging artifacts. Dent Mater. 2008;24(6):715-723. doi:10.1016/J.DENTAL.2007.07.002
2. New PF, Rosen BR, Brady TJ, et al. Potential hazards and artifacts of ferromagnetic and nonferromagnetic surgical and dental materials and devices in nuclear magnetic resonance imaging. Radiology. 1983;147(1):139-148. doi:10.1148/radiology.147.1.6828719
3. Hinshaw DB, Holshouser BA, Engstrom HI, Tjan AH, Christiansen EL, Catelli WF. Dental material artifacts on MR images. Radiology. 1988;166(3):777-779. doi:10.1148/radiology.166.3.3340777
4. Hua J, Qin Q, Van Zijl PCM, Pekar JJ, Jones CK. Whole-brain three-dimensional T2-weighted BOLD functional magnetic resonance imaging at 7 Tesla. Magn Reson Med. 2014;72(6):1530-1540. doi:10.1002/mrm.25055
5. Hua J, Miao X, Agarwal S, et al. Language Mapping Using T2-Prepared BOLD Functional MRI in the Presence of Large Susceptibility Artifacts—Initial Results in Patients With Brain Tumor and Epilepsy. Tomography. 2017;3(2):105-113. doi:10.18383/j.tom.2017.00006
6. Agarwal S, Hua J, Sair HI, et al. Repeatability of language fMRI lateralization and localization metrics in brain tumor patients. Hum Brain Mapp. 2018;39(12):4733-4742. doi:10.1002/hbm.24318
7. Miao X, Wu Y, Liu D, et al. Whole-brain functional and diffusion tensor mri in human participants with metallic orthodontic braces. Radiology. (in press)
8. Zaca D, Hua J, Pillai JJ. Cerebrovascular reactivity mapping for brain tumor presurgical planning. World J Clin Oncol. 2011;2(7):289. doi:10.5306/wjco.v2.i7.289
9. Urback AL, MacIntosh BJ, Goldstein BI. Cerebrovascular reactivity measured by functional magnetic resonance imaging during breath-hold challenge: A systematic review. Neurosci Biobehav Rev. 2017;79(April):27-47. doi:10.1016/j.neubiorev.2017.05.003
Figures